

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Rapid palatal expansion (RPE) has been used as an effective treatment modality for growing patients since its first introduction by Angell1 in 1860. For adults, because of increased resistance from the bony palate and zygomatic buttress,23 surgically assisted RPE (SARPE) has been proposed and used. However, SARPE is associated with several limitations, including additional expenses and surgical morbidity. Two-stage surgery involving SARPE followed by double-jaw orthognathic surgery may be indicated for adults with both anteroposterior and transverse maxillary deficiency.4
The morphological development of the midpalatal suture can be divided into three stages.5 The suture begins as a short, broad, Y-shaped structure, which becomes more sinuous in the second stage and undergoes heavy interdigitation in the third stage. Although it was once believed to be obliterated during the juvenile period, histological studies have shown that the midpalatal suture rarely shows a marked degree of closure before the third decade of life.67 Moreover, a radiologically invisible suture does not indicate histological fusion or closure.7 Consequently, nonsurgical RPE may be a feasible treatment protocol for young adults with a patent suture.8
Nonsurgical RPE can be achieved with conventional (C-RPE), bone-borne (B-RPE), or combination-type palatal expanders. Lin et al.9 reported that B-RPE produced greater skeletal effects and fewer dentoalveolar side effects compared with C-RPE in late adolescence. In addition to several reports of successful nonsurgical expansion using C-RPE in young adults,810 Lee et al.4 reported miniscrew-assisted RPE (MARPE) using a combination-type device for the delivery of an expansion force directly to the basal bone.
Nevertheless, even in the presence of patent sutures, nonsurgical RPE can produce unwanted effects when used for skeletally mature patients, such as lateral tipping of the posterior teeth, buccal root resorption, and fenestration of the buccal cortex.21011 Excessive stress can be concentrated on the maxillary buccal cortex because of the increased rigidity of the maxillary articulations with the face.
For visualization and quantification of the initial displacement and stress distribution caused by an orthodontic force, finite element analysis (FEA) effectively produces a three-dimensional (3D) computational model to analyze the stress and strain distributions and simulate various appliance conditions.12
Recently, a study using 3D FEA recommended the use of B-RPE with miniscrews located at the palatal slopes and a resin plate, because it resulted in the least stress concentration around the dentition and buccal plates and produced fewer dentoalveolar side effects.13 However, in that study, the efficacy of maxillary expansion with regard to the amounts of transverse displacement of the maxillary halves and the dentoalveolar unit was not considered. To our knowledge, few studies have investigated the efficacy of maxillary expansion in young adults according to the patterns of stress concentration and distribution with various devices, including C-RPE, B-RPE, and MARPE devices, using 3D FEA. In spite of the diversity of appliance designs, evidence regarding the mechanical effects of each device on the circumaxillary structures has been scarce, particularly for Korean adults.
The aim of this study was to evaluate the stress distribution and displacement of dental and craniofacial structures upon the use of respective C-RPE, B-RPE, and MARPE for young adults using 3D FEA.
MATERIALS AND METHODS
Construction of the finite element model
The dry skull of a 20-year-old man was scanned using computed tomography (CT). The skull, excluding the mandible, was inspected for gross defects and discontinuities in the craniofacial anatomy. Sequential CT images were acquired at 2-mm intervals in the axial direction, parallel to the Frankfort plane. Images were reconstructed layer by layer to create the 3D FEA model. Given the complexity of the bone structures and their interactions with the surrounding structures via sutures, the simplifications introduced by Tanne et al.14 were applied to the model. On the basis of previous studies assessing the cranial sutures,7 the suture thickness was uniformly set at 0.2 mm (Figure 1A).
The Nissin dental model (Nissin Dental Products, Kyoto, Japan) from a sample survey of adults with normal occlusion was subjected to 3D scanning and constructed. The dental arch was arranged in the broad arch form from Ormco (Glendora, CA, USA), and the inclination and angulation of each tooth were set according to the prescription by Andrews.15 The periodontal ligament thickness was uniformly set at 0.25 mm, in accordance with the studies by Coolidge16 and Kronfeld.17 Under the assumption that its condition was normal, the alveolar bone was built up at 1 mm away from and along the curvature of the cementoenamel junction.
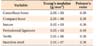
Because this study was designed to investigate the initial reaction to an orthopedic expansion force, the teeth, alveolar bone, periodontal ligament, suture, and supporting wire were assumed to be homogeneous, isotropic, and linearly elastic. The mechanical properties of the components of the model were obtained from experimental data reported in previous studies1819 (Table 1).
