

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Co-administration of two or more antimicrobials with anti-anaerobic activity is not recommended except in certain circumstances. Unnecessary double anaerobic coverage (DAC) has been related to increased hospital costs, risk of drug-resistant pathogen acquisition, and development of adverse reactions [123]. Clindamycin use is one of the well-known predisposing factors for development of Clostridium difficile infection [4]. In previous research examining the prescription of metronidazole in combination with other anti-anaerobic agents, 23.4 to 43.8% of days of therapy and 49.4% of prescriptions were considered unnecessary [567]. These results show the necessity of stewardship intervention to reduce unnecessary DAC.
To reduce the number of patients receiving unnecessary DAC, an intervention was initiated in July 2013, at Seoul National University Bundang Hospital. This study was conducted to estimate the impact of the intervention on prescription of unnecessary DAC.
Materials and Methods
1. Study setting and description of intervention
This study was conducted at Seoul National University Bundang Hospital, Seongnam, Republic of Korea, which is a tertiary, teaching, and referral hospital with 1,100 beds at the time of the study.
The DAC in this study was defined as a combination therapy with one of metronidazole or clindamycin and one of beta-lactam/beta-lactamase inhibitors, cephamycins, carbapenems, or moxifloxacin.
The intervention consisted of two parts. The first was education using the institutional intranet. The second was prospective audit and feedback provided through collaboration between a pharmacist and an infectious diseases physician.
The education was performed through e-mail, sent via the institutional intranet. At the beginning of the intervention (early July 2013), the e-mails were sent to physicians in the name of the infectious diseases department and antimicrobial management committee. Then, e-mails were sent to individual clinical departments once again. The infectious diseases physician communicated with the members of individual departments by e-mail about this issue. These e-mails explained the meaning of DAC, the institution's status about the issue, the details of the intervention, and the list of exceptional circumstances in which DAC could be considered appropriate or necessary.
The prospective audit and feedback was performed via consultation notes. This part was implemented by the antimicrobial stewardship team, which consisted of a pharmacist and an infectious diseases physician. The roles of the pharmacist included (1) screening the patients receiving DAC on a daily basis, (2) reviewing medical records and assessing the appropriateness of DAC, and (3) making the singed consultation notes on patients' progress notes when the prescription was not in the list of exceptional circumstances. The consultation notes covered the details of current DAC, presumptive indication, list of exceptional circumstances, and opinions and recommendations, in this order. If the screened patients were not in the hospital, the consultation notes were written for educational purposes. The infectious diseases physician reviewed the preformed consultation notes and co-signed them.
The list of exceptional circumstances in which DAC was considered appropriate or necessary included (1) metronidazole use for the treatment of C. difficile infection, (2) metronidazole use for the treatment of infections in which metronidazole is the drug of choice, such as Trichomonas vaginalis infection, amebiasis, and giardiasis (3) adjuvant clindamycin use in the treatment of toxic shock syndrome, (4) clindamycin use in the treatment of pneumocystis pneumonia, and (5) certain cases of complicated intra-abdominal infections based on recommendations of infectious disease specialists. Except for these circumstances, all episodes of DAC were considered unnecessary.
2. Study period and patient selection
The study period was 1 year, in which the pre-intervention period covered 6 months (from January 1 to June 30) and the intervention period covered the remaining 6 months (from July 1 to December 31) in the year 2013.
Study subjects were all inpatients and outpatients in our institution who received DAC (including discharge prescriptions) during the study period. In the case of outpatient or discharge prescriptions, we considered the number of days of prescription as days of therapy. Patients in the pediatric department were excluded.
3. Study measures
The primary outcome was the number of patients receiving unnecessary DAC and the proportion of patients receiving unnecessary DAC among patients receiving necessary or unnecessary DAC.
Since the intervention consisted of two parts, estimation of the impact of the intervention was also performed in accordance with the detailed parts of the intervention. A schematic diagram of the study shows the indicators and the timing for estimation of the effect of intervention in Figure 1.
First, to estimate the effect of education, we compared the monthly number of patients identified as receiving unnecessary DAC at screening (receiving unnecessary DAC at day 1, the day of screening). The proportion of these screened subjects among all patients receiving DAC was also assessed.
Subsequently, we investigated the number of patients receiving unnecessary DAC for more than 3 days after screening. To estimate the effect of prospective audit and feedback, we compared the proportion of these patients among the patients identified as receiving unnecessary DAC at screening.
Then, to estimate the overall effect of the intervention on unnecessary DAC prescription, we compared the monthly number of patients receiving unnecessary DAC for more than 3 days after screening and the proportion of these patients among all patients receiving DAC.
Compliance with consultation notes was assessed on the third day after screening (day 3). If the unnecessary DAC was stopped before this day, we considered that the attending physicians had complied with the recommendations.
4. Statistical methods
The Wilcoxon rank sum test was used to compare the monthly number of patients receiving unnecessary DAC. To compare the proportions of unnecessary DAC and the changes between day 1 and day 3, a chi-square test was used. All statistical analyses were performed using R version 3.1.2. A P-value of <0.05 (two-tailed) was used to establish statistical significance.
Results
The number of patients receiving DAC regardless of appropriateness was 380 in the pre-intervention period and 307 in the intervention period. Moreover, the number of patients receiving DAC prescription considered appropriate or necessary was 172 in the pre-intervention period and 201 in the intervention period. The most common situation in which these prescriptions were considered appropriate or necessary was C. difficile infection. The number of patients receiving DAC because of C. difficile infections was 169 in the pre-intervention period and 196 in the intervention period. There was no significant difference in the median monthly number of C. difficile infection before and after the intervention (Wilcoxon rank sum, P = 0.809).
