

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Core needle biopsy (CNB) is widely used as a standard procedure for diagnosis of breast cancer [12]. However, immunohistochemistry (IHC) assessment in CNB samples may be less reliable than in surgical specimens' due to the relatively smaller sample size and tumor heterogeneity [34]. Several studies have reported the concordance between preoperative CNB and surgical specimens for estrogen receptor (ER), and human epidermal growth factor receptor 2 (HER2) determination [567]. A recent meta-analysis has shown that the CNB tissue could replace open excision biopsy for determining ER, progesterone receptor (PR), and HER2 status [8]. The 2015 European Society of Medical Oncology breast cancer clinical practice guideline recommends a preoperative pathological examination of the CNB, with a report on ER, PR, and HER2 status by IHC or fluorescence in situ hybridization [9].
Neoadjuvant chemotherapy (NAC) before definitive surgery can reduce the size and extent of locally advanced tumors. There is an increasing acceptance of view that a pathological complete response (pCR) following chemotherapy is important, particularly as a surrogate for prognosis [10]. The information obtained from CNB may be the only information available for determining the candidates for preoperative or neoadjuvant treatment [3]. Therefore, demand has been markedly increased for clinicians to provide prognostic information considering the determination of IHC for treatment planning. However, there are few studies that have reported concordance rates between CNB and surgical specimens, before and after NAC.
In this study, we evaluated the concordance between CNB and surgical specimens in evaluating intrinsic biological subtypes and the receptor status, and examined the accuracy of CNB as a basic diagnostic method. Second, we assessed changes in intrinsic biological subtypes of breast cancer before and after NAC comparing CNB and surgical specimens.
METHODS
Data collection
We analyzed breast cancer patients with paired CNB and surgical specimen samples during 2014 at Samsung Medical Center, Seoul, Korea. Seventeen hundred eighty-six patients underwent primary surgery or NAC prior to operation. Clinical information on patients collected from medical records included age, body mass index, operation type, NAC history, and main pathological findings that included tumor size, number, nuclear grade, TNM stage, and ER, PR, HER2, and Ki-67 status from both CNB and surgical specimens. The study was approved by the Institutional Review Board of Samsung Medical Center (approval number: 2017-01-102), Seoul, Korea.
ER, PR, HER2, and Ki-67 evaluation
We used monoclonal antibodies for nuclear staining and ER (anti-ER; clone 6F11, Novocastra, Newcastle, UK) and PR (anti-PR; clone 16, Novocastra) status evaluation. A positive test was defined as staining greater than or equal to 1% of tumor cells. A negative test was defined as staining of less than 1% of tumor cells. We used the Allred score interpretation system of intensity score (0–3) and proportion score (0–5) [6].
HER2 (anti-HER2; 4B5, BenchMark XT, Ventana, Tucson, USA) was first graded by IHC and scored as 0 to 3+ according to the recommendations of the American Society of Clinical Oncology/College of American Pathologists [11]. The scoring system defines negative as 0/1+. No observed staining or faint/barely perceptible membrane staining in <10% of tumor cells is 0. Incomplete membrane staining or faint/barely perceptible membrane staining in ≥10% of tumor cells is 1+. A weak to moderate complete membrane staining observed in >10% of tumor cells is 2+ and is interpreted as equivocal. A strong complete membrane staining observed in >10% of tumor cells is 3+ and is considered as positive. In cases of HER2 2+ surgical specimens, we conducted silver in situ hybridization (SISH) assays (INFORM DDISH™ HER2 DNA SISH probe kits; BenchMark XT) to determine HER2 amplification [1112].
Ki-67 immunostaining was performed using the monoclonal antibody Ki-67 (clone MIB-1; Dako, Glostrup, Denmark). Ki-67 is a nuclear marker expressed in all phases of the cell cycle other than the G0 phase [1314]. Ki-67 expression has a value between 0% and 100% and is reported at 10% intervals in our center. In this study, we classified samples as low or high expression using 20% as cutoff value.
Five intrinsic biological subtype classifications were categorized according to the 12th St. Gallen international breast cancer conference (2011): luminal A (ER and/or PR positive, HER2 negative, and Ki-67 low); luminal B/HER2 negative (ER and/or PR positive, HER2 negative, and Ki-67 high); luminal B/HER2 positive (ER and/or PR positive, any Ki-67 and HER2 positive); HER2 positive (ER and PR absent, and HER2 positive); and triple negative (ER and PR absent, and HER2 negative) [15].
