

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Internal snapping hip syndrome is a condition produced by the iliopsoas tendon snapping over the iliopectineal eminence or the femoral head. This condition is caused by hypertrophy or hyperactivity of the iliocapsularis, chronic inflammation of the iliopsoas tendon and bursa, overhanging acetabular cup, abnormal angulation of the tendon, a large femoral head, and high femoral anteversion.1,2,3,4)
Internal snapping hip syndrome may occur without pain in up to 10% of the general population.5) However, when symptomatic, surgical treatment may be indicated. Open surgical release of the iliopsoas has been reported by several authors for the treatment of internal snapping hip syndrome.1,6,7) The approach can be moderately successful, although a 40% complication rate was reported.8)
Advances in arthroscopic techniques and instruments have included arthroscopic iliopsoas tendon release.9,10,11,12) It is our experience that patients with symptomatic internal snapping hip frequently have concomitant hip pathology including femoroacetabular impingement and labral tears. However, most reported studies have focused on the surgical technique and the result of focused isolated treatment of internal snapping hip.
The purpose of this study was to evaluate concomitant hip pathology in patients with painful internal snapping hip and the clinical outcomes of arthroscopic iliopsoas tendon surgery after a minimum follow-up of 2 years. The study hypothesis is that arthroscopic iliopsoas tendon release can provide good clinical outcomes in patients with painful internal snapping hip and concomitant intracapsular hip pathologies.
METHODS
Between January 2009 and December 2011, we performed arthroscopic iliopsoas tendon release in 25 patients followed up for a minimum of 2 years postoperatively. The indications for surgery were an audible and painful popping sound of the iliopsoas attachment area and intractable pain after preoperative conservative treatment, manifest as limitation of patient's activity, physical therapy, and/ or the need for medications and injections for at least 12 weeks. On physical examination, all patients had a painful range of motion and a positive impingement test (flexion, adduction, and internal rotation). Preoperative imaging included plain radiographs (pelvis anteroposterior and frog leg) and computed tomography arthrogram or magnetic resonance arthrogram to detect bony impingement and labral lesons. Patients who had undergone previous hip surgery, and who had avascular necrosis, rheumatologic disorder, and arthritis more severe than Tonnis grade 2 were excluded.
The 25 patients comprised 20 men and 5 women, with a mean age of 32 years (range, 17 to 53 years). Preoperative diagnoses included internal snapping hip with isolated labral tear in 6 hips, cam-type impingement in 14 hips, pincer-type impingement in 3 hips, and mixed type in 2 hips. Preoperative radiographs revealed Tonnis grade 0 to 1 changes in 23 hips and grade 2 changes in 2 hips (Table 1). During surgery, all patients had ilipsoas tendon release combined with another procedure; arthroscopic femoroplasty with labral repair was performed in 16 patients, chondroplasty in 3 patients, and labral repair or debridement in 6 patients.
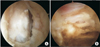
Arthroscopy was performed with the patient supine on a fracture table, with the post for counter-traction in the central position and a well-padded foam cushion in place to protect against any nerve compression. The arthroscope was initially inserted through a posterolateral portal in all cases. Anterior and anterolateral portals were used as necessary. Complete inspection of the central compartment was performed, with care to evaluate for the presence of injury to any part of the labrum, articular cartilage damage, or pincer lesion. In cases with a tear of the labrum, the torn portion was debrided using the shaver or reattached using suture anchors. The traction was released and the peripheral compartment entered via anterolateral and anterior portals with the hip in 30° flexion to open the space anteriorly over the hip. For exposure of the tendinous portion of the iliopsoas, further capsulotomy was made anterior to the labral injury using the shaver or radiofrequency ablation device. A 30° arthroscope was introduced into the anterolateral portal aiming caudally and set on the femoral head-neck junction. With the arthroscope pointing toward the anterior capsule, an electrocautery device was introduced from the anterior portal. An 8-mm transverse capsulotomy was made just lateral to the medial synovial fold and just proximal to the zona orbicularis anteriorly, directly under the iliopsoas tendon.13) Through this capsular window, the tendinous portion of the iliopsoas could be visualized (Fig. 1). The shaver was used to peel any adherent portions of the iliopsoas off of the capsule. The tendinous portion of the iliopsoas was then incised through an anterior portal from medial to lateral using arthroscopic electrocautery (Fig. 2). Careful attention was paid to avoid damage to any of the nearby neurovascular structures (Supplement 1  ). The surgery was completed with a thorough inspection of the peripheral compartment with care to note the presence of a cam lesion or capsular-sided labral abnormality. The operation was completed by joint lavage and injection with a local anesthetic. Postoperatively, all patients followed a standardized rehabilitation program.
