

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Oral diseases and disorders can negatively affect a child's life.1 Normal tooth alignment contributes to not only the oral health but also the overall well-being and personality of children. Malocclusion and caries are among the most common chronic dental diseases in childhood.2,3 These conditions have increased the demand for orthodontic and restorative treatments in most countries.
The etiology of malocclusion is multifactorial: the dentofacial structure is mainly determined by genetic factors and environmental factors such as habits can induce malocclusion during growth and development.4 Caries and premature loss of primary teeth are considered predisposing factors for occlusal and space anomalies in the mixed and permanent dentitions.5 Nevertheless, previous attempts to investigate the association of malocclusion and caries yielded conflicting or inconclusive results.5-7
The present study was designed to assess the prevalence of malocclusion in school children aged 11 - 15 years in Kanyakumari District, Tamil Nadu, India, by using the Dental Aesthetic Index (DAI) and determine its relationship with caries.
MATERIALS AND METHODS
Subjects
The ethical committee of Rajas Dental College approved the study approved the study, and permission to survey the various schools was given by the chief education officer and director of Public Health, Kanyakumari District.
The initial sample was designed to contain 1,500 subjects who had never undergone orthodontic treatment with 300 children in each of the chronological ages from 11 to 15 years. To overcome the error associated with cluster sampling, the final sample size was fixed at 1,800 subjects. Subjects were examined from 18 (12 public and 6 private) randomly selected schools. By using random number tables, 20 students per class from grades 6 to 10 were invited to participate in the study. Parents provided written consent for the participating students.
Measurements
For determining malocclusion, the standard DAI components8 were recorded as described by the World Health Organization (WHO)9 using a community periodontal index probe, mouth mirror, and ruler. The numbers of decayed, missing, and filled teeth (DMFT) were also computed according to the WHO recommendations.9 Before data collection, two examiners (JKB and CRB) were trained and calibrated by an orthodontist (AT) to ensure interexaminer reliability. The kappa statistics of interexaminer and intra-examiner consistency were 0.84 and 0.91, respectively, for the DAI scores and 0.82 and 0.84, respectively, for the DMFT scores.
The socioeconomic status (SES) was determined on the basis of the Standard of Living Index10 and self-reports of parental income, possession of goods, and household facilities. According to the index scores, the subjects were divided into the high-, medium-, and low-income categories. Further, regarding the daily consumption of cariogenic foods, the students completed a questionnaire including dichotomous measures (yes/no) on the intake of foods such as chocolate, ice cream, toffee, pastry, cakes, biscuits, dates, and carbonated drinks as well as sugared tea, coffee, and milk. The frequency, mode, and preferred time of eating and drinking were recorded. According to the median values of the total dietary scores, the subjects were categorized into the high- and low-risk groups. Data reduction was performed to avoid co-linearity problems obscuring the results.
Statistical analysis
The data were analyzed with PASW for Windows ver. 17.0 (IBM SPSS Inc., Armonk, NY, USA). The chi-square test was used to analyze gender differences in the DAI scores. ANOVA was applied to assess the differences in the distributions of the mean DMFT and DAI scores across the age groups. Multiple comparisons were performed by using the Bonferroni adjustment. The Spearman rank-order correlation coefficient (r) was used to measure the correlation between the DMFT and the DAI scores. A significance level of 5% was adopted.
RESULTS
The sample consisted of 1,042 (57.9%) boys and 758 (42.1%) girls. More than half (55.8%) of subjects lived in rural areas and about 40% belonged to the medium-income group. In terms of daily cariogenic food consumption, about 16% of the children belonged to the high-risk group.
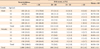
The mean DAI score was 18.61 ± 6.1, and no significant differences were observed between the gen ders and among the age groups (Table 1). About 85% of the students (83.0% boys and 86.8% girls) had mean DAI scores of < 26, thus not requiring orthodontic treatment (Table 1). One-tenth of the sample had mean DAI scores between 26 and 30, indicating definite malocclusion and elective treatment, and about 3% had mean scores between 31 and 35, indicating severe malocclusion with desirable treatment. Only 29 (1.6%) children (16 boys and 13 girls) had mean DAI scores above 35, indicating handicapping malocclusion requiring mandatory treatment.
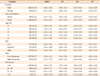
The gender distribution of the 10 DAI components is shown in Table 2. Incisal crowding was the most common malocclusion (41.2%), followed by maxillary overjet of > 2 mm (14%) and incisal spacing (12.4%). Girls had significantly (p < 0.01) higher mean DAI scores with respect to incisal crowding and boys had significantly higher mean DAI scores for mandibular overjet and anterior open bite (p < 0.01).
