

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The efficacy of myelosuppressive chemotherapy regimens is often restricted by dose-limiting toxicities that can delay subsequent treatment cycles. Febrile neutropenia (FN) is a common adverse effect of chemotherapy, sometimes causing life-threatening complications [1]. Chemotherapy-induced FN may also result in modifications to the chemotherapy dose or schedule, which may compromise treatment efficacy [2]. In breast cancer, there is evidence supporting a close correlation between maintaining the relative dose intensity (RDI) of neoadjuvant or adjuvant chemotherapy and the clinical outcomes of patients [34]. Prevention of chemotherapy-induced FN is therefore a medical priority in neoadjuvant or adjuvant settings.
Recombinant granulocyte-colony stimulating factor (G-CSF) products have emerged as effective therapies for reducing the duration and incidence of chemotherapy-induced neutropenia and FN by stimulating neutrophil proliferation and differentiation in cancer patients [5]. Clinical guidelines from the American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN) in the United States, and from the European Organization for Research and Treatment of Cancer (EORTC), all recommend that G-CSF should be administered prophylactically if the risk of FN is greater than 20%. In the case of chemotherapeutic regimens with an intermediate risk of FN (10%–20%), the guidelines emphasize the importance of considering several risk factors for evaluating a patient's overall risk for FN [67]. These risk factors include old age, previous chemotherapy or radiotherapy, pre-existing neutropenia or infection, poor performance status, and poor renal or hepatic functions. However, ethnic or geographic differences in response to the same chemotherapy regimen have so far been poorly investigated.
Sequential doxorubicin/cyclophosphamide and docetaxel (AC-D) is a widely used neoadjuvant and adjuvant chemotherapy regimen for breast cancer. The incidence of FN ranges widely from 3.1% to 25%, and many guidelines including the NCCN, ASCO, and EORTC have categorized this regimen into the intermediate risk group (e.g., the risk of FN is 10%–20%) [89]. However, most of these studies were conducted in Western countries [1011], and there have been few reports on the incidence of FN in Asian countries.
METHODS
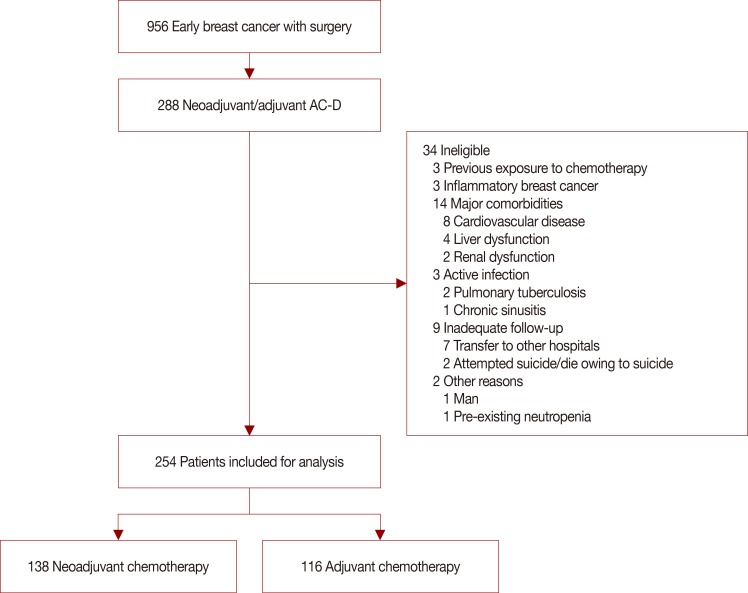
This study was approved by the Institutional Review Board of Yonsei Cancer Center (approval number: 4-2015-1154). Breast cancer patients who received neoadjuvant or adjuvant sequential AC-D from September 2010 to February 2013 were analyzed from the Yonsei Cancer Center registry of breast cancer. Patients with previous exposure to chemotherapeutic agents; inflammatory breast cancer; major cardiovascular, liver, or renal diseases; active infection; inadequate follow-up; or preexisting neutropenia were excluded in order to minimize other confounding factors (Figure 1).