). The surgery was completed with a thorough inspection of the peripheral compartment with care to note the presence of a cam lesion or capsular-sided labral abnormality. The operation was completed by joint lavage and injection with a local anesthetic. Postoperatively, all patients followed a standardized rehabilitation program.
). The surgery was completed with a thorough inspection of the peripheral compartment with care to note the presence of a cam lesion or capsular-sided labral abnormality. The operation was completed by joint lavage and injection with a local anesthetic. Postoperatively, all patients followed a standardized rehabilitation program.Clinical and radiographic follow-up evaluations were performed at 6 weeks, 3, 6, and 12 months, and every 6 months thereafter. Patients that did not attend regularly scheduled visits were contacted by telephone.
Clinical evaluations were performed using the Harris hip score (HHS),14) visual analog pain score (VAS), hip outcome score (HOS)-activities of daily living subscale and HOS-sports subscale. Radiographic analysis included anteroposterior view of the pelvis, frog-leg lateral view, and cross-table lateral view of the hip. All radiographs were assessed using the Tonnis classification15) to grade radiographic degenerative changes and the Outerbridge classification system16) that grades according to the degree of chondromalacia.
The difference between preoperative and postoperative outcome measures were analyzed using Wilcoxon signed rank test for continuous outcome measures and Fisher exact test for categorical outcome measures. The null hypotheses of no difference was rejected if p-values were < 0.05. Statistical analyses used SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA).
The design and protocol of this retrospective study were approved by the Institutional Review Board of Chung-Ang University Hospital, Seoul, Korea.
RESULTS
Clinical Outcome
Snapping sounds and pain had disappeared at the 2-year follow-up in 24 of the 25 patients. During follow-up, significant loss of flexion strength in all patients was present after surgery but improved by 6 to 10 weeks. The overall rating for the 25 patients (25 hips) using the HHS was 65 points (range, 46 to 86 points) preoperatively and 84 points (range, 67 to 98 points) postoperatively (p < 0.001). Seven hips (28%) had an excellent score, 15 hips (60%) a good score, 2 hips (8%) a fair score, and one hip (4%) a poor score. The HOS-activities of daily living subscale and HOS-sports subscale preoperatively were 66% and 60%, respectively. The score changed to 87% and 82%, respectively, at the final follow-up evaluation. University of California, Los Angeles (UCLA) activity at the latest follow-up was improved in 17 patients and remained the same in 8 patients. The mean VAS score decreased from 6 to 2 at the latest follow-up.
Radiologic Outcome
Five patients had an Outerbridge grade III articular cartilage lesion of the acetabulum at the time of the surgical exploration. The Tonnis grade of osteoarthritis did not change in any of the patients at the last follow-up.
Complications
Although significant complications such as infection, heterotopic ossification, thromboembolic episode or permanent nerve injury did not occur, one patient had a reoperation because of recurred painful snapping hip 3 days postoperatively. The patient did not experience further recurrence throughout the 2-year follow-up. One patient experienced a recurrent audible sound at the 1-year postoperative follow-up. However, the clinical symptoms were much improved at the last follow-up.
DISCUSSION
Good-to-excellent clinical outcomes after arthroscopic release of internal snapping hip have been reported since the year 2000. However, most of the reported studies have focused on the surgical techniques used and the clinical outcomes of isolated internal snapping.9,10,11,17) This study was done to evaluate clinical outcomes after combined arthroscopic iliopsoas tendon release and other arthroscopic procedures in patients with internal snapping and other intracapsular pathologies. Twenty-four of 25 patients experienced disappearance of the snapping sound and 22 patients (88%) had scores indicating excellent and good responses over the minimal 2-year follow-up period (Table 2).