The mean DMFT score was 2.28 ± 1.47 and 91.8% of the subjects had a DMFT score of > 0. Caries was clinically evident in 82.3% of the students. Table 3 shows their mean DMFT, decayed teeth, missing teeth and filled teeth scores. No significant differences in the caries experience were noted between the genders and between the urban and the rural dwellers. The 13 year olds had higher, but not significant, mean DMFT scores. Further, children belonging to the medium-income and high-risk groups had significantly (p < 0.001) higher mean DMFT scores. Children with mean DAI scores of >35 were found to have a significantly (p < 0.001) higher caries experience. The mean DAI scores showed a significant correlation with the mean DMFT scores (r = 0.368, p < 0.05).
DISCUSSION
This study was conducted as part of a large school dental health program in Kanyakumari District. Considering that studies on the prevalence of malocclusion should be large enough and cover non-orthodontically treated children,11 the moderately large sample of this study seems to satisfy those requirements.
Many population-based indices have been developed to assess malocclusion, such as the commonly used DAI and Index of Orthodontic Treatment Need (IOTN).8,12-15 The DAI is relatively easy to use and identifies deviant occlusal traits, and links clinical and aesthetic components mathematically to produce a single score, unlike the IOTN.16 The structure of the DAI consists of 10 prominent traits of malocclusion, weighted on the basis of their relative importance. This study used DAI as it has not only been adopted by WHO but also been validated in India.17
The prevalence of malocclusion in India reportedly ranges from 20% to 43%.18 In this study, 85% of the children aged 11 - 15 years require no orthodontic treatment. The percentage of children with handicapping malocclusion requiring mandatory treatment was less than 2%. These results are in agreement with the findings of other Indian studies.6,19
Gender-specific analysis of the DAI components revealed that the prevalence of incisal crowding was significantly higher among girls. Numerous other studies have reported similar gender differences.20,21 This result is attributable to the fact that girls have inherently smaller jaws, leading to crowding. Contrarily, in the Ng'ang'a et al.22 study, boys had a higher prevalence of crowding. In the present study, although a significantly higher number of boys than girls had mandibular overjet and anterior open bite, the prevalence was low.
Incisal crowding and maxillary overjet of > 2 mm were the most common DAI components, as previously reported.5 Crowding is caused by a discrepancy between tooth and jaw sizes or by the influence of functional factors on the development of the dentition. Seemann et al.23 found a significant relationship between anterior crowding and the habitual open mouth posture in the early mixed dentition. In the mixed dentition, premature loss of primary teeth and caries in the supporting zones associated with such loss could also cause crowding.21
In this study, no significant difference in the overall DAI score was observed among the age groups. In some studies, malocclusion was more prevalent in the mixed dentition than in the primary dentition.23 This could be because the remaining primary teeth may be loose and permanent teeth may be erupting in the mixed dentition period. Further, at this stage, a physiologic increase in spacing and overjet occurs, which decreases with the maturation of the arches.
Daily cariogenic food intake and the SES were found to be significantly associated with the mean DMFT scores. Regular consumption of cariogenic food contributes to the development of caries.24 The high-risk group had a higher caries experience than the low-risk group. Students belonging to the 'low-income' group had the least mean DMFT scores whereas those classified into the 'medium-income' group had the highest. However, the SES and daily cariogenic food intake were not significantly associated with the mean DAI scores. This finding is in contrast to a previous study, where orthodontic treatment was reported to be more commonly needed by socially deprived children than by their affluent counterparts.25 The previous result may be because children having a high SES are more likely to undergo timely orthodontic treatment.26
Children with DAI scores of > 35 were found to have a significantly higher caries experience, as previously reported.27,28 Borzabadi-Farahani et al.28 reported a higher caries experience in subjects with DAI scores of > 30, although this relationship was not significant. Moreover, Stahl and Grabowski21 reported no significant correlation between malocclusion and caries experience in the mixed dentition period, but specific types of malocclusion were found to be more prevalent in individuals with a high caries experience.
The present study has some limitations. Both the DAI and the IOTN include aesthetic and anatomic components of malocclusion,29 but the IOTN is reportedly more accurate.27 The DAI was preferred in this study because several local studies have used this index to report the prevalence of malocclusion.6,19 This enables comparability of findings among similar studies. The low percentage of children with high DAI (> 35) scores precludes drawing firm conclusions regarding a group correlation. Further, the SES variables used may differ from those in other studies, and therefore, the results may not be generalized. Finally, the measurement of daily cariogenic food consumption depended on the subjective recall ability, which increases the potential for bias.
CONCLUSION
The positive correlation between the severity of malocclusion and the caries experience is an important finding of this epidemiologic survey. Incisal crowding and maxillary overjet are the most common orthodontic anomalies in these students. The majority of the population studied does not require any orthodontic interventions, but their caries incidence seems to be high. Although this study was not aimed at assessing the causal relationship between malocclusion and caries, the findings provide valuable information on the prevalence of malocclusion and caries in this population.

 XML Download
XML Download