

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Injuries to the glenoid labrum can occur anywhere around the labrum. They may involve only the anterior or anteroinferior portion, as seen in a Bankart and anterior labral periosteal sleeve avulsion (ALPSA) lesions, the posteroinferior area (Kim's lesion), or the superior labrum from anterior to posterior (SLAP) lesions. SLAP lesions were first classified by Snyder et al.1) into 4 subtypes. However, more extensive labral tears do occur, some of which may be progression of pre-existing SLAP lesions, or its combination with a Bankart lesion (SLAP type V).23)
A Bankart lesion is the primary pathology in posttraumatic anterior shoulder instability4) and is present in over 90% of traumatic anterior shoulder dislocation.56) A concomitant SLAP lesion occurs in up to 22% of anterior instabilities,17) the presence of which greatly increases shoulder instability.8910) As such, it has been suggested that more extensive lesions are a result of an increased number of dislocations and treatment of both lesions is imperative to restore joint stability.34511)
However, this is not always true since extensive lesions have been noted with a low number of dislocations in the presence of a high-energy trauma.1213) As such, other authors believe that reattachment of the concomitant SLAP lesion depends on the age and functional demands of the patient, noting that biceps tenodesis or tenotomy had varied results. Most studies claim that there is no significant difference in the range of motion (ROM), functional scores, and recurrence rates when compared to patients who underwent Bankart repair alone;8141516) however, a number of authors have noted several limitations of ROM, especially in external rotation, among those who underwent the combined procedure.817)
To investigate these problems further, the authors compared the clinical characteristics of patients who had anterior shoulder instability with and without SLAP lesion. In addition, we analyzed the effect of concomitant SLAP repair on surgical outcome after arthroscopic stabilization of anterior instability. We hypothesized that anterior shoulder instability with SLAP lesion would be related to high-energy trauma or more episodes of dislocation compared to shoulder instability without SLAP lesion, and that shoulder ROM will decrease after combined arthroscopic anterior capsulolabral reconstruction and SLAP repair, resulting in poorer clinical outcomes.
METHODS
Inclusion and Exclusion Criteria
The study was approved by the hospital's Institutional Review Board (IRB number: B-1407/258-108) and we retrospectively reviewed the prospectively collected data of patients who underwent arthroscopic anterior capsulolabral reconstruction in the senior author's institution between January 2004 and March 2013 and included those who met the following criteria: (1) had posttraumatic anterior instability and (2) were available for follow-up for at least 1 year after surgery. We excluded patients with previous stabilization procedures performed by another surgeon, multiple surgeries due to recurrent dislocations, biceps tenotomy or tenodesis, and detached SLAP lesions that were not repaired because the lesions were asymptomatic, or had no physical findings regarding SLAP lesions. Patients with humeral avulsion of glenohumeral ligament or bony Bankart lesions exceeding 20% of the glenoid were also excluded.
A total of 198 patients underwent arthroscopic stabilization for anterior shoulder instability during the indexed period and 120 (61%) were available for functional assessment at least 1 year after surgery. We divided the patients into 2 groups according to the presence of SLAP lesion. All SLAP lesions were type II (63.6% of type V) by Snyder's classification.1) There were 44 patients (36.7%) with reparable concomitant detached SLAP lesions (group I) and 76 patients (63.3%) without (group II); patients in group II served as the control population. Hand dominance, level of sports activity, and presence of a high-energy trauma were evaluated together with the population demographics. Injuries sustained through sports or falls from a height, thus causing forceful abduction and external rotation, traction, forceful hyperextension, or resulting in direct blows to the shoulder were considered high-energy trauma.
Range of Motion Evaluation and Functional Outcome Assessment
Range of external rotation in 0° and in 90° of abduction was measured using a goniometer. Internal rotation at the back was assessed with the patients sitting upright and their hands placed at their backs as high as possible. Anatomic reference points were the inferior border of the scapula for the seventh thoracic vertebra (T7) and the highest point of the iliac crest for the fourth lumbar vertebra (L4). For ease of statistical analysis, the vertebral levels were converted into numeric values as follows: T1-12 to 1-12, L1-5 to 13-17, and sacrum to 18.
Functional outcomes were evaluated using the Rowe score, wherein lesser scores denote worse shoulder condition. The visual analogue scale (VAS) for pain was used to grade the pain suffered by the patient, with 0 being no pain and 10 being the worst pain experienced. Patient satisfaction with regard to the surgical outcome and improvement was also rated using the VAS, with 10 being the best score.
