

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most common malignancy in women, and invasive carcinoma of no special type is the most common form of breast cancer [12]. Several studies have attempted to identify potential therapeutic agents and prognostic markers of breast cancer. The staging system of the American Joint Committee on Cancer (AJCC) indicates that histological grade, estrogen receptor (ER) positivity, progesterone receptor (PR) positivity, and human epithelial growth factor receptor 2 gene (HER2) overexpression are important parameters for determining therapeutic options for breast cancer. A recent study analyzed breast cancer cell lysates by performing quantitative enzyme-linked immunosorbent assay (ELISA) and identified urokinase-type plasminogen activator (uPA) and plasminogen activator inhibitor 1 (PAI-1) as novel prognostic markers in patients with breast cancer [1]. uPA, a serine protease, and its inhibitor PAI-1 are the key players in proteolytic cascades involved in tumor progression, extracellular matrix degradation, cell proliferation, cell adhesion, and cell migration [2]. Several international research groups have shown that uPA and PAI-1 levels in breast tumors are indicators of disease aggressiveness and are strong prognostic markers of disease-free survival (DFS) and overall survival (OS) in patients with primary breast cancer [345]. Low uPA and PAI-1 levels are associated with a low risk of recurrence. This pattern is more prominent in patients with breast cancer showing ER or PR positivity who are undergoing adjuvant endocrine therapy and in whom chemotherapy is less effective [67]. Multicenter, prospective, randomized trials investigating uPA and PAI-1 are ongoing [8]. In several trials, patients with high uPA and PAI-1 levels who received chemotherapy with 5-fluorouracil, epirubicin, and cyclophosphamide showed better responses than control patients [679]. Further, a recent study discussed the role of tumor uPA and PAI-1 levels in a making decision for using adjuvant therapy for treating early breast cancer [10]. In the present study, we evaluated uPA and PAI-1 levels by performing immunohistochemical staining to determine whether they were reliable prognostic markers in patients with breast cancer.
METHODS
Patient selection
The study included 214 patients with invasive ductal carcinoma (IDC) and 80 patients with ductal carcinoma in situ (DCIS) who were diagnosed and treated at Kangbuk Samsung Hospital from January 2006 to April 2010. All the experiments were conducted after obtaining approval from the Institutional Review Board of the Kangbuk Samsung Hospital (approval number: 2013-01-250). The patients were characterized based on their clinical characteristics such as age at diagnosis, history of hormone replacement therapy (HRT), history of trastuzumab therapy, history of radiation therapy, locoregional recurrence, distant metastasis, and death due to breast cancer. The patients were also characterized based on their pathological characteristics such as skin or chest wall invasion, Paget disease, lymphovascular invasion (LVI), ER positivity, PR positivity, HER2 overexpression, triple negativity in immunohistochemical staining, TNM stage, lymph node metastasis, and AJCC stage. Hematoxylin and eosin (H&E)-stained slides from all the patients were reviewed by two pathologists (S.I.D. and S.W.C.) to reconfirm histological data such as T and N stage, lymphatic invasion, and other characteristics. Discrepancies among cases were resolved through consensus.
Tissue microarray construction
Surgical specimens were fixed in 10% buffered formalin, processed, and embedded in paraffin. All H&E-stained slides were individually reviewed, and the most representative tumor area was selected and marked on individual paraffin blocks. The most representative tissue core was obtained from each tumor specimen. Tissue microarray (TMA) specimens were assembled using a TMA instrument (TMA Master; 3D HISTECH, Budapest, Hungary) containing thin-walled stainless steel punches and stylets for emptying and transferring needle contents. The assembly was held in an X-Y position, with a 1-mm increment between individual samples, 4-mm punch depth stop device, and semiautomatic micrometers. The instrument was used to create holes in recipient blocks with defined array cores. A fit needle was used to deliver the tissue cores into the recipient blocks. Considering the limitations in the representative areas of the tumor specimens, duplicate 2-mm-diameter tissue cores were used from each donor block. The percentage of tissue core taken from within the tumor was >70%.