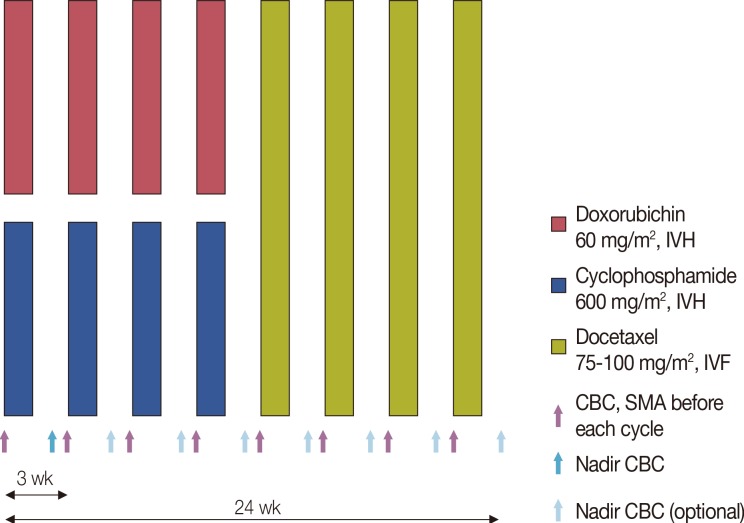
Four cycles of doxorubicin (60 mg/m2) and cyclophosphamide (600 mg/m2) followed by four cycles of docetaxel (75 mg/m2 or 100 mg/m2) were administered. Blood samples were collected before each cycle for complete blood cell counts with differential and serum samples for chemistry assays. During the first cycle, nadir blood cell counts were measured between days 10 and 14. After the first cycle, nadir blood cell counts were measured selectively (Figure 2).
Data on patient demographics, pretreatment laboratory parameters, and tumor characteristics were collected. Patients were divided into four subtypes in accordance with the St. Gallen 2011 consensus [16]. The incidence of FN, FN-related hospitalization requiring intravenous antibiotics, FN associated with shock or death, subsequent dose reduction/delay, and other hematologic toxicities according to the common terminology criteria for adverse events (CTCAE), version 4.02, were investigated. FN was defined as neutropenia (<500 neutrophils/µL or <1,000 neutrophils/µL for over 48 hours) with a febrile event (oral temperature ≥38.3℃, or ≥38.0℃ for over 1 hour) observed by medical staff. Dose reduction was defined as reductions in the delivered dosages of agents administered relative to the standard values, and dose delay was defined as a chemotherapy interval of more than 28 days (more than 7 days delay) or early cessation of chemotherapy. RDI was calculated by the method described in Supplementary Table 1 (available online) [17].
All patients received neither G-CSF nor antibiotics as primary prophylaxis for FN. Secondary prophylaxis with G-CSF, antibiotics for FN, and dose reduction/delay were administered at the physicians' discretion. Filgrastim was the most commonly used G-CSF analogue, and choice of antibiotics was based on NCCN guidelines.
Statistical analyses were performed using SPSS version 21.0 for Window (IBM Corp., Armonk, USA). Descriptive statistics were used for baseline characteristics. Binomial two-sided 95% confidence intervals (CIs) for the incidence of FN and dose reduction/delays were calculated. The chi-square test was used for comparison between categorical variables, and the two-sample t-test was used for comparison between continuous variables. Two-sided p-values less than 0.05 were considered statistically significant.
