

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Benign bone tumors are seldom aggressive, but grow rapidly. They can be treated by curettage or a simple lesion resection and consequently, there are few cases of reconstruction. However, some benign bone tumors, like giant-cell tumors, must be resected in order to provide a safe margin to prevent local recurrence. This causes a loss of bone stock, and therefore, reconstruction is required.
Distraction osteogenesis with the Ilizarov apparatus is widely used for the treatment of several orthopedic problems, such as leg length discrepancy (LLD), deformity, osteomyelitis, and congenital or acquired skeletal defects.1,2,3) Recently, it has also been used for the treatment of bone defects caused by trauma4,5) and bone tumor resection.6,7)
The aim of this study was to assess the results and the indication of treating bone defects in patients with benign bone tumors through bone transport using the Ilizarov apparatus.
METHODS
Between 1997 and 2006, seven patients (six males and one female) with benign bone tumors were treated with bone transport using the Ilizarov apparatus in our institution. Their mean age at surgery was 14.4 years (range, 4.8 to 36.9 years) and the mean follow-up period was 106.2 months (range, 34.6 to 180.5 months).
The histological diagnoses included four cases of osteofibrous dysplasia, one giant-cell tumor, one intraosseous cavernous hemangioma, and one aneurysmal bone cyst. The lesions were located in the proximal tibia in two cases, the tibial shaft in three cases, and the distal femur in two cases (Table 1). The mean defect ratio was calculated using the corticotomy method; dividing the affected long bone length by the length of the defect.
Bifocal bone transports were performed in six cases, and a trifocal bone transport was performed in the remaining cases. Bone transport with diaphyseal reconstruction was performed in five cases (tibia), and shorteningdistraction with metaphyseal reconstruction was done in two cases (distal femur). The reconstruction procedures were classified via distraction osteogenesis.8)
The distraction was started after a latent period of 8.6 days,6,7,8,9,10,11) the distraction rhythm was set at four times, and the length was 0.5 or 1 mm per day. The distraction settings were adjusted according to the quality of bone formation as seen in the serial radiographs during follow-up. Partial weight-bearing was allowed after the full length was reached, and the external fixator was removed after sufficient cortex development had been observed.
We used three indices for evaluating the results: the external fixation index, which was obtained by dividing the duration of external fixation by the length of bone regeneration; the distraction index, which was obtained by dividing the duration of distraction by the length of bone regeneration; and a maturation index, which was obtained by dividing the duration of external fixation, measured from the completion of distraction to the removal of external fixation, by the length of bone regeneration.
RESULTS
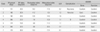
The mean length of the defect after tumor resection was 7.3 cm (range, 5.1 to 12.1 cm) and the mean defect ratio was 22.1% (range, 12.9% to 52.4%), which is shown in Table 1. The length of distraction was determined by the patient's age, bone age, and unaffected limb length. The mean length of distraction was 6.9 cm (range, 4.9 to 11.0 cm). The external fixation was applied at 185.6 days (range, 106 to 266 days). The mean external fixation index was 26.0 day/cm (range, 19.8 to 32.5 day/cm), the distraction index was 9.6 day/cm (range, 6.8 to 12.0 day/cm) and the maturation index was 14.9 day/cm (range, 8.0 to 22.5 day/cm) (Table 3). All the patients were able to perform their daily activities without problems. The bone and functional results were rated excellent in six cases and good in one case. The radiographs of representative cases are shown in Figs. 1,2,3.
There were complications in three patients, including pin tract infection, local recurrence, and nonunion. The pin tract infection was treated successfully with oral antibiotics for one week. One patient had local recurrence of the tumor due to an insufficient resection. The patient was subsequently treated with a tumor resection and a fibular autogenous bone graft. Nonunion occurred in one patient and was treated by osteosynthesis with a fibular autogenous bone graft. There was no instance of LLD over 3 cm shortening (mean, 1.1 cm; range, 0.1 to 2.7 cm) at the final follow-up.
DISCUSSION
Bone defects are a common orthopedic problem, resulting from trauma or malignant or benign bone tumors. Malignant bone tumors can lead to bone defects, soft tissue defects, and limb length discrepancy after a surgical resection. After the malignant bone tumor is resected, there are many modalities of treatment to reconstruct the defect, including allografts, autoclaved autografts, vascularized fibular or iliac bone grafts, irradiated bone grafts, prosthesis, and distraction osteogenesis.6,7,10,11) Each technique has its own advantages and disadvantages.