Statistical analysis
Concordance analysis of ER, PR, HER2, Ki-67, and five intrinsic biological subtypes was performed on CNB and surgical specimens. Statistical analysis for concordance was calculated using κ-tests. κ-values >0.8 indicated very good agreement, between 0.6 and 0.8 indicated good agreement, between 0.4 and 0.6 were considered as moderate agreement, <0.4 as fair, and <0.2 as poor agreement. All statistical tests were two-sided and considered significant if p-value was below 0.05. We used SPSS version 22.0 (IBM Corp., Armonk, USA).
RESULTS
Patient characteristics
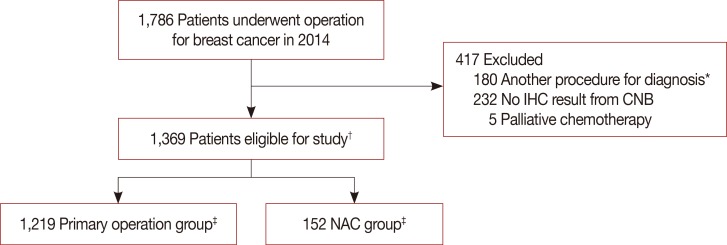
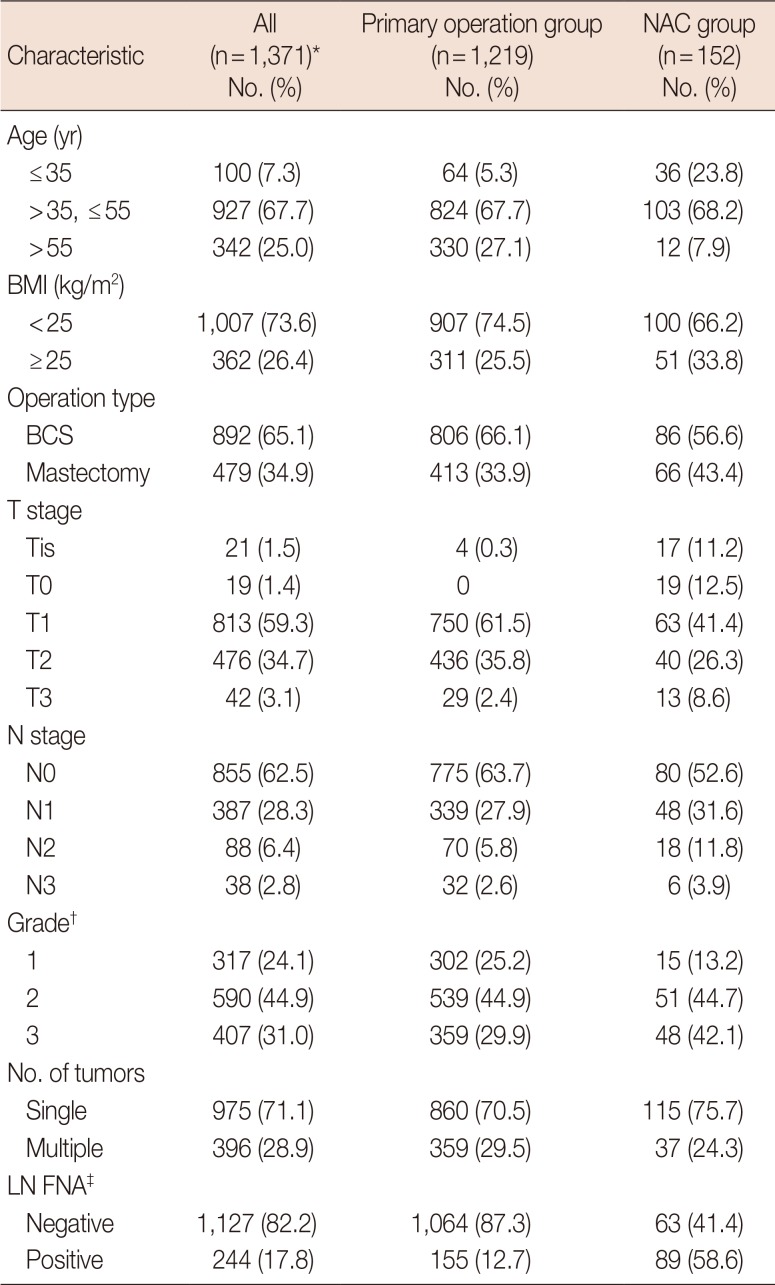
We investigated 1,786 breast cancer patients who underwent surgery during 1 year. There were 1,369 eligible patients with a median age of 49.5 years (range, 24–86 years). We excluded 180 patients who underwent vacuum-assisted biopsy, excisional biopsy, or had previous breast surgery. Moreover, 232 patients were excluded for inadequate test results; for example, CNB sent from other hospitals after diagnosis and their specimens were inadequate to conduct IHC test. Five more patients were excluded because they received palliative chemotherapy. After diagnosis by CNB, 1,219 patients underwent primary surgery and 152 received NAC before surgery (Figure 1); there were two patients with bilateral breast cancer in each group. Patient characteristics and pathology results are shown in Table 1. Eight hundred ninety-two patients (65.1%) underwent breast-conserving surgery and 479 (34.9%) underwent mastectomy. The rate of mastectomy was higher in the NAC group than in the primary surgery group.