The ROM and functional outcome measurements were evaluated during preoperative admission, 6 months and 1 year postoperatively, and annually thereafter. The scores and ranges of motion at the final follow-up visit were used for the statistical analysis.
Surgical Procedure
All patients underwent arthroscopic surgery performed by the senior surgeon. Anterior shoulder stabilization consisted of a Bankart or ALPSA lesion fixation with capsular plication, with or without a rotator interval (RI) closure. Additional RI closure using additional suture anchor was confined to patients who demonstrated definite sulcus sign with shoulder in the external rotation position. A concurrent SLAP lesion was repaired between the 10- to 12-o'clock positions on a right shoulder, to avoid anterior labral and capsular plication at the 12- to 2-o'clock positions.
We used the lateral decubitus position for the shoulder arthroscopy with the operated arm pulled by a traction device (ACUFEX; Smith & Nephew, Andover, MA, USA) with approximately 4 kg of weight (10 lb). During anterior capsulolabral reconstruction, an additional lateral traction device was applied for lateral pulling of the arm to obtain easy access to the anterior compartment of the glenohumeral joint. Diagnostic arthroscopy was performed throughout the standard posterior portal as the viewing portal, and an anteroinferior portal as the primary working portal. After overall examination of the glenohumeral joint, the additional anterosuperior portal was used as the secondary working portal for procedures on the anterior labrum or capsule.
For Bankart repair or anterior capsular shift, the abnormally attached labrum or anteroinferior glenohumeral ligament was mobilized from the glenoid neck, then 2- to 3-mm wide subchondral bone was exposed using a motorized burr for the recipient bed. The capsule together with the anterior labrum, when present, were sutured and tacked down using 3 or 4 evenly spaced suture anchors (BIOKNOTLESS; Depuy Mitek Inc., Raynham, MA, USA) between the 2- to 6-o'clock positions, on the right shoulder.
For repair of a SLAP lesion, we used the trans-rotator cuff portal, as described by O'Brien et al.18) and Oh et al.19) to achieve the appropriate angle for anchor insertion. After preparation of the subchondral bone of the superior glenoid rim, 1 to 2 anchors (BIOKNOTLESS) were used for repair of the superior labrum in most cases. To prevent postoperative external rotation limitation, we did not fix the anterosuperior labrum (1- to 2-o'clock position), and released the superior and posterosuperior capsule after fixation of SLAP lesion.
Postoperative Rehabilitation
A standardized rehabilitation protocol was applied to all patients. Immobilization neutral rotation with an abduction pillow was maintained for 6 weeks. ROM exercises were initiated at 6 weeks after surgery and the brace was discontinued. Muscle-strengthening exercises commenced 3 months after surgery, and were continued until at least 6 months postoperatively. Return to sports was permitted 6 months after surgery.
RESULTS
Demographics
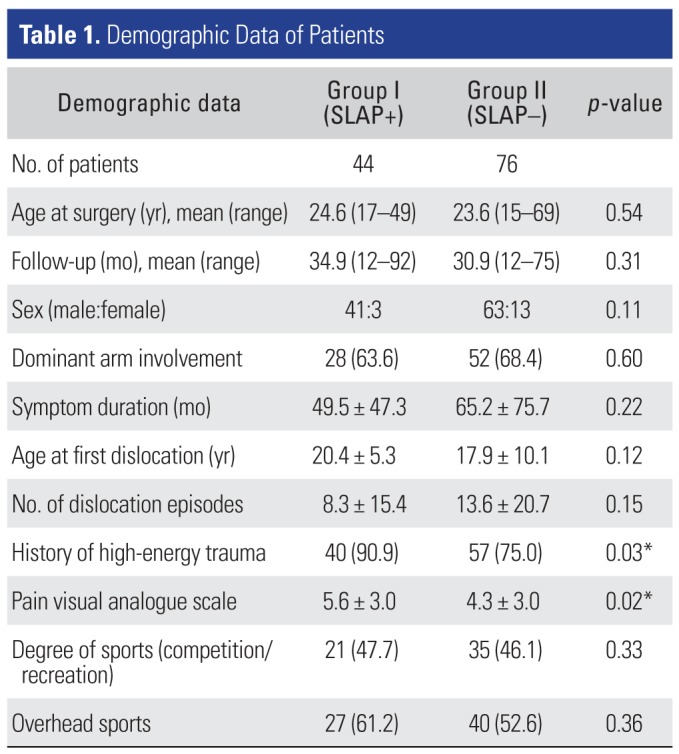
A total of 120 patients were included in the study (Table 1). The mean age of the patients was 24 years (range, 15 to 69 years), with a mean follow-up of 32.3 months (range, 12 to 92 months). There were 104 males and 16 females.