RESULTS
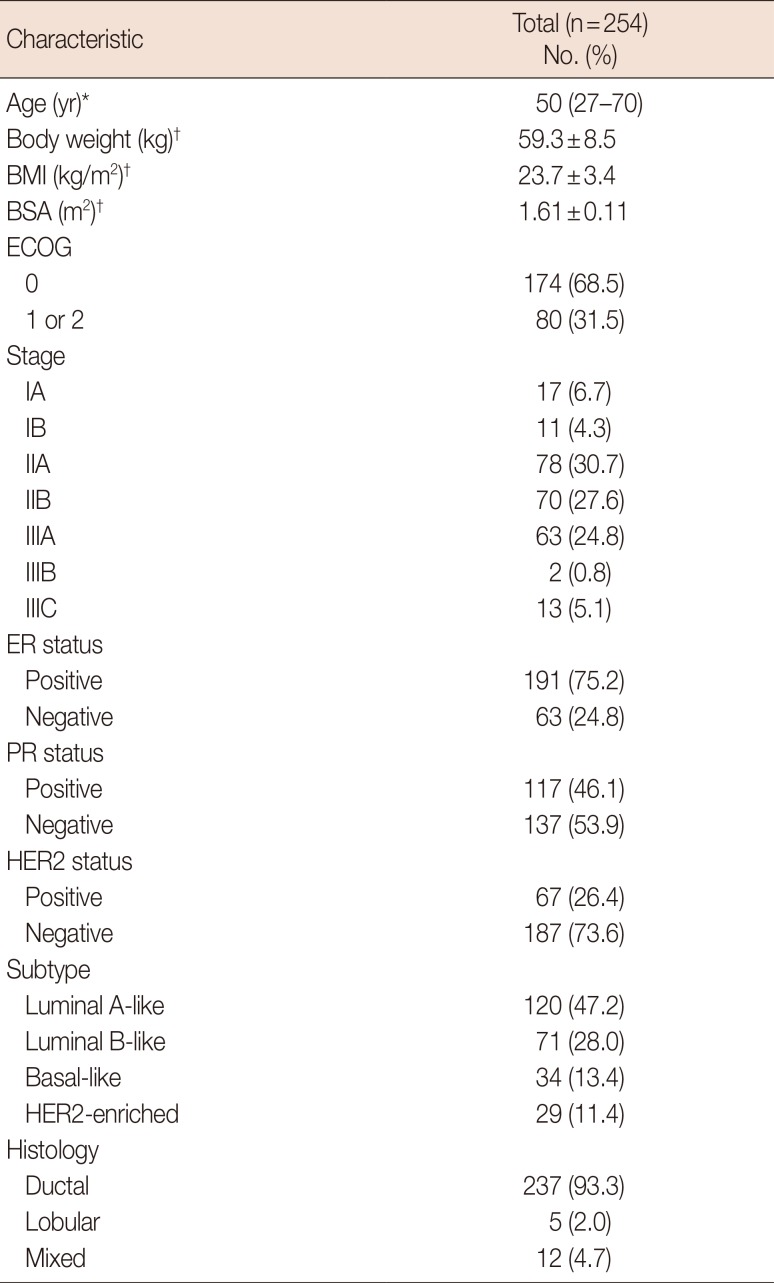
Between September 2010 and February 2013, 254 Korean breast cancer patients receiving AC-D were recruited for the analysis (Table 1). The median patient age was 50 years (range, 27–70 years) and 5.9% (15/254) of patients were more than 65 years old. The mean body weight, body mass index, and body surface area were 59.3±8.5 kg, 23.7±3.4 kg/m2, and 1.61±0.11 m2, respectively. The number of patients with Eastern Cooperative Oncology Group performance status 1 or 2 was 31.5% (80/254). There were 13.4% (34/254) cases of basal-like subtype tumors and 11.4% (29/254) cases of human epidermal growth factor receptor 2 (HER2) enriched subtype tumors. A total of 138 patients received neoadjuvant chemotherapy and 116 patients received adjuvant chemotherapy.
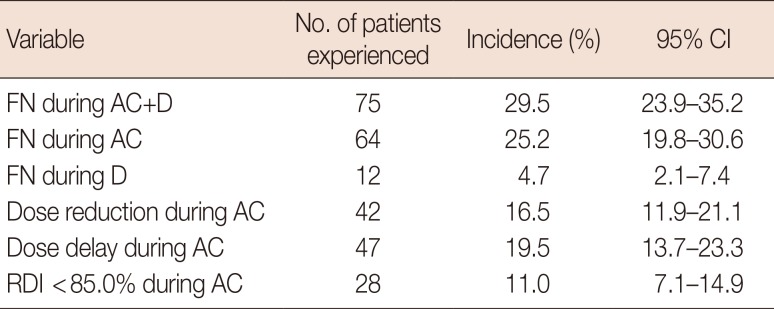
During the AC and D stages of chemotherapy 25.2% (64/254) and 4.7% (12/254) patients experienced FN, respectively (Table 2). Overall, 29.5% of patients experienced FN during chemotherapy (95% CI, 23.9%–35.2%, 75/254). Dose reduction, delays, and RDI less than 85.0% during AC were observed in 16.5% (42/254), 19.5% (47/254), and 11.0% (28/254) of patients, respectively.