Allografts are a commonly used technique for the reconstruction of bone defects after tumor resections. The technique is beneficial because of biology and the graft is customized to the proper size and form. However, there are also some disadvantages, including the potential transmission of a disease, allograft rejection, late fracture, infection, and nonunion.
For this reason, autogenous bone grafts are also commonly used for reconstruction. There are advantages to this solution, such as the capability to cover long defect lengths, a resistance to infection, and its biological properties. Laffosse et al.12) reported in a study of 13 patients with long bone defects that autologous vascularized fibular graft treatment yielded good union results. However, there are some disadvantages, including the fact that it is a technically demanding procedure, takes a long time, graft fracture, nonunion, and size limitations.
Prosthetic replacement is a useful reconstructive method after resection a malignant bone tumor, but there are few reports of its use in benign bone tumors. Shin et al.13) reported that prosthetic replacements for aggressive benign bone tumors are a good treatment option for reconstruction of the bone defect. However, late complications such as infection, loosening, and breakage are common and troublesome.
Recently, distraction osteogenesis using external fixation has been reported as a management technique for posttraumatic bone defects4,5) and bone defects after malignant tumor resection.6,7) There are many advantages to this technique, such as biomechanical stability, a bloodless technique, regeneration of new bone, and a gradual lengthening of the soft tissues.14) Therefore, we tried to use the bone transport technique with the Ilizarov apparatus to reconstruct bone defects after resecting benign bone tumors and saw good results.
Karita et al.15) treated two patients with osteofibrous dysplasia using en bloc marginal excision of the lesion and bone transport, a distraction osteogenesis procedure. They reported good results and recommended the treatment as a way to reconstruct large bone defects after tumor resection.
Tsuchiya et al.14) also reported good functional results in 10 patients with benign bone tumors of the extremities that were treated by resecting the tumor and reconstructing with external fixation. They recommended an Ilizarov frame or Taylor spatial frame instead of unilateral fixators because limb-length discrepancy and deformity can be treated simultaneously with these frames. In this study, we use an Ilizarov apparatus for reconstruction in all cases.
The mean defect ratio was 17.1% (range, 12.9% to 21.9%), except for one outlier with the largest defect (52.4%). It is not the same condition in children because the total limb length is shorter than in adults. We used the trifocal bone transport in one case and its defect ratio was 52.4%. Trifocal bone transport is used in cases of longer defects as compared to bifocal bone transport.16) If we use the trifocal bone transport when there is a large defect ratio, we can shorten the period of treatment. But, we only have one such case, so we cannot make conclusions about the indication of trifocal bone transport. Thus, more research about the correlation between the defect ratio and bifocal or trifocal bone transport is needed. The most common complication of external fixation is a pin track infection. In our cases, one case had a pin track infection that was managed by oral antibiotics.
Nonunion or refracture are not rare. The external fixation period is important for healing distracted bones because it promotes stability and maturation. We had one case of nonunion and reviewed the maturation index. The mean maturation index was 14.9 day/cm but only 8.0 day/cm in the case of nonunion. If the duration of the external fixator is too short, the limited maturation time can lead to the instability of the distracted bone, causing nonunion or refracture. Therefore, it is important that external fixation is maintained for maturation of distracted bone. Also Green et al.17) recommended bone grafting at the docking site in order to shorten the period of treatment and promote the rate of union formation. In our cases, we did an autogenous bone graft at the docking site in all cases and all but one case achieved a union.
The mean LLD was 1.1 cm at last follow-up. The case of the longest length discrepancy is a pathologic fracture with an aneurismal bone cyst in the distal femur. The lengthening after shortening was done, but we could not get a full lengthening because of leg pain. In the other cases, lengthening was stopped after correction of LLD. The residual LLD was caused by stopping the lengthening early and occurred during growth. Long periods of external fixation can be uncomfortable for the patient. Today, we can shorten the period of external fixation by converting to internal fixation.18,19) Internal fixation greatly reduces the patient's time in external fixation during the consolidation phase, gives additional stability to protect the tibia against refracture, and is expected to prevent nonunions.
Bone transport using the Ilizarov apparatus is a good treatment option in patients with bone defects after resection of a benign bone tumor. It offers a good alternative to other conventional methods. Furthermore, bifocal or trifocal osteotomies can be used to reconstruct large bone defects. Some complications such as a pin track infection, nonunion, and local recurrence still need to be addressed.
Bone transport is only indicated in limited cases, not in all benign bone tumors. We think this is the most suitable course of treatment for active or aggressive benign bone tumors where a large bone defect is expected, but more study is needed.




 XML Download
XML Download