Appliance designs and experimental conditions
The following RPE devices were designed to examine the effects of tooth- or bone-borne RPE, with a miniscrew length of 7 mm (Figure 1B).
C-RPE utilized a tooth-borne device. A conventional hyrax expander incorporating the first premolars and first molars was designed for this purpose.
B-RPE utilized a bone-borne device (expander screw with four miniscrews only). Four rigid connectors made from stainless steel wire (0.8-mm diameter) were soldered on the base of a hyrax screw body and connected to four orthodontic miniscrews (2.0-mm diameter, 7-mm length). Two of the miniscrews were positioned in the rugae region between the central and lateral incisor roots, while the other two were placed in the parasagittal area.
MARPE utilized a combination-type device (tooth- and bone-borne device with four miniscrews). The expander had connectors to both the teeth and the miniscrews. The positions of the miniscrews were the same as those in the B-RPE device.
Finite element analysis
ANSYS version 10.0 (Swanson Analysis System of USA, Canonsburg, PA, USA), a general program for the interpretation of finite elements, was used to analyze the force system. The components used for model construction were configured as a regular tetrahedron, with 41,480 model elements and 158,070 nodes. The foramen magnum, which formed the base of the model, was constrained in its displacement by the X, Y, and Z directions.
The C-RPE appliance used in this study was the hyrax type. Each turn of the screw induced a 0.2-mm separation of the midpalatal suture. The force ranged between 3 and 10 lbs, with multiple turns generating loads that were > 20 lbs.20 The stress and displacement produced by each appliance were analyzed with one turn of the screw and a maximum force of 10 lbs.
Displacements were measured in the x-, y-, and z-axes (transverse, anteroposterior, and vertical axes, respectively). Displacement in the medial, posterior, and superior directions was represented by a positive (+) value. The internal stress reaction was measured by the von Mises stresses (g/mm2). The stress distribution was presented by color contour bands, where different colors represented different stress levels in the deformed state. Positive or negative values in the stress spectrum column indicated tension or compression, respectively.
RESULTS
Stress distribution over the circumaxillary structures
Figure 2A and 2B and Table 2 show the distribution of stresses produced by activation of the RPE appliance over the various sutures and bones in the craniofacial complex. C-RPE resulted in high stress values for the buccal plate of the anchor teeth (first premolar, 196.2 g/mm2; first molar, 174.5 g/mm2) and the frontal process of the maxillary bone (224.7 g/mm2); this increased stress was capable of causing side effects during maxillary expansion. With B-RPE, the stress was highly concentrated around the miniscrews (1,899.9 g/mm2) and was not transferred effectively to the basal bone or the sutures. With MARPE, the maximum stress (558.6 g/mm2) was concentrated around the miniscrews. However, the stress was distributed with relative uniformity among the circumaxillary structures. Compared with the values observed with C-RPE, the stress values around the buccal plate were reduced by 37% at the first premolar (124.5 g/mm2), 65% at the first molar (62.5 g/mm2), and 17% (186.5 g/mm2) at the frontal process of the maxillary bone.
von Mises stress distribution over the sutures
The maximum von Mises stresses were concentrated at the midpalatal, palatomaxillary, frontomaxillary, zygomaticomaxillary, and palatosphenoid sutures (Figure 2C and Table 2). With B-RPE, although the maximum stress was observed at the midpalatal and palatomaxillary sutures (48.2 g/mm2 and 36.2 g/mm2, respectively), the stress was locally concentrated and was not distributed throughout the sutures. Although the maximum stress values for the midpalatal and palatomaxillary sutures (22.0 to 22.5 g/mm2 and 20.2 to 20.5 g/mm2, respectively) were lower with C-RPE and MARPE than with B-RPE, the former two appliances resulted in relatively uniform stress distribution throughout the sutures.
Displacement of anchor teeth
Displacement of the anchor teeth was measured along the x-, y-, and z- axes, with positive values set for displacement in the medial, posterior, and superior directions. Displacement was analyzed by determining the coordination between and distance moved by the midpoint of the incisal edge and root apex of the central incisor, the buccal cusp tip and buccal root apex of the first premolar, and the mesiobuccal cusp tip and mesiobuccal root apex of the first molar (Table 3).