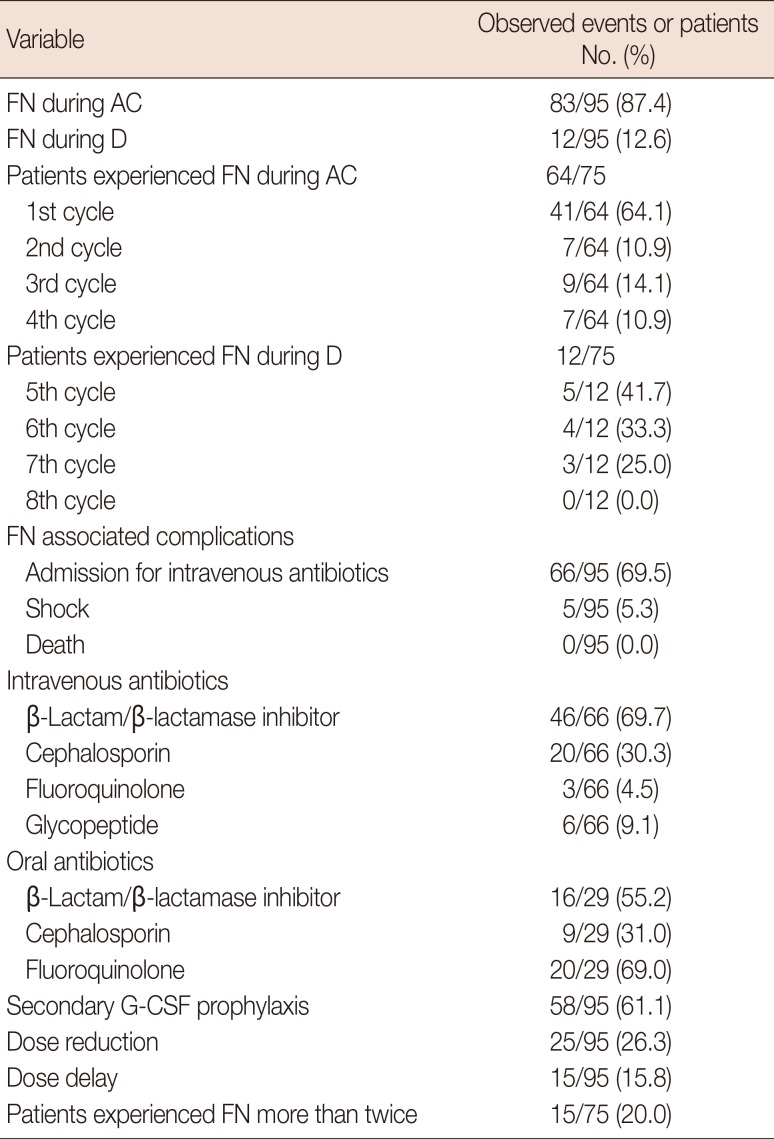
The total number of FN events during chemotherapy was 95, including 83 events (87.4%) during AC and 12 events (12.6%) during D (Table 3). Of the 64 patients who experienced FN during AC, 41 patients (64.1%) experienced FN in the first cycle. Of 95 events of FN, 66 events (69.5%) were accompanied by administration of intravenous antibiotics and five (5.3%) were accompanied by septic shock. No chemotherapy-related death was observed. The median duration of admission was 5 days, ranging from 2 to 20 days. β-Lactam/β-lactamase inhibitors were the most frequently used intravenous antibiotics (69.7%) and glycopeptides were used in six events (9.1%). Secondary G-CSF prophylaxis for the next cycle was administered in 58 cases (61.1%). Dose reduction and dose delays were performed in 26.3% and 15.8% of patients, respectively. Fifteen patients experienced more than two events of FN, even with prophylactic G CSF administration, and dose reduction/delays were performed for these patients.
