

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The popularity of complementary and alternative medicine (CAM) is rapidly increasing among cancer patients, in particular in ethnic Chinese areas. More than 95% of patients had used CAM after diagnosis of breast cancer, most of them considered that they had benefited from CAM [1,2]. CAM is also popular in North America and Western Europe [3-5]. Traditional Chinese herbs and acupuncture are the most popular methods in East Asia.
Acupuncture is an ancient Chinese means of treatment. It is performed using tiny needles to give irritation to the body and help the body cure the disease. It is a vibrant component of Chinese medicine. Acupuncture therapy is commonly used worldwide. In Taiwan, it is more accepted by the public and is part of the health system. Modern research shows that acupuncture can affect most of the body's systems, and has been proven effective in cancer-related pain control and in treating chemotherapy-induced side effects [6-9].
In Chinese medical theory, qi imbues the Universe; it is everywhere; it can be accessed in the human body via acupoints, and acupoints are found along channels. Another puncture point is called the tender point, and is located at a painful site in the human body. Our patient went to see an acupuncturist because she felt left neck stiffness and pain. A left neck mass with a painful sensation was found. The needle punctured the skin and was manipulated directly in the mass, and this was treated as a tender point. Skin nodules were found and spread rapidly one week after acupuncture. As pointed out by this case, we advise that patients should be aware of their cancerous condition and seek a second opinion before undergoing any therapy.
CASE REPORT
The patient, a 54-year-old Taiwanese woman, discovered a left progressively enlarging breast mass more than 6 months previously, and came to our outpatient department. On physical examination, a 4×3 cm protruding irregular hard mass was noted at the left upper breast, as well as mobile and enlarged axillary lymph nodes. Ultrasonography of the left breast was performed, and revealed a 4×2.6 cm, hard and ill-defined mass with an indistinct border at 12 o'clock, 3 cm from the nipple. Mammography also showed an irregular nodule-like asymmetric mass of breast tissue with an indistinct margin at the left upper inner quadrant, associated with clustered microcalcification, and distorting the parenchyma. A bone scan and liver ultrasound were arranged, and revealed negative findings for metastasis. A core needle biopsy proved the invasive ductal carcinoma of the left breast.
She received a left modified radical mastectomy after the diagnosis of left breast cancer. The tumor size was 4 cm with a grade III histological type and lymphovascular invasion. The axillary lymph node dissection showed metastatic carcinoma in 15 out of 24 lymph nodes. The tumor was staged as IIIC (T2N3M0). Adjuvant chemotherapy and radiotherapy were advised due to the high risk of tumor recurrence. She underwent 6 courses of CEF chemotherapy (cyclophosphamide 500 mg/m2, 5-fluorouracil 500 mg/m2, and epirubicin 90 mg/m2) and radiotherapy 50 Gy in 26 fractions. She was given oral chemotherapy (oral form 5-fluorouracil, UFUR) at a maintenance dose to prevent recurrence.
The patient was regularly followed up at our hospital, and a bone scan series was performed one year after surgery. A new lesion was noted involving the fourth anterior right rib, but was more likely a traumatic fracture. However, the possibility of bone metastasis still could not be ruled out.
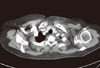
She visited our outpatient department 3 months after the bone scan examination. According to the patient's description, she had a sore left shoulder and sought the advice of an "East Asian Medicine" practitioner 2 weeks previously. Acupuncture was performed once. A left neck mass was punctured as an acupoint using a manipulation method to relieve her pain. The symptom did not improve and multiple skin nodules spread from needled site and radiated to the neck and chest wall rapidly. At the clinical examination, a left neck mass with multiple skin lesions was noted. The chest computed tomography (CT) revealed increasing fatty stranding of the subcutaneous fat and skin thickening at the left supraclavicular and neck regions (Figure 1). Skin biopsy was suggested, and a specimen of about 1×0.5×0.5 cm was obtained (Figure 2A). The pathology report showed metastatic carcinoma in the dermis (Figure 3). Six courses of chemotherapy (paclitaxel and gemcitabine) followed by weekly target therapy (trastuzumab) were given as therapeutic chemotherapy. Then, we shifted to oral chemotherapy and trastuzumab. The neck mass and cutaneous lesions subsided after 2 courses of chemotherapy (Figure 2B). Unfortunately, dizziness and severe headache lasting for one week occurred one year after the left neck recurrence, and she was sent to our ER. The brain CT revealed focal abnormal vasogenic edema in the right occipital region; an underlying non-enhancing hematogeneous metastasis was then considered. Brain magnetic resonance imaging also showed brain metastasis at the right occipital cortical metastasis. The patient expired 3 months later, after palliative radiotherapy followed by chemotherapy.
DISCUSSION
Cutaneous metastasis is relatively rare in invasive breast cancer. Diagnosis of cutaneous metastasis is easy using a skin biopsy. In this case, the origin of the cutaneous metastasis was left neck mass. We arranged chest CT in order to identify the origin and extent of metastasis. The chest CT showed the fatty stranding of the subcutaneous fat and skin thickening at the left supraclavicular and neck regions. No prominent mass lesion was found. We performed skin biopsy and proved the diagnosis. In this case, she was a stage IIIc breast cancer patient with a high risk of recurrence. A nodule at the left neck along with the sore shoulder was the sign of recurrence. Breast cancer patients must always be on the alert for any physical changes. If anything seems different, they should return to their physician for help.
