

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In growing children or adolescents, angular deformity of long bones can be corrected by hemiepiphysiodesis or hemiepiphyseal stapling, which take advantage of longitudinal physeal growth.1,2) These physis-manipulating procedures have minimal perioperative morbidity compared with acute correction by osteotomy or gradual correction by distraction osteogenesis. Physeal growth inhibition by epiphyseal stapling is reversible so that physeal growth can be restored if the staples are removed within due time,1,3-5) which makes this technique useful even in young children.
Because hemiepiphyseal stapling basically inhibits physeal growth of the long bone, it is generally considered to shorten the operated limb and to initiate or aggravate leg length discrepancy when the procedure is performed unilaterally. However, correction of an angular deformity might increase effective leg length and improve pelvic obliquity in a standing position6) even though the anatomical leg length decreased to some extent. Therefore, hemiepiphyseal stapling has both positive and negative effects on effective leg length. We mathematically analyzed changes in effective leg length induced by unilateral hemiepiphyseal stapling, and validated the devised formula in clinical cases.
METHODS
Mathematical Analysis
Our mathematical analysis was based on the following assumptions; 1) the unstapled side of the operated physis grows as fast as that of the contralateral limb, and 2) the hinge point of angular correction is located at the perichondrium of the stapled physis. The limb length distal to the stapled physis is represented by L, the width of the stapled physis by d, and the amount of angular deformity to be corrected by θ.
The gain of effective leg length resulting from angular correction can be written as

From the above two trigonometric formulae, the resultant change in effective leg length discrepancy (ΔELLD) is