In group I, there were 41 males and 3 females, with an average age of 24.6 years (range, 17 to 49 years). The dominant shoulder was involved in 28 patients (63.6%). The mean symptom duration was 49.5 months before surgery, with a mean pain VAS of 5.6. A history of high-energy trauma to the affected shoulder was noted in 40 patients (90.9%), and there was an average of 8.3 dislocations per shoulder. Twenty-seven patients engaged in overhead sports and 21 were involved in competition-level sports.
In group II, there were 63 males and 13 females, with an average age of 23.6 years (range, 15 to 69 years). The dominant shoulder was involved in 52 patients (68.4%). The mean symptom duration was 65.2 months before surgery, with a mean pain VAS of 4.3. A history of high-energy trauma to the affected shoulder was noted in 57 patients (75.0%), and there was an average of 13.6 dislocations per shoulder. Forty patients engaged in overhead sports and 35 were involved in competition-level sports.
Patients with anterior instability and detached SLAP lesion (group I) had a significantly higher incidence of high-energy trauma (p = 0.03), and patients in group II had a younger mean age of dislocation, longer symptom duration and more episodes of dislocation; however, these were not significantly different from group I (p = 0.12, p = 0.22, and p = 0.15, respectively).
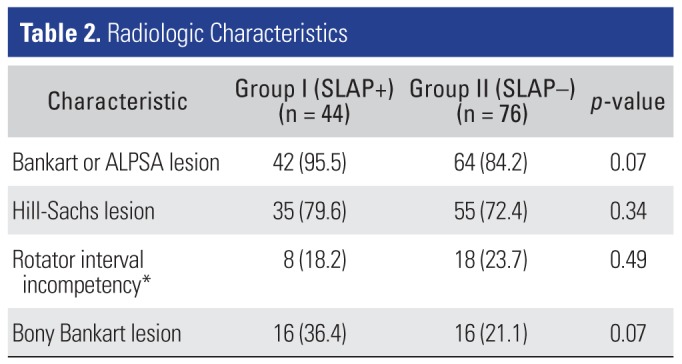
A Bankart, ALPSA, or bony Bankart lesion was encountered marginally, more frequently in patients with detached SLAP lesion, while there were a greater number of patients with RI incompetency in SLAP-negative patients, but the difference was not significant (p = 0.49) (Table 2).
Evaluation of Clinical Outcomes
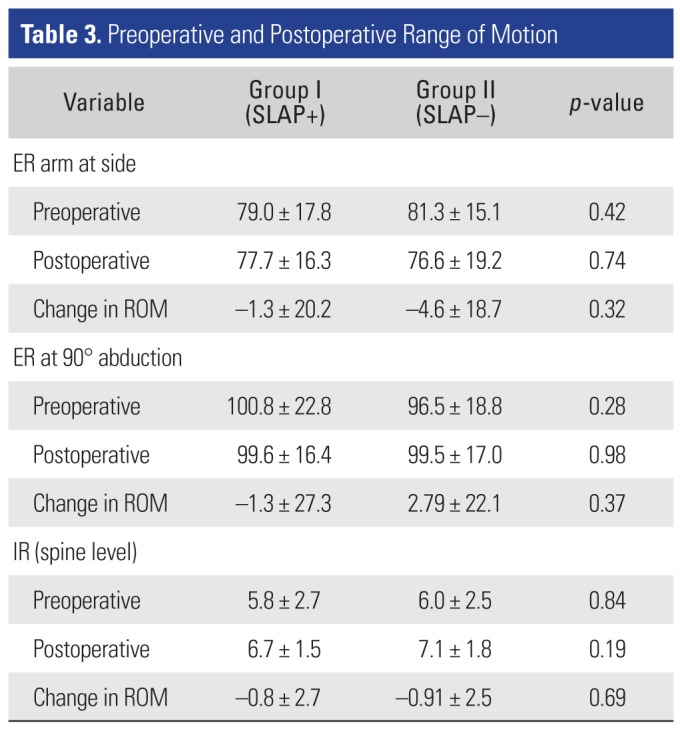
Preoperative shoulder external rotation in 90° abduction and internal rotation were better in group I than in group II, though the differences were not significant (p = 0.28 and p = 0.84, respectively). Generally, there was noted limitation in all ROMs in group I postoperatively, but the changes in ROM were not significantly different than those observed in group II (Table 3).