Tumor pathology and IHC results
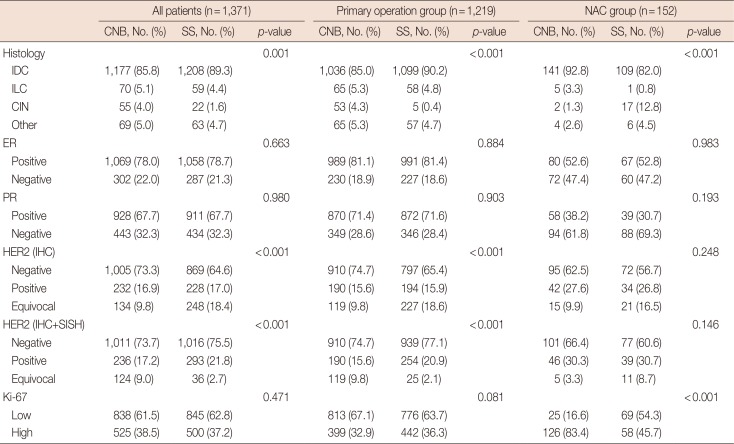
About 86% of patients were diagnosed with invasive ductal carcinoma using CNB. Expression of ER, PR, and Ki-67 was not significantly different between CNB and surgical specimens, except for HER2 in the primary surgery group. Patients receiving NAC showed a difference in the Ki-67 status. In contrast, ER, PR, and HER2 did not show significant differences (Table 2).
Concordance of IHC results
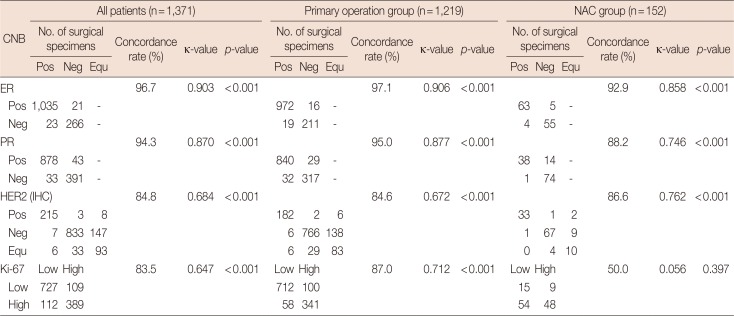
ER and PR expression in CNB samples showed very good agreement with results for surgical samples; overall concordance rate was 96.7% for ER (κ=0.903) and 94.3% for PR (κ=0.870). HER2 and Ki-67 expression showed good agreement between CNB and surgical specimens; overall concordance rate was 84.8% for HER2 (κ=0.684) and 83.5% for Ki-67 (κ=0.647).
We divided patients into primary surgery and NAC groups. Concordance rates and κ-values for ER, PR, and HER2 showed similar tendency between the two groups. Meanwhile, in cases of primary surgery, Ki-67 expression also showed good agreement between CNB and surgical results with a concordance of 87.0% and κ-value of 0.712. The NAC group had poor agreement between CNB and surgical results with a concordance of 50.0% and κ-value of 0.056 (p=0.397) (Table 3).