Validation of the Equation in Clinical Cases
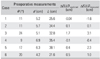
In an attempt to validate this equation, a patient database was reviewed from January 1997 to May 2003, and data on those who fulfilled the following inclusion criteria was retrieved: 1) a unilateral angular deformity around the knee joint, 2) an angular deformity only in the coronal plane, 3) no obvious partial physeal arrest, 4) treated by unilateral hemiepiphyseal stapling, and 5) those who were followed up regularly and whose angular deformity had been corrected completely by hemiepiphyseal stapling. Among the patients satisfying the inclusion criteria, seven patients had complete medical records and radiographs taken before and after the angular correction. Pertinent patient data is summarized in Table 1. Mean age at the time of surgery was 9.7 years (range, 5.8 to 12.8 years). All cases had genu valgum except one with genu varum. The amount of angular deformity to be corrected (θ) was the angle formed between the mechanical axes of the femur and tibia, which averaged 15.3°. The width of the stapled physis (d) and the limb length distal to the stapled physis (L) were measured on a preoperative standing teleradiographs of the lower extremity. Change in effective leg length discrepancy was predicted using equation 1, and denoted as ΔELLDpredicted.
Changes in effective leg length discrepancy were also measured on preoperative and post-correction radiographs, and denoted as ΔELLDmeasured. First we created a line along the mechanical axis of the femur, and we created second line, that was perpendicular to the first line, from the ankle joint center to the first line. The distance from femoral head center to the cross point of the first and second line was defined as the effective leg length (Fig. 1). Preoperative effective leg length discrepancy was measured teleradiographs. Angular correction was considered to be achieved successfully when the mechanical axes of the femur and tibia were co-linear, which took 17.8 months at average (range, 10 to 28 months). Post-correction effective leg length discrepancy was also measured using the same method. ΔELLDpredicted was correlated with ΔELLDmeasured using Spearman's rho correlation coefficient. Significance was set at p < 0.05.
Range of L/d Ratio
In order to determine the range of L/d ratio in growing children, the width of the stapled physis (d) and the limb length distal to the stapled physis (L) were measured on standing teleradiographs of the lower extremities in twenty seven children, who underwent hemiepiphyseal stapling or percutaneous hemiepiphysiodesis to correct angular deformity, including the six cases above. Their ages averaged 11.7 years (range, 6.7 to 15.3 years). Their measurements were merged with those of six patients who fulfilled inclusion criteria. The mean and standard deviation of L/d ratio were calculated in these twenty-seven patients.
RESULTS
Mathematical Analysis Predicting Change in Effective Leg Length Discrepancy
Equation 2 indicates that effective leg length of the operated limb may increase, remain the same, or decrease after angular correction by hemiepiphyseal stapling, according to L/d ratio and θ value (Fig. 2). If a case is plotted above and right to the curve of Fig. 2, hemiepiphyseal stapling will gain effective leg length. On the other hand, if it is plotted below or left to the curve, it will lose effective leg length. With a constant L/d ratio, the larger angular deformity is to be corrected, the more likely is it to increase effective leg length.
Validation of the Equation in Clinical Cases
Table 2 shows the preoperative anatomical parameters and changes in predicted and measured effective leg length discrepancies in 6 cases. Changes in effective leg length discrepancy which were predicted by equation 1 (ΔELLDpredicted) coincided with the actual changes measured on preoperative and post-correction radiographs (ΔELLDmeasured), although the amount of changes was not exactly the same. A significant correlation was found between predicted and measured ΔELLD's with correlation coefficient of 0.823 (p = 0.044).
Range of L/d Ratio
The mean of L/d ratio in twenty-seven children was 4.82 with a standard deviation of 0.51. Range of L/d ratio within 2 standard deviations was from 5.85 to 3.78. Range of value that fulfilled equation 2 with this range of L/d ratio was from 9.9° to 15.6° (Fig. 2).
DISCUSSION
Epiphyseal stapling is well established as a simple and effective means of controlling physeal growth.7-10) By applying staple(s) to one side of the physis angular deformities of a long bone can be corrected. It appears reasonable to conclude that hemiepiphyseal stapling inevitably causes limb shortening because it inhibits physeal growth. This could lead to adopt distraction osteogenesis or open wedge osteotomy instead of hemiepiphyseal stapling in cases with pre-existing limb shortening on the affected side.
The effect of hemiepiphyseal stapling on effective leg length is, however, twofold. The inhibition of physeal growth on the stapled side does decrease long bone longitudinal growth to some extent. On the other hand, a significant portion of the length can be restored by correction of an angular deformity. Gain of effective leg length by acute angular correction has already been well demonstrated.6,11-14) Paley explained the lengthening effect of angular correction in terms of the difference between mechanical and anatomical lengths.15) However, angular correction by hemiepiphyseal stapling is different from acute angular correction in some aspects. As it takes time to obtain the attempted correction, physeal growth during that time should be considered. Depending on the amounts of each of these contradictory effects, hemiepiphyseal stapling can either increase or decrease effective leg length compared with the contralateral side. However, to the best of our knowledge, no systematic analysis of these contradictory effects has been reported that considered physeal growth and its asymmetrical inhibition by hemiepiphyseal stapling.
In the current study, we investigated mathematically the positive and negative effects of hemiepiphyseal stapling on effective leg length. The formula indicates that; a smaller width of the operated physis, a longer distance from the operated physis to the ankle joint, and a larger angular deformity will increase effective leg length of the operated limb. For example, in case 3, which had the largest angular correction, a relatively small physeal width, but a substantial distance between the operated physis and the ankle joint, effective leg length discrepancy improved to a maximal extent in terms of both predicted and measured values (Fig. 3).
Predicted changes in effective leg length discrepancy in the 6 patients concurred with clinical results. However, the amount of changes varied between the predicted and measured values as the assumptions upon which the mathematical model was based are not always satisfied in reality. The unstapled side of the operated physis, which was assumed not to be affected by any pathologic process, may have some functional (though not structural) defect. Moreover, the hinge point of angular correction by hemiepiphyseal stapling is not necessarily at the perichondrium but possibly nearer to the midline of the limb segment. Another source of error for this model is that physeal growth of the unstapled side of the operated physis may also be retarded by hemiepiphyseal stapling to some extent.7,16) If this occurs, it would interfere with the length gain effect and subsequently aggravate the effective leg length discrepancy. Nevertheless, this study revealed that hemiepiphyseal stapling could improve effective leg length in a certain circumstance. As L/d ratio was found to remain in a relatively narrow range, it is largely influenced by the amount of angular correction whether the effective leg length discrepancy will improve or aggravate. Our data suggest that the hemiepiphyseal stapling is likely to lose effective leg length if the amount of angular correction is less than 10°, whereas it is to gain effective leg length if it is larger than 16°. This should be taken into consideration when determining the surgical method for angular deformity correction in skeletally immature patients.




 XML Download
XML Download