Immunohistochemical staining and evaluation
Immunohistochemical staining was performed using 2-µm sections of TMA blocks. The sections were incubated in 0.3% H2O2 solution for 15 minutes to inhibit endogenous peroxidase activity. Antigen retrieval was performed using a solution containing 10 mM Tris, 1 mM EDTA, and 0.03% Tween 20 for 30 minutes in a presser cooker. Nonspecific blocking was quenched by incubating the sections with 4% bovine serum albumin for 30 minutes. The sections were then incubated with primary antibodies against PAI-1 (dilution, 1:20; Abcam, Cambridge, USA) and uPA (dilution, 1:50 Abcam) for 1 hour at room temperature. Immunohistochemical staining was detected using ChemMate polymer kit and ChemMate™ DAKO EnVision™ Detection Kit (K5007; DAKO, Glostrup, Denmark), according to the manufacturer's instructions. Next, the sections were stained with liquid diaminobenzidine tetrahydrochloride by using a high-sensitivity substrate–chromogen system (K5007; DAKO). Finally, the sections were counterstained with Mayer's hematoxylin. Results of immunohistochemical staining were graded according to both the intensity and percentage of positively stained tumor cells. Staining intensities of uPA and PAI-1 were scored on a scale of 0 to 3, with 0 indicating no staining, 1 indicating weak staining, 2 indicating moderate staining, and 3 indicating strong staining. The percentage of positively stained cells was also classified into the following four categories: 1 (0%–24%), 2 (25%–49%), 3 (50%–74%), and 4 (75%–100%). In case of discrepancy between duplicate cores, higher score of 2 tissue cores was used as the final score. Level of staining was analyzed as immunoreactive score (IRS), which was calculated by multiplying the score of staining intensity and the percentage of positively stained cells [11]. Expression levels of uPA and PAI-1 were classified as low expression (IRS ≤7) and high expression (IRS >7), according to a previous study [11].
Data analysis
Statistical analyses were performed using PASW Statistics for Windows, version 18.0 (SPSS Inc., Chicago, USA). Chi-square and Fisher exact tests were used to evaluate the associations between uPA and PAI-1 expression and clinicopathological parameters. DFS was defined as the length of time from the day of surgery to the day of recurrence. OS was defined as the length of time from the day of diagnosis to the day of patient's death or last known contact. Cox proportional hazards regression test was used to calculate hazard ratio (HR) of data on DFS and OS. Multivariate Cox regression analysis was performed only for variables with a significant univariate impact. Survival probability curves were calculated using Kaplan-Meier method. A p-value of <0.05 (two-tailed) was considered statistically significant.
RESULTS
Demographic characteristics of patients
We retrospectively reviewed the clinicopathological data of 214 patients with IDC and 80 patients with DCIS (Table 1). The mean age of the patients was 49.0±11.6 years (range, 27–82 years). Eighty patients (27.2%) had stage 0 tumors, 66 patients (22.5%) had stage I tumors, 110 patients (37.4%) had stage II tumors, and 38 patients (12.9%) had stage III tumors. LVI and lymph node metastasis were detected in 88 (32.1%) and 104 (35.4%) patients, respectively. Of the 294 patients studied, 10 (3.4%), 23 (7.8%), and eight (2.8%) patients showed locoregional recurrence, distant metastasis, and death due to breast cancer, respectively, during follow-up.
Expression of uPA and PAI-1 and its association with the clinicopathological characteristics of patients
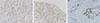
Of the 214 patients with IDC, 44.8% showed high uPA expression and 64.9% showed high PAI-1 expression (Table 2, Figures 1, 2). Patients with DCIS showed higher PAI-1 expression than those with IDC (82.5% and 36.2%, respectively; p=0.003) (Table 2).
Further, uPA or PAI-1 expression was not significantly associated with locoregional recurrence (p=0.754 and p=0.911, respectively), distant metastasis (p=0.459 and p=0.637, respectively), or death due to breast cancer (p=0.471 and p=0.428, respectively) (Table 3). Lymph node metastasis was significantly associated with high uPA expression (p=0.001) (Table 4). Univariate analyses showed that HRT, skin and chest wall invasion, LVI, ER positivity, triple-negative subtype, and N stage were significantly associated with OS (p<0.050) (Supplementary Table 1, available online). Moreover, age at diagnosis, HRT, radiation therapy, Paget disease, T stage, and AJCC stage were significantly associated with DFS (p<0.050) (Supplementary Table 1).
Multivariate analyses did not show any association between uPA and PAI-1 expression and prognostic factors or predictors of high uPA and PAI-1 expression (data not shown). Kaplan–Meier curve analyses did not show any association of uPA and PAI-1 expression with OS (uPA: χ2=0.345, df=2, p=0.589; PAI-1: χ2=1.059, df=3, p=0.951) and DFS (uPA: χ2=2.605, df=2, p=0.272; PAI-1: χ2=0.529, df=3, p=0.912).