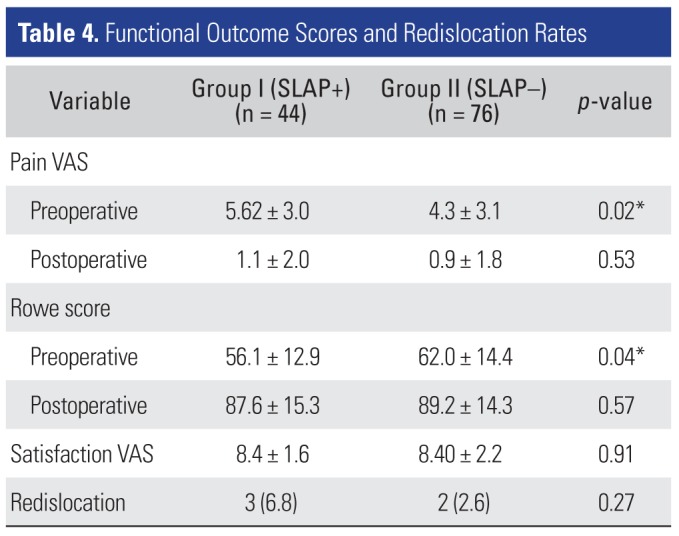
Group I patients had higher pain VAS (p = 0.02) and lower Rowe (p = 0.04) scores preoperatively, as compared to those in group II (Table 4). The pain VAS and function scores of both groups improved postoperatively. Both groups were equally satisfied with their condition (p = 0.91) and the redislocation rate was similar (p = 0.27).
DISCUSSION
In the current study, patients with anterior instability and detached SLAP lesion had a significantly higher incidence of high-energy trauma (p = 0.03). However, the mean age at the first dislocation, symptom duration before surgery, and the number of dislocations were not significantly different between the 2 groups. Involvement of the dominant arm was similar in both groups, as were the degree of sports and participation in overhead sports. On the whole, patients in group I suffered more pain, had more difficulties in performing daily activities, perceived a more unstable shoulder, and were more dissatisfied with their shoulder condition, as evidenced by higher pain VAS (p = 0.02) and lower Rowe (p = 0.04) scores preoperatively.
Patients in group II had a younger mean age at dislocation, longer symptom duration and more episodes of dislocation; however, these were not significantly different from group I (p = 0.12, p = 0.22, and p = 0.15, respectively). Bony and soft tissue injuries were more severe in patients with SLAP lesion, group I, which suggests that instability with SLAP lesion may be related not to the chronicity or frequency of shoulder dislocation but to the presence of high-energy trauma.
Several studies have noted that patient age at the time of first dislocation greatly influences the subsequent number of dislocations and have suggested that an increased number of dislocations creates more-severe labral tears.1520) Younger age and longer time from initial injury to surgery contribute to the propagation of the injuries, which in turn worsens the present instability.45) However, recent investigations have reported that a history of high-energy trauma to the involved shoulder may also account for extensive lesions and severe instability even after a single dislocation. Kim et al.13) reported that 68.7% of patients with fewer than five dislocations had extensive circumferential labral lesions. Likewise, radiologic evaluation of shoulder dislocation patients showed superior labral involvement in 39% of patients with a single episode.12) In the current study, we observed that patients with a combined anterior instability and detached SLAP lesion had significantly higher incidence of high-energy trauma (p = 0.03) and fewer episodes of dislocation (p = 0.15). This suggests that the severity of the lesions may not be secondary to progression of a simple injury; rather, it was a result of the initial trauma. As such, this supports our hypothesis that anterior shoulder instability with SLAP lesion is related to high-energy trauma.