The remaining 3 patients in the pre-intervention period received DAC because of toxic shock syndrome. Among the remaining 6 patients in the intervention period, 3 patients received DAC because of pneumocystis pneumonia, 2 because of the infectious disease physician's recommendation, and 1 because of toxic shock syndrome.
Figure 2 shows the monthly number of patients receiving necessary or unnecessary DAC.
1. Effect of education
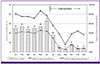
The number of patients identified as receiving unnecessary DAC was 208 in the pre-intervention period and 105 in the intervention period. The average monthly number of patients identified as receiving unnecessary DAC at screening was decreased by 49.5% from 34.7 in the pre-intervention period to 17.5 in the intervention period (Fig. 3). Wilcoxon rank sum test revealed there was a significant statistical difference in the monthly number of patients receiving unnecessary DAC at screening between the two periods (P = 0.016). The proportion of patients identified as receiving unnecessary DAC at screening among all patients receiving DAC also decreased by 37.5% from 54.7% in the pre-intervention period to 34.2% in the intervention period (P < 0.001) (Fig. 3).
2. Effect of prospective audit and feedback
The number of patients receiving unnecessary DAC for more than 3 days was 161 in the pre-intervention period and 42 in the intervention period. The proportion of patients receiving unnecessary DAC for more than 3 days among the patients identified as receiving unnecessary DAC at screening decreased by 48.3% from 77.4% in the pre-intervention period to 40.0% in the intervention period (P = 0.002) (Fig. 4). In other words, changes from day 1 to day 3 increased in the intervention period by 165.5%.
3. Overall effect of the intervention
After all, the average monthly number of patients receiving unnecessary DAC for more than 3 days decreased by 73.9% from 26.8 in the pre-intervention period to 7.0 in the intervention period (Fig. 4). Wilcoxon rank sum test revealed there was a significant statistical difference in the monthly number of patients receiving unnecessary DAC for more than 3 days between the two periods (P = 0.005). The proportion of patients receiving unnecessary DAC for more than 3 days among all patients receiving DAC decreased by 67.8% from 42.3% in the pre-intervention period to 13.6% in the intervention period (P < 0.001) (Fig. 4).
4. Compliance with consultation notes and time spent on screening and writing
For 33 out of the 105 patients identified as receiving unnecessary DAC in the intervention period, prescriptions were issued when the pharmacist was off duty. These patients were not subject to consultation notes. Among the remaining 72 patients, consultation notes were written for educational purposes for 23 patients who were not in the hospital at the time of screening.
Consultation notes were written for the purpose of intervention for 49 patients (68.1% of 72). In the assessment on day 3, only 3 out of 49 patients still received unnecessary DAC. Thus, the rate of compliance with the consultation notes was 93.9% (46/49).
The pharmacist recorded the daily time spent on screening and writing the consultation notes. The average daily time spent on works related with the intervention was 37.0 min (95% CI, 11.6-62.4).
Discussion
This study showed that an intervention targeting unnecessary DAC, which consisted of education via e-mail along with prospective audit and feedback, significantly reduced the number of patients receiving unnecessary DAC. To estimate the overall effect of the intervention, we compared the monthly number of patients receiving unnecessary DAC for more than 3 days after screening, before and after the intervention. The average monthly number of patients receiving unnecessary DAC for more than 3 days decreased by 73.9% after the intervention was initiated. The proportion of patients receiving unnecessary DAC for more than 3 days also decreased by 67.8% after initiation of the intervention.
Traditionally, education has been considered as one of the key elements of antimicrobial stewardship program (ASP), and various forms of intervention programs on the basis of education had been implemented. However, there were several conflicting results, and there have been concerns about the effectiveness of education as a method of stewardship intervention, especially when provided alone [8910].
Given that the prospective audit and feedback can be considered a kind of education, we could regard "education" as a core element of our intervention. However, education in our study was confined to the provision of information and local guideline via e-mail. Although there might be interactions between the 2 methods of the intervention during the overall intervention period, the monthly number of patients receiving unnecessary DAC decreased significantly just with education, before the audit and feedback component of the intervention was implemented. This suggests that unnecessary DAC prescription stems from insufficient information about the spectrum of antimicrobial activity and the routine repetition of incorrect practices. The high rate of compliance with the consultation notes (93%) also supports this assumption about the nature of unnecessary DAC prescription.
Although the intervention effects were the result of collaboration between a pharmacist and an infectious disease physician, the pharmacist was responsible for the key activity of writing consultation notes. This kind of multidisciplinary approach may enable the development of various types of stewardship programs and make their implementation more efficient, especially in settings with limited resources for ASP [11].
There was a large variation in the average time the pharmacist spent on intervention-related activities. This variation might be due to differences in weekday workloads. In other viewpoint, it is difficult to say that the amount of time spent was not large when considering the actual number of subjects for prospective audit and feedback during the intervention period. Therefore, efforts to enhance the efficiency of this program are needed.
The present results, however, should be interpreted with caution. We analyzed the data assuming independence of all antimicrobial prescriptions. This assumption may have confounded the results since we did not calculate correlations between prescriptions from the same prescribers or the same departments. Thus, although we have provided evidence of the beneficial effects of a stewardship intervention on unnecessary DAC prescription, further research that tests such correlations would provide a more sophisticated estimate of the intervention effects.
In conclusion, this study showed that a stewardship intervention including education along with prospective audit and feedback was effective in reducing unnecessary DAC prescription. Our results indicate that unnecessary DAC prescription can be an appropriate target for stewardship interventions and that a multidisciplinary approach involving collaboration with pharmacists could be promising for ASP.



 XML Download
XML Download