In 2006, Ilizaliturri et al.10) performed arthroscopic release of the iliopsoas tendon in 7 hips. They reported that the snapping symptoms disappeared in all patients over the average 21-month follow-up period and significant loss of flexion strength was present after surgery but had improved by 8 weeks. In 2009, Ilizaliturri et al.11) performed a prospective randomized study of two different techniques for endoscopic iliopsoas tendon release in 19 patients. The Western Ontario and McMaster Universities (WOMAC) scores in both groups improved without complications. Flanum et al.18) reported all 6 patients in the case series reported no recurrence of their snapping or pain at the last follow-up. Our findings are consistent with those of the previous three studies.
The aforementioned three studies focused only on the snapping symptoms and pain. However, in this study, all patients had combined internal hip pathologies such as labral tear (6 patients) and femoroacetabular impingements (19 patients). Domb et al.12) performed arthroscopic iliopsoas tendon release in 25 patients. They observed anterior labral tears at the 3 o'clock area and suggested that iliopsoas impingement is one of the causes of labral tear in the hip. Fabricant el al.17) evaluated the clinical outcomes of 67 patients with internal snapping hip who underwent arthroscopic psoas tendon lengthening. Thirty-seven of these patients had combined structural pathologies. Also, increased femoral anteversion was reported as a risk factor for inferior clinical outcomes after arthroscopic lengthening for symptomatic internal snapping hip. Patients with internal snapping hip might have combined hip pathologies. However, during open surgical treatment of internal snapping hip, it may be difficult to evaluate and treat combined internal hip pathologies such as structural bony abnormalities, labral tear, and femoral anteversion.12,17) Recently, Khan et al.19) performed a systemic review using 11 eligible studies. They reported that arthroscopic surgery for internal snapping hip syndrome showed a decreased failure rate, fewer complications, and decreased postoperative pain in comparison with open management.19) A possible reason for the better outcomes after arthroscopic iliopsoas tendon release is that combined intraartcular hip pathologies can easily be treated during this procedure. We think that clinical outcomes after iliopsoas tendon release might be related to the treatment of combined hip pathologies.
The medial femoral circumflex artery is close to the psoas tendon.20) Theoretically, there is a risk of osteonecrosis of the femoral head after injury to the medial femoral circumflex artery during arthroscopic psoas tendon release. However, to our knowledge, there has been no report of medial femoral circumflex artery injury during arthroscopic psoas tendon release, and it did not occur in this study.
Presently, rehabilitation after arthroscopic iliopsoas tendon release was delayed and a crutch was needed for a longer time than after typical arthroscopic hip surgery because of loss of flexion strength. Others reported that significant loss of flexion strength was present after surgery but improved by 8 weeks.10) In the present study, all patients who had presented with loss of flexion strength postoperatively showed recovery by week 6 to 10. Therefore, patients should be told about the inevitable loss of flexion strength and the longer rehabilitation period plus the longer period of crutch use that occur after this procedure.
There are several limitations of this study. First, it is a retrospective review of prospectively collected data and no control group was used, it might be hard to know what effect the psoas tendon release had on the overall results. However, we are sure of the reliability of our study because all patients had painful snapping hip and completed the follow-up for the minimum 2-year period. Second, all patients had combined hip pathology. It might be difficult to evaluate the effect of arthroscopic iliopsoas release on internal snapping hip only when there is combined hip pathology. In addition, patients with internal snapping hip should be thoroughly evaluated and a plan made for the treatment of combined pathology such as structural bony abnormalities, labral tear, and femoral anteversion. Dynamic ultrasound is a well-suited, complementary tool for diagnosing snapping hip because of its real-time visualization of the snapping structures. This diagnostic method might be helpful to evaluate painful internal snapping hip. However, dynamic ultrasound technique was not available in this study period.
Patients with painful internal snapping hip have combined hip pathologies. Therefore, the surgeon should keep in mind the possibility that painful internal snapping hips can frequently accompany concomitant intraarticular pathologies.



 XML Download
XML Download