

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Henoch-Schöenlein purpura is a vasculitic syndrome that occurs most commonly in prepubertal children, and is typically characterized by a purpuric rash on the lower extremities, abdominal pain and joint symptoms1. Although renal involvement is frequent, pulmonary involvement is rare; when present pulmonary abnormalities significantly increase mortality2. This report presents a case of pulmonary hemorrhage and renal involvement in a 46-year-old male with the diagnosis of HSP. The patient responded to prednisolone therapy. Here we present the case and review the medical literature.
Case Report
A 46-year-old male presented with pulmonary hemoptysis and a purpuric rash on the extensor surface of the lower extremities and complained of knee joint pain. He was treated with oral prednisolone 7.5 mg p.o. b.i.d. for the skin rash. However, two days later he complained of abdominal pain. His medical and family history were unremarkable. His blood pressure was 140/90 mmHg, temperature 36.5℃, heart rate 82/min, and respiratory rate 24/min, and he had clear lung sounds without rales or wheezing. The physical examination showed a purpuric rash on the extensor surface of the lower extremities and buttocks. Both knee joints were slightly swollen, but otherwise his examination was within normal limits.
The laboratory tests showed: hemoglobin 14.1 g/dL, platelets 281,000/µL, white blood cells (WBC) 14,000/µL, prothrombin time 12.1 sec, activated partial thromboplastin time 25.4 sec, serum sodium 140 mEq/L, potassium 4.3 mEq/L, urea 14 mg/dL, and creatinine 1.0 mg/dL. His C3 was 104 mg/dL, C4 29.3 mg/dL, and antinuclear antibody (ANA) 2.0 IU/L, but he was negative for antineutrophil cytoplasmic antibody. The urinalysis had no protein, red blood cells 11~20 per high-power field (HPF), and WBC 0~2 per HPF.
Chest X-ray revealed an ill-defined nodular opacity at the right middle lung zone and minimal reticulonodular infiltration at the right upper lobe apex (Figure 1). The chest computed tomography showed a partially calcified nodule with a fibrotic linear opacity at the right apex and an enhanced wedge-shaped lobulated mass at the superior segment of the right lower lobe of the lung (Figure 2). The bronchoscopy findings were negative.
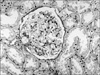
The percutaneous kidney biopsy showed a normal looking glomerular architecture (Figure 3). However, immunofluorescent microscopy showed mild mesangial Ig A deposits in the mesangium of glomeruli, consistent with Henoch-Schöenlein purpura nephritis (grade I according to the Counahan grading system) (Figure 4).
The patient received prednisolone 20 mg p.o. o.d. for seven days and his hemoptysis and purpura of the lower extremities improved. One week later, his chest X-ray showed that the longitudinal mass at the right lower lobe was diminished in size.
Discussion
Henoch-Schöenlein purpura is a vasculitic syndrome of unknown cause, and is usually a mild, self-limited disease that most commonly affects children between two and 10 years of age; however, it can occur in older children and adults3. Serious complications of this syndrome usually involve the kidney and occasionally the gastrointestinal tract, whereas clinically important pulmonary complications are rare.
The pathologic process of lung involvement in HSP is derived from immune mediated vasculitis processes, requiring differential diagnosis with other systemic vasculitic disorders. Especially, localized lung involvement can be presented in Wegener's granulomatosis and Churg-Strauss syndrome4, contrary to diffuse parenchymal involvement more commonly in cases of microscopic polyangitis, Bechet's disease, drugs, systemic lupus erythematosus, antiphospholipid antibody syndrome, polymyositis, IgA nephropathy, rheumatoid arthritis, Goodpasture's syndrome, and bone marrow transplantation5. In cases of HSP, localized lung involvemet is less common.
The differential diagnosis of HSP requires careful observation. This case showed a normal ANA level, indicating a less than 0.14% chance of having SLE6 and his complement levels were normal. Even though Wegener's granulomatosis is so difficult to differentiate from HSP during early stages of disease7, it could be excluded based on the normal ANCA level and the presence of renal Ig A deposits.
Pulmonary hemorrhage in HSP has been associated with a high morbidity and mortality5. Sixteen cases have previously been reported in the medical literature8. Of these 16 patients, five subjects recovered but six died due to pulmonary hemorrhage and four had no followed up information. The majority of cases of HSP with pulmonary hemorrhage reported in the literature were older and had more severe multiorgan involvement than the typical pediatric case of HSP.
The principal cause of pulmonary hemorrhage in HSP is vasculitis of small pulmonary blood vessels, especially capillaries9-11. Corticosteroids have been used with the hope of ameliorating the vasculitis, but efficacy has not been established. There was a report showing improved outcome with combined therapy of cytotoxic drugs together with pulse methylprednisolone. A combination of pulse methylprednisolone and other cytotoxic agents including cyclophosphamide or azathioprine may achieve a better outcome12.
In conclusion, we report an adult case of HSP with pulmonary hemorrhage, hematuria and skin purpura who achieved complete recovery after steroid therapy. Pulmonary hemorrhage due to HSP should be considered when hemoptysis is accompanied by purpura of the lower extremeties and or hematuria.



 XML Download
XML Download