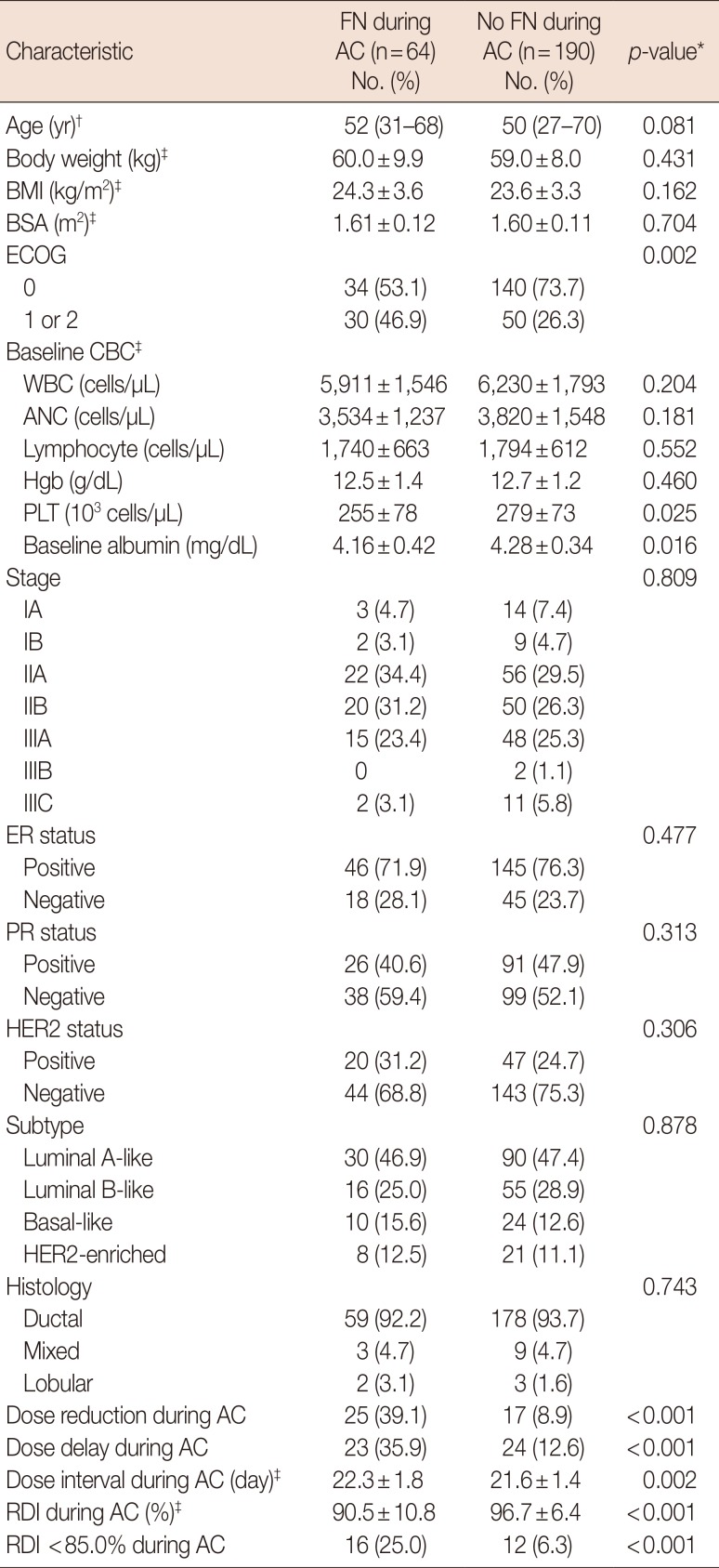
Baseline and treatment characteristics were compared between patients who experienced FN during AC and patients who did not (Table 4). Dose reduction and delay during AC chemotherapy were more frequently observed in patients who experienced FN (39.1% vs. 8.9%, p<0.001; 35.9% vs. 12.6%, p<0.001, respectively). The dose interval during AC was longer in patients who experienced FN (22.3 vs. 21.6 days, p=0.002) and the RDI during AC was lower in patients who experienced FN (90.5% vs. 96.7%, p<0.001). Patients who experienced FN during AC were more likely to have an RDI less than 85.0% (25.0% vs. 6.3%, p<0.001).