DISCUSSION
Malignant tumors degrade the extracellular matrix, which is crucial for their invasion and metastasis. Proteolytic enzymes such as matrix metalloproteinases, cysteine proteases, and serine proteases play an important role in cancer metastasis [12]. The uPA system is an important proteolytic system. uPA is a 50-kDa serine protease synthesized by fibroblasts, monocytes, neutrophils, epithelial cells, and tumor cells and is involved in tissue remodeling. uPA-mediated proteolysis is regulated at several levels, particularly by PAI-1, which belongs to serpin superfamily [13]. The uPA system includes serine proteases involved in the degradation of basement membranes and extracellular matrix that promotes tumor invasion and metastasis [1415]. Several research groups have shown that high uPA and PAI-1 levels in primary breast cancer tissue are indicators of breast cancer aggressiveness and strong prognostic markers of primary breast cancer [345].
Our results showed that high PAI-1 expression was more prominent in patients with DCIS (82.5%) than in patients with IDC (36.2%) (p=0.003) (Table 2). The role of PAI-1 in cancer is unusual. While PAI-1 inhibits the invasion and metastasis of some cancers by inhibiting uPA–Urokinase-type plasminogen activator receptor (uPAR) [161718], it promotes the growth and angiogenesis of some cancers [1819]. Our results are consistent with the role of PAI-1 in the inhibition of cancer invasion. PAI-1 may inhibit the uPA system in the early stages of tumor progression by binding to the uPA–uPAR complex. Although results of a previous study indicated an association between high PAI-1 expression in primary breast cancer tissue and poor prognosis [2021], the results of our study did not show a significant association between high PAI-1 expression and prognosis of patients with IDC.
Malinowsky et al. [22] compared uPA and PAI-1 expression and signaling in primary breast tumors and lymph node metastases. They observed that uPA was highly expressed in both primary tumors and lymph nodes, whereas PAI-1 was differentially expressed in primary tumors and lymph nodes. Our data showed a nonsignificant negative correlation between PAI-1 expression and lymph node metastasis (HR=0.592, p=0.080) (Table 4). However, high uPA expression was detected in higher percentage of patients with lymph node metastasis (56.3%) than in patients without lymph node metastasis (33.6%) (p=0.001) (Table 3). This result suggested that uPA expression affected lymph node metastasis of breast cancer.
We did not observe any association between uPA and PAI-1 expression and breast cancer prognosis. However, a previous study reported that high uPA and PAI-1 levels were associated with poor relapse-free survival and OS in patients with lymph node-positive or lymph node-negative disease [232425]. However, Cox univariate analyses of OS and DFS showed that uPA and PAI-1 expression was not associated with disease outcomes (Supplementary Table 1). To determine the natural course of the disease and unaltered prognostic impact of uPA and PAI-1, which was not affected by adjuvant systemic chemotherapy, we performed univariate analyses of OS and DFS in 109 patients with lymph node-negative disease who underwent adjuvant chemotherapy (data not shown). However, we did not observe any association between uPA and PAI-1 expression and disease outcomes in these patients.
Limitations of the present study are associated with the retrospective nature of data analyses. First, the study included small number of patients who relapsed or died due to breast cancer, which might be responsible for the lack of association observed between the known prognostic factors such as hormone receptor positivity, HER2 overexpression, triple-negative subtype, and lymph node metastasis and prognosis (Supplementary Table 1).
Second, we performed immunohistochemical staining instead of ELISA to determine uPA and PAI-1 expression. At present, ELISA is the gold standard for determining uPA and PAI-1 expression. However, ELISA is not an effective method because it is time consuming and requires >300 mg of fresh or frozen breast cancer tissue [2627]. Haas et al. [28] questioned the reliability of ELISA because ELISA performed using tissue sample isolated from near the biopsy channel showed decreased and increased uPA and PAI-1 levels, respectively. Immunohistochemical staining is a new alternative method for detecting uPA and PAI-1 expression, and a recent study by Lang et al. [29] has discussed the practical use of this method. The study by Lang et al. showed that uPA and PAI-1 levels determined by performing immunohistochemical staining were more clinically significant than those determined by performing ELISA. Moreover, the therapeutic relevance of uPA and PAI-1 levels determined by performing immunohistochemical staining was comparable to that of uPA and PAI-1 levels determined by performing ELISA [26].
In conclusion, our results showed that high PAI-1 expression was more prominent in patients with DCIS than in patients with IDC, suggesting that PAI-1 was involved in tumor progression in the early stages of breast cancer, such as DCIS. In addition, our results showed that high uPA expression was associated with lymph node metastasis of breast cancer, indicating that uPA affected tumor aggressiveness.





 XML Download
XML Download