Preoperative pain VAS and Rowe scores were significantly worse in patients with SLAP lesions, despite having fewer dislocation episodes. The current findings are in accordance with those of Kim et al.13) who reported that patients with more severe labral lesions had worse preoperative pain VAS and functional scores and consulted sooner than those with only a Bankart or ALPSA lesion, most likely because of the more severe pain and limitation of activity of daily living. Postoperatively, their patients had similarly improved ROM and shoulder scores, despite the degree of injury and extent of repair. These are consistent with previous reports that the functional outcomes of patients with combined lesions are not dependent on concomitant SLAP repair.15) Therefore, we ascertain that SLAP repair combined with an anterior stabilization procedure does not lead to poor functional outcomes if appropriate surgical procedures and methodical postoperative rehabilitation are performed.
The objective of surgical management is to provide adequate joint stability, pain relief, and shoulder ROM comparable to the preinjury level so that the patient may return to his or her preinjury status. The basic tenet in the treatment of anterior shoulder instability is to recognize that surrounding structures, aside from the Bankart lesion, contribute to the pathology. Fixation of both the Bankart lesion and symptomatic SLAP lesion has been advocated by some authors, since fixation of only one would still result in residual instability in some cases.31121) A biomechanical study of SLAP repair showed that, when all other structures in the joint are intact, a SLAP repair alone helps to normalize the glenohumeral translation. However, when there was an additional pathology, the repair was rendered ineffective.22) Another cadaveric study by Mihata et al.10) investigated the effect of combined type II SLAP lesions with anterior capsular laxity, as would be seen in throwing athletes. They noted increased external rotation and anterior glenohumeral translation after simulation of anterior capsular laxity and type II SLAP lesion. After arthroscopic repair of the SLAP lesion alone, there was a significant decrease in the external rotation; however, this did not fully restore anterior glenohumeral translation.10) As such, most authors would recommend fixation of both lesions to restore primary shoulder stability, which is essential to allow postoperative rehabilitation, while preventing residual laxity. Furthermore, repair of the SLAP lesion, especially in younger and more active patients, promoted return to overhead sports, and good outcomes can be achieved with appropriate treatment.1623) However, concerns regarding limitation of shoulder motion secondary to over-tightening of the capsulolabral complex or over-treatment have been raised. Postoperative decrease in shoulder ROM may be expected in most procedures and a decrease specifically in external rotation has been noted to occur, especially after combined anterior shoulder stabilization and SLAP repair.1418)
Although recovery of shoulder ROM may be slower in this subset of patients, no difference was noted in the final ROM after 1 year. In the current study, the surgical technique for anterior capsulolabral reconstruction was identical in both groups. For the concurrent SLAP repair, we repaired between the 10- to 12-o'clock positions on a right shoulder and avoided anterior labral and capsular plication at the 12- to 2-o'clock positions. This fixation was firm and stable, and at the same time, provided some slack to the biceps anchor to maintain some external rotation. After fixation of SLAP lesions, authors always also release the superior and posterosuperior capsule. As such, we did not observe a significant decrease in external rotation in our patients with combined labral lesions. While there was indeed a decrease in the ROM at final follow-up, this was not different from the final ROM of the patients without SLAP lesions. Therefore, care should be taken during the surgery to preserve postoperative external rotation.
There are some limitations to be mentioned in the present study. First, the natural history of untreated asymptomatic SLAP lesions and their possible effect on the patient outcomes is unclear. Patients with anterior shoulder instability with asymptomatic detached SLAP lesions and those who underwent biceps tenodesis with anterior stabilization procedures instead of SLAP fixation should also be evaluated. Second, high-energy trauma is a somewhat vague and subjective experience. However, we confined high-energy trauma if shoulders were dislocated after a forceful traumatic event, such as vehicle accident, fall with outstretched hand and so on. Third, the number of subjects was limited and the length of follow-up in this retrospective study was relatively short. Also, the high rate of patients lost to follow up could pose a risk of type I error. A prospective study with mid-term follow-up would facilitate determination of differences in patient performance and return to sports between the 2 groups.
In conclusion, the extent of labral lesion was not dependent on the number of preoperative dislocations, but related to the amount of energy exerted during the initial dislocation. Our findings show that combined arthroscopic anterior capsulolabral reconstruction and additional fixation of SLAP lesion can yield good to excellent functional outcomes, if appropriate surgical procedures are conducted, such as saving anterosuperior labral fixation and superior and posterosuperior capsular release after SLAP fixation.
 XML Download
XML Download