The opportunity for tumor spread from needle tracks (known as "seeding") varies with different types of needle biopsy. Core needle biopsy is a standard procedure in the diagnosis of a breast lesion. It has a shorter operation time and establishes the histological diagnosis, and also provides the patients with the opportunity to be involved in their own therapeutic decision-making. Large-gauge core needle biopsy (11-16 gauge) allows a definitive pathologic diagnosis when a breast mass is discovered. The incidence of needle track seeding ranges from 1.1% to 3.7% [10-12]. The theory of needle track seeding is that there is a presence of displaced tumor cells left after the biopsy procedure [13]. However, epithelial tumor cell displacement has occurred in patients after core needle biopsy, although biopsy methods have shown no statistical difference in local recurrence in recent studies [10-12]. In clinical practice, we routinely excise the puncture wound during breast surgery. Fine needle aspiration cytology also carries the risk of local recurrence from the needle track, but the real probability of these events is difficult to assess [14]. The complications of fine-needle cytology include bleeding and hematoma; tumor recurrence is seldom reported. One report estimated the incidence of needle track seeding to be quite low (0.5/10,000) [15]. The procedure should be performed by a trained team and with negative pressure to avoid seeding.
The acupuncture needle is much smaller than the fine needle. The gauges of the acupuncture needle range from 0.12 to 0.3 mm. To our knowledge, acupuncture related rapid skin spreading has never been reported. The incidence of tumor seeding should be rare because the gauges of the needles are smaller than those of the fine needle, and the tip of the needle is round, without a cutting edge (Figure 4). In this case, the patient received only one acupuncture treatment, and the tumor spread rapidly. However, the manipulations of acupuncture, including repeat punctures, and punctures with twisting upward and downward, increase the incidence of cutaneous tumor spread.
The complications of acupuncture manipulation include local infection, hematoma, vasovagal events, damage to internal organs, spinal cord injury, pneumothorax and hepatitis infection. The side effects can be avoided by a well-trained physician. However, the prevalence of cancer is increasing rapidly, and alternative medicine physicians have less experience dealing with cancer patients. Cancer-related symptoms and signs, including cancer pain, chemotherapy side effects, tumor recurrence and metastasis are not easily identified. When patients seek second opinions or alternative therapy, they should discuss the matter with their surgeon or family physician. Clinical specialists provide rapid evaluation and expert opinions in the management of cancer patients, and acupuncturists provide prompt feedback to their specialists. In clinical practice, physicians must recognize the need to provide such patients with up-to-date information to help them make therapeutic decisions. Acupuncture manipulation is safe and effective only in a situation with well-communicated collaborative care.
Some might doubt that cutaneous metastasis is really related to acupuncture. In fact, we have no direct evidence to prove this. The patient received no intervention except acupuncture before this incident. We do not know what acupoints were needled and what manipulations were used. The patient confirmed the neck mass had been punctured and that skin nodules spread from the needled site. A reasonable explanation is that the metastatic mass ruptured after puncture, and acupuncture initiated some inflammatory reaction and enhanced the cutaneous spreading of tumor cells. Chest CT scan offered some evidence for this theory. The chest CT scan revealed increasing fatty stranding of the subcutaneous fat and skin thickening at the left supraclavicular and neck regions but no mass was found. The rapid development of cutaneous metastasis might be related to her cancer properties and iatrogenic stimulation. Acupuncture is an effective and relatively safe procedure in East Asian medicine. We point out this rare phenomenon to alert patients and physicians to the potential risk of acupuncture. Once again, we emphasize the importance of well-communicated collaborative care.
In Taiwan, there are two types of acupuncturists, some of whom are "folk healers" and some of whom are fully trained professional acupuncturists. Folk healers treat disease based on their Oriental theories. They are not educated in modern biomedicine. On the other hand, professional acupuncturists are fully trained in acupuncture theory and modern oncology knowledge. From the professional acupuncturist's point of view in this case, the acupuncturist should have referred her back to her physician or built up good communication with her physician. However, some folk healers and aged professional acupuncturists have not updated their medical knowledge and so some legal problems might come up.
In addition, patients should be aware of their cancerous status, and explain their condition before any new therapies. This patient might have been shy about her cancerous condition, and did not tell the truth to the acupuncturist, or she may have had no insight into cancer. Active communication between practitioner and patient is essential in current medical situations. Cancer patients can get maximal benefits from it.
In conclusion, our case showed that breast cancer patients may use East Asian Medicine in addition to standard Western medical care. The use of East Asian Medicine by patients with breast cancer is increasing, but research on its safety and effectiveness is seldom evaluated. A well-communicated collaborative care is important when patients are looking into East Asian Medicine -- this will provide information about breast cancer risk and help in making correct therapeutic decisions.



 XML Download
XML Download