Concordance among intrinsic biological subtypes
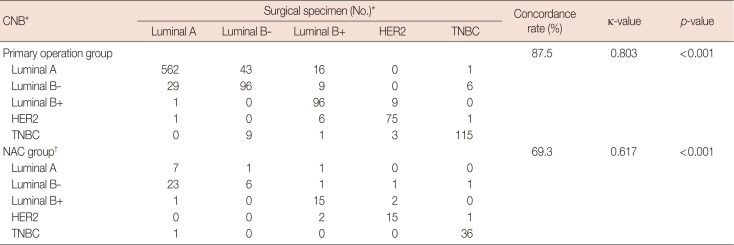
We classified surgical specimens and CNB into five intrinsic biological subtypes according to the 12th St. Gallen international breast cancer conference: luminal A, luminal B (HER2 negative and positive), HER2 positive, and triple negative. Concordance among the five subtypes was 85.8% and the κ-value was 0.786 (p<0.001). Concordance rates of the subtypes were 87.5% for the primary surgery group and 69.3% for the NAC group, and the κ-values between CNB and surgical specimen results were 0.803 and 0.617, respectively (p<0.001) (Table 4).
pCR rate according to the intrinsic biological subtypes in NAC patients
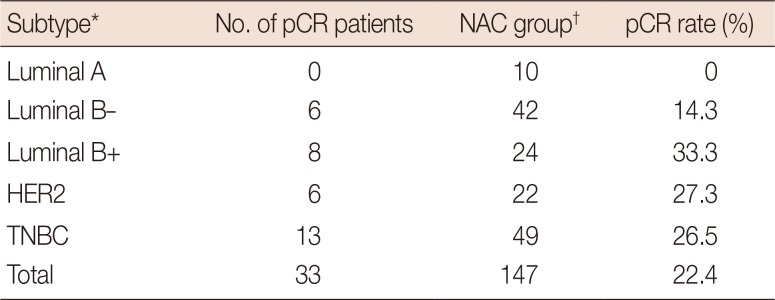
We included both no residual disease of any sort and residual ductal carcinoma in situ (DCIS) without invasive disease and node metastasis in to define pCR. Among the 147 patients in the NAC group, the total pCR rate was 22.4% (33/147); the pCR rate of each intrinsic biological subtypes is shown in Table 5. Among the 33 patients who achieved pCR, 17 patients had no residual tumor and 16 patients had DCIS. No residual tumor patients were excluded from the comparison of the IHC results between CNB and surgical specimens because they had no available tissue sample and postoperative IHC assay could not be performed.
DISCUSSION
In this study, we investigated the concordance among IHC test results obtained using CNB and surgical specimens, as well as the agreement with subgroup classification. We found very good agreement for ER and PR with concordance rates of 96.7% (κ=0.903) and 94.3% (κ=0.870), respectively. HER2 and Ki-67 showed concordance rates of 84.8% (κ=0.684) and 83.5% (κ=0.647), respectively, which was interpreted as good agreement. Subgroup analysis showed 85.8% agreement and κ-value of 0.786, also indicating good agreement.
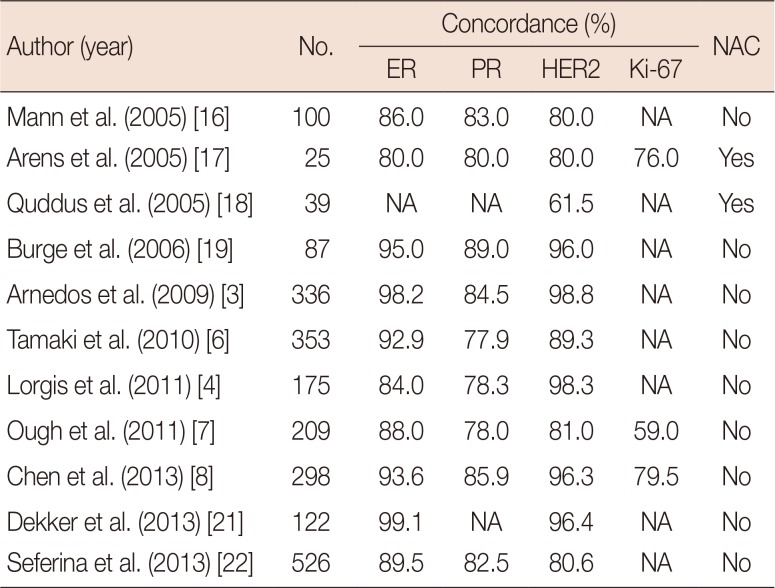
ER and PR status between CNB and surgical specimens showed very good agreement. These results were similar to those that were previously reported; the concordance rates between CNB and surgical specimens of these previous results are shown in Table 6 [346716171819202122]. Hormone receptors are used as predictive factors for response to endocrine therapy and as prognostic factors [23]. We also found that overall agreement between CNB and surgical specimens is better for ER than PR. This result suggests that PR is more heterogeneously distributed in tumors [24].