We investigated other hematologic toxicities by using the CTCAE grading system (Supplementary Table 2, available online). Patients with FN during AC cycles were more likely to experience grade 3/4 lymphopenia, anemia, and thrombocytopenia (Supplementary Table 3, available online).
DISCUSSION
This study showed that the incidence of FN during AC-D chemotherapy was 29.5% in breast cancer patients in Korea. FN events occurred frequently during AC chemotherapy (25.2%) and more than half of the FN events (64.1%) occurred in the first cycle. Patients who experienced FN were more likely to have poor performance status and low pretreatment albumin levels, similar to the results of a previous study [18]. Patients with FN events frequently experienced dose reduction/delays, which eventually led to a decreased RDI. Furthermore, we observed frequent hospitalization and use of intravenous antibiotics for the management of FN.
Previous studies reported a diverse range of FN incidence during AC or AC-D chemotherapy. The ECOG 1199 and CALBG 40101 trials reported an incidence of FN of 6.5% and 6.0%, respectively, during adjuvant AC chemotherapy [1920]. The CALGB 9741 and BCIRG-005 trials reported an incidence of 6.0% and 7.7%, respectively, during adjuvant AC-D chemotherapy [1121]. The GEPARDUO study documented an incidence of 3.7% during neoadjuvant AC-D chemotherapy [8]. In contrast to early breast cancer patients, the FN incidence was higher in patients with metastatic breast cancer during AC-D chemotherapy, up to 25% of those without prophylactic G-CSF support [22]. Chan et al. [23] investigated the incidence of FN following AC chemotherapy in Asian countries. After the first cycle, 9.1% (17/189) of patients developed FN and after all cycles this rose to 13.8%. The authors pointed out that the relatively lower incidence of FN in previous randomized control trials could be attributed to patient selection before inclusion into the trial.
Ethnic differences in hematologic toxicity from chemotherapeutic agents or monoclonal antibodies have been described in lung cancer [121324] and renal cell carcinoma patients [14]. In breast cancer, the pharmacokinetics and pharmacodynamics of doxorubicin and docetaxel are different in terms of nadir white blood cell count and neutrophil count between ethnicities [25]. Genetic polymorphisms also influence nadir white blood cell and neutrophil counts in patients receiving cyclophosphamide-based combination chemotherapy [26]. In these previous studies, severe hematologic toxicities were more frequently observed in Asian patients than in Western patients. These findings provide indirect evidence that Asian patients are more likely to experience FN during chemotherapy. Consistent with the findings above, although the patients in our study did not have any of the baseline characteristics that elevate the risk of FN, including other comorbidities, they had FN events more frequently and lower RDIs during AC-D chemotherapy compared to study populations in previous studies that were mostly conducted in Western countries.
Our study has several limitations, including its relatively small sample size, being conducted in a single institution, and its retrospective nature. Indications for admission, selection of antibiotics, secondary G CSF prophylaxis, and dose reduction/delay were according to the individual physicians' judgment rather than protocol-defined management. Additionally, only FN reported officially was counted, and patients' or caregivers' self-documentation of febrile events were excluded, which could imply under-estimation of the incidence of FN. When we included possible cases of FN in the analysis, 32.7% (95% CI, 26.9%–38.5%) and 28.3% (95% CI, 22.8%–33.9%) patients experienced FN during any cycle and during AC cycles, respectively.
In conclusion, the incidence of FN during AC-D in breast cancer patients was 29.5%, 25.2% during AC and 4.7% during D chemotherapy. Patients who experienced FN had more occurrences of hospitalization and dose reduction/delays, which may compromise treatment efficacy and quality of life. Further large prospective studies are required to define the exact incidence of FN in Asian patients with this regimen. In add-ition, whether to consider the use of prophylactic G-CSF in Korean breast cancer patients treated with this regimen needs to be validated in future prospective clinical trials.
 XML Download
XML Download