Very little dentoalveolar effects were observed with B-RPE, as the appliance was not connected to the anchor teeth (Figure 3A). C-RPE and MARPE showed similar displacement patterns for the anchor teeth. The maximum displacement was observed in the transverse plane as buccal tipping of the first premolar (cusp tip, −9.69E-03 to −1.05E-02 mm; apex, 2.52E-04 to 3.96E-04 mm) caused by the transverse expansion force. Lateral tipping of the first molar (cusp tip, −7.40E-03 to −4.34E-03 mm; apex, −4.80E-04 to −2.20E-04 mm) was also observed with C-RPE and MARPE. However, compared with that caused by C-RPE, the buccal tipping tendency of the anchor teeth was effectively reduced with MARPE, indicating that the ratio of the first molar cusp tip-to-apex displacement was 1:0.03 with C-RPE and 1:0.11 with MARPE (Figure 3B). The displacement pattern in the y- and z-axes was related to the downward and forward displacement of the maxilla caused by RPE treatment.
Comparison of the stress distribution among the three devices
To evaluate the effects of each device, the stress distribution pattern and maximum von Mises stresses for specific areas were compared among devices (Table 4). The B-RPE device was expected to be the ideal device without any side effects for nonsurgical RPE in adults. However, the expansion force generated by the screw was concentrated on a small area around the miniscrews and was not transferred to the basal bone. The maximum stress value was extremely high and was localized at the middle of the midpalatal suture. With MARPE, although the maximum stress was observed around the miniscrews, the value was much smaller than that with B-RPE. Moreover, the von Mises stress was evenly distributed throughout the midpalatal suture. Stresses on the buccal plates of the first premolar and first molar were decreased by one-third compared with those induced by C-RPE.
DISCUSSION
The prerequisites for successful maxillary expansion in adults may include both effective force delivery to the midpalatal suture and generation of minimal stress around the buccal plate of the anchor teeth. In the present study, 3D FEA showed that C-RPE exhibited significant force transduction on all the circumaxillary sutures, although one of the highly stressed areas was the buccal plate of the anchor teeth, implying unwanted side effects during maxillary expansion in adults. Carvalho Trojan et al.21 also reported that only one turn of the jackscrew in the C-RPE device resulted in maximum stress peaks of 1.5 to 2 MPa in the buccal plate of the anchor teeth, at the beginning of the zygomatic process of the maxilla, at the nasal floor, and on the inner walls of the nasal cavity.
With MARPE, the maximum stress value of 558.6 g/mm2 was concentrated around the miniscrews, but the stress value was much lower than that with B-RPE. The stress was evenly distributed throughout the midpalatal suture and decreased at the buccal plate of the anchor teeth. The addition of miniscrews may have moved the resultant vector of the expansion force closer to the center of resistance of the basal bone.22 Consequently, compared with C-RPE, MARPE secured significant expansion of the anchor teeth to the buccal side with decreased buccal tipping.
B-RPE was expected to be an effective alternative to eliminate the excessive stress on the buccal plate. However, this particular appliance concentrated the stress around the miniscrews only and the force transduction along the suture was scarce; this could lead to failure of the miniscrew and subsequent failure in splitting the suture.21 It is difficult to find a report where a true B-RPE has been successful in adults. Therefore, a theoretical basis for its inability may be provided according to the results of the present study. Considering that the shape of the maxillary bone is triangular and fixed at the proximal side, forces applied at the tooth level are expected to create a greater bending moment near the region of the midpalatal suture.23 This leverage action may be helpful in splitting the suture. In contrast, an extremely high force must be required with the B-RPE to separate the suture, because the point of force application near the proximal area would create a considerably lesser bending moment under a given magnitude of force. Taken together, a MARPE is considered as an effective combination of these two extremes, considering it delivers an efficient expansion force and decreases unwanted side effects on the buccal plate of the anchor teeth.