Approximately 15% to 20% of breast cancer patients have HER2 gene amplification [11]. This study showed a significant difference when comparing results with CNB and surgical specimens for HER2 (Table 2). As a result of the IHC test, concordance rate was 84.8% and the κ-value was 0.684. Equivocal results were 9.8% and 18.4% for CNB and surgical specimens, respectively. We then performed additional SISH tests when HER2 2+ equivocal results were primarily obtained from surgical specimens, and defined HER2 positivity as SISH positive.
Ki-67 is currently the most representative marker for tumor proliferation [13]. The proliferating fraction of cells in tumors prior to treatment, as measured by the Ki-67 nuclear antigen and S-phase fraction (SPF), predict response to chemotherapy [25]. However, scoring procedures have varied, and standardization according to the specimen type is lacking [14]. In our institution, we divided the Ki-67 values at 10% intervals, and the cutoff value for high Ki-67 in this study was defined as 20%. In this study, no significant difference was observed in high and low Ki-67 values between CNB and surgical specimens, with a concordance rate of 83.5% and a κ-value of 0.647.
No significant difference was noted in the expression of hormone receptors in the NAC group. Concordance rate was 92.9% for ER (κ=0.858) and 88.2% for PR (κ=0.746). These results were slightly lower than those of the primary surgery group, but they still showed very good or good agreement as the κ-value was >0.6. HER2 results showed no significant difference between CNB and surgical specimens. Concordance rate of the IHC results was 86.6% and the κ-value was 0.762. However, the concordance rate for Ki-67 was 50.0% and the κ-value was 0.056 (p=0.397), indicating inconsistency between the two groups. These findings suggest that NAC affected proliferative activity and the chemotherapeutic agents interfered with the signal transduction pathway associated with cell division, resulting in a diminished SPF [18].
The degree of agreement of each ER, PR, and HER2 was generally good, except for results of Ki-67 in the NAC group (Table 3). The five intrinsic biological subtypes according to the 12th St. Gallen conference also showed high concordance rate in the NAC group (69.3%, κ=0.617, p<0.001) (Table 4). Notably, 20% of patients (23/114) of the Luminal B (HER2 negative) group turned out to be luminal A after NAC due to a decrease in Ki-67 expression (Table 4). A previous study has found a significant decrease in Ki-67 expression after NAC with mitoxantrone, methotrexate (±mitomycin C), and tamoxifen [25], which has been confirmed in this study.
In the current study, the pCR rate was 0% in the luminal A, 14.3% in the luminal B/HER2 negative, 33.3% in the luminal B/HER2 positive, 27.3% in the HER2, and 26.5% in the triple-negative breast cancer group. These results were similar to those of a large German series and recent studies for the same pCR definition [262728]. For this reason, it is important to determine the intrinsic biological subtypes of breast cancer with CNB before NAC for predicting clinical benefits and it is recommended to some institutes that there are not conducting IHC of CNB specimens before NAC.
There are some limitations in this study. First, this was a single-center, retrospective study. Hence, the results could have selection bias and cannot be generalized. Second, many patients were initially diagnosed in other institutes and referred to our institute for surgery. In this case, CNB was not reexamined, except in cases of vague diagnoses. CNB results were exposed to the possibility of several levels of technical problems that may arise during pathological examinations at hospitals. Third, several neoadjuvant regimens were used depending on the patient, which might cause bias when evaluating the pCR rate among the intrinsic biological subtypes. Besides the limitations, to our knowledge, this study is one of the largest studies comparing concordance between CNB and surgical specimens with sufficient patients who were treated following the same guidelines in a short period. Second, we evaluated the factors of ER, PR, HER2, and Ki-67, which constitute the five intrinsic subtypes according to the 12th St. Gallen international breast cancer conference (2011) [15]. Third, we compared the results of concordance between CNB and surgical specimens of the NAC group at the same time.
In conclusion, CNB showed high diagnostic accuracy when compared with surgical specimens, and good agreement for ER, PR, HER2, and Ki-67. Similarly, patients who underwent NAC also showed good agreement for receptor status, except for Ki-67. Our findings reaffirmed the recommendation of CNB as an initial procedure for breast cancer diagnosis, as well as the assessment of the receptor status and intrinsic biological subtypes to determine further treatment plans.
 XML Download
XML Download