In a study about the effects of miniscrew orientation on the stability and resistance to failure, the maximum force at failure was 87 ± 27.2 N to 342 ± 80.9 N in the human mandible.24 The vector of the shear force and the long axis of miniscrews affect the values. The physiological threshold of the bone strain for the maxilla has not been determined yet, although strain is related to the stress and the area of the force applied.25 If accumulated strain caused by multiple jackscrew turns exceeds the physiological strain limits, marginal bone loss would occur as a result of mechanical stress and lead to miniscrew failure.26
The method of connecting miniscrews to the device for clinical application should be considered. In our finite element model, miniscrews were connected to the RPE device using 0.8-mm stainless steel wires, and the entire setup was assumed to function as a single unit without loss of expansion force to the conjunction area. The efficiency of the expansion force delivered to the miniscrews would be decreased according to the miniscrew position, length of the connecting wire, and the solidity of the junction between the wire and the miniscrews. The axis of the miniscrews and the direction of movement of the connecting wire during RPE should be considered while designing the appliance.
The MARPE device is a simple modification of the C-RPE device. The main difference is the incorporation of several miniscrews to ensure expansion of the underlying basal bone and maintain bone separation during the consolidation period. Miniscrew placement is a simple procedure that does not require osteotomy. At the time of selecting the number and location of miniscrews, one must consider whether the connected miniscrews would be able to withstand the expansion force. An appropriately designed appliance would be helpful to minimize the side effects of C-RPE while maintaining the efficiency of the expansion force in adults. The results of the present study and those of previous studies suggest that MARPE is an effective treatment modality for transverse deficiency in young adults from the late teens to young adults.23
FEA permits the simulation of clinical orthodontic systems for the study of biomechanical variables induced by various external forces in a 3D space. The accuracy of the results depends on the accuracy of the modeling procedure, element density, and material properties. In the present study, skull modeling was performed using data from individualized CT images, which were acquired at 2-mm intervals for good continuity and accuracy. The maxillary dentoalveolar arch, orthodontic miniscrews, and RPE appliance were artificially added to the whole skull model with the appropriate proportional relationship.
Because of the complexity of bone structures and the extensive network of sutures, the exact mechanical properties of sutures at each stage of human development are not well defined. Recent reports of the nanomechanical properties of rat cranial sutures assessed using atomic force microscopy (AFM) indicated that the elastic moduli of such sutures vary from 0.64 to 1,371 MPa.27 Using nanoindentation by AFM, Radhakrishnan and Mao28 demonstrated that the average elastic moduli of the zygomaticotemporal, nasofrontal, and premaxillomaxillary sutures in rabbits were 1.20, 1.16, and 1.46 MPa, respectively.
The degree of ossification of the circumaxillary sutures can affect the material properties. Several studies have examined the mechanical properties of unossified,29 completely ossified,30 and partially ossified sutures. Provatidis et al.18 suggested an elasticity modulus of 500 MPa for partially ossified sutures. The material properties of craniofacial sutures also vary according to the region of ossification. Assigning appropriate values to the material properties for each condition is technically difficult, and slight variations in these values may not significantly affect the overall displacement and stress distribution patterns. Therefore, in the present study, the craniofacial sutures were assumed to be isotropic, homogeneous, and linearly elastic, and the elastic modulus was determined on the basis of a previous study using a similar skull model.18
Research on the physical properties of living structures is not yet adequate. Errors caused by deformations of the bone and appliances and the effects of soft tissues were not considered. Future studies should aim to model the suture as a viscoelastic material with hardening properties and under growing conditions. Nevertheless, when supplemented with clinical, cytological, and biochemical research, the results from this study may be effectively applied in the clinical field.
Our results provide additional explanations about the mechanical reactions of the bony tissue, which are the first step in the complex process of tissue response to an expansion force. The findings can aid in elucidating the therapeutic effects of appliances and their mechanisms of action on the basal bones and sutures of the craniofacial complex.
CONCLUSION
In conclusion, C-RPE induced high stress around the buccal plate of the anchor teeth and the frontal process of the maxillary bone, but not in the midpalatal suture area, which was presumed to cause side effects during maxillary expansion. In contrast, with B-RPE, the maximum stress was localized around the miniscrews, with limited stress distribution visualized within the suture. As a combination of the C-RPE and B-RPE devices, the MARPE device showed a relatively even stress distribution and decreased stress on the buccal plate of the anchor teeth. Therefore, it can be implicated that the role of the miniscrews in the MARPE device is to secure sufficient expansion in the dentoalveolar area with minimal tipping while effectively decreasing the pressure on the buccal plates of the anchor teeth. Considering the rigidity of the craniofacial structure in adults, MARPE may serve as an effective treatment modality to deliver an expansion force and minimize any unwanted force on the dentoalveolar complex in young adults with transverse maxillary deficiency.






 XML Download
XML Download