

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Human being have recently experienced a novel H1N1 influenza A virus that was genetically reassorted in swine [1]. After severe acute respiratory syndrome (SARS) and the avian influenza epidemic, many countries had prepared for the arrival of the next pandemic influenza [2, 3]. In 2009, pandemic influenza became a real situation. We observed a surge of patients with influenza-like illness (ILI) from the end of September 2009 in the Republic of Korea, 3 months after the declaration of a pandemic by the World Health Organization on June 11, 2009. The severity of the pandemic (H1N1) 2009 varied among countries, and the policies for pandemic (H1N1) 2009 were adjusted every month since the first recorded infection in Veracruz, Mexico.
At the time pandemic (H1N1) 2009 was being transmitted in other continents, emergency triages and isolation wards were prepared in our country. The Korea Centers for Disease Control and Prevention (KCDC) appointed epicenter hospitals among the general hospitals or tertiary hospitals in every city specifically for treating pandemic (H1N1) 2009 infected patients. In most schools, febrile students were sent home and recommended to visit a clinic to determine if they were infected with H1N1 influenza virus. Tremendous numbers of reverse transcriptase polymerase chain reaction (RT-PCR) were performed, and the neuraminidase inhibitor, oseltamivir or zanamivir were prescribed to the suspected patients in advance before the results of RT-PCR were confirmed. Newly developed vaccines against pandemic (H1N1) 2009 were first distributed to the medical staffs and school aged-children for preventing further spread [4, 5]. After starting the vaccination program against H1N1, a big surge of patients with H1N1 infection was rapidly suppressed in the end of November 2009 [4].
Many reports about fatal pneumonia due to influenza including pandemic (H1N1) 2009 have given us useful immunologic information for timely management [6-8]. Lymphopenia has been focused on as a major risk factor for many critical cases. This marker, lymphopenia, can be easily detected before the result of RT-PCR. Cui et al. directly showed that CD4+ T cells and CD8+ T cells were initially reduced in the fatal cases with pandemic (H1N1) 2009 [9]. Other studies on the relationship between lymphopenia and secondary bacterial infection in patients with influenza support the importance of lymphopenia in the rapid clinical progress of H1N1 [10, 11]. Therefore, lymphopenia could be the main link to understand the big gap between the relatively low to moderate virulence of H1N1 and the clinically fatal outcome of cases with H1N1 infection.
We report here how the severity of the admitted pediatric H1N1 patients was changed after the vaccination program. Additionally, we focused on lymphopenia which might explain the differences of the clinical courses between the pre- and the post-vaccination periods.
Materials and Methods
From August 20 2009 to February 20 2010, patient screening and real time RT-PCR (rRT-PCR) for pandemic (H1N1) 2009 infection were performed in Wonju Christian Hospital (WCH), which covers 300,000 people as one of the tertiary hospitals in the Republic of Korea. We reviewed the clinical characteristics of the patients with pandemic (H1N1) 2009 and analyzed the differences between two periods: August 20 - November 30 2009, which is the pre-vaccination period, and December 1 2009 - February 20 2010, which is the post-vaccination period. According to the KCDC guidelines, medical workers and school-aged children received H1N1 vaccination preferentially [12]. The clinical records were reviewed by one pediatrician and the radiologic findings were determined by one radiologist.
The approval of the institutional review board was exempted because this study was performed retrospectively by chart review and the private information of the patients was not revealed to the public.
1. Case definition
Any patients who had fever ≥37.8℃, as checked by a tympanic thermometer, and who had at least a symptom among cough, rhinorrhea, sore throat, myalgia or headache underwent rRT-PCR for diagnosing pandemic (H1N1) 2009 infection. If the result of rRT-PCR was positive, then the patient was confirmed as having an pandemic (H1N1) 2009 infection. The patients younger than 15 years of age with confirmed pandemic (H1N1) 2009 infection and who were admitted due to severe respiratory infection, febrile convulsion or dehydration were included in this study.
2. Diagnosis of pandemic (H1N1) 2009 infection
The method of sample collection was nasopharyngeal aspiration or nasopharyngeal swab. After collecting samples, rRT-PCR was performed within 4 hours in the laboratory of our hospital. The RNA was extracted with an ExiPrep viral RNA/DNA extraction kit (BIONEER Co., Daejeon, Korea). rRT-PCR was conducted using InfA Real-Time RT-PCR Kit (BIONEER Co.) and an Exicycler™ 96 (BIONEER Co.) [13].
3. Secondary bacterial pneumonia
The secondary bacterial pneumonia was defined as follows: 1) Radiologic findings that show confluent lobar consolidation and 2) the peripheral white blood cell count higher than 15,000/mm3 with a predominance of granulocytes or a serum C-reactive protein (CRP) level more than 8 mg/dL [14, 15].
The diagnosis of mycoplasma infection was based on serologic study. If M. pneumoniae-specific immunoglobulin M was detected in a patient, then the patient was regarded as being co-infected with this microorganism. Other laboratory workups for detecting bacteria that can cause pneumonia such as Chlamydophila pneumoniae or Legionella pneumophila were not performed because of their relatively low incidences in children.
4. Definition lymphopenia
The study group was divided into 2 groups as 1) the patients with lymphopenia (PL) and 2) those without lymphopenia (nonPL), according to the results of the complete blood count performed at admission. The definition of lymphopenia in this study was a lymphocyte count less than 10 percent of the total number of leukocytes, and the absence of lymphopenia was defined as a lymphocyte count more than 20 percent of the total number of leukocytes as in other study [16]. The patients in the overlapping zone (10~20% of total leukocytes) were excluded. The clinical differences between the PL and nonPL were analyzed.
5. Statistical analysis
The differences of clinical characteristics between the pre-vaccination period and the post-vaccination period and the differences of clinical severity between the PL and nonPL were analyzed by unpaired t-test with Welch's correction. The difference of the hypoxia incidence according to lymphopenia was analyzed by Fisher's Exact test. GraphPad Prism version 5.00 for Windows (GraphPad Software, San Diego, CA, USA) was used for the statistical analysis. P<0.05 was considered statistically significant.
Results
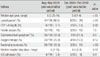
Of the 2,399 children who had been confirmed as having pandemic (H1N1) 2009 infections, 149 patients (6.2%) were admitted over the 6 month period. Through the end of November 2009, 2,177 children were confirmed as having pandemic (H1N1) 2009 infections and 119 patients (5.5%) were admitted. From December 1 2009 to February 20 2010, the number of patients with confirmed H1N1 infection decreased to 227. The number of admitted patients also decreased to 30 (13.2%). Table 1 showed the differences of the demographics, the laboratory findings and the hospital course of the admitted pediatric patients with H1N1 between the pre-vaccination period and the post-vaccination period.
1. Comparison of the clinical features between the pre- and post-vaccination period
The median age of the admitted patients was significantly different between the pre- and the post-vaccination period (P<0.05). During the first 3 months before starting vaccinations for pandemic H1N1, the median age was 6 years of age (range: 0.25-14), while during the later 3 months (post-vaccination period) it was 3 years of age (range: 0.1-14) (Table 1).
The percentage of patients with lymphopenia was significantly decreased during the post vaccination period (P<0.05). However, the number of patients with a CRP level ≥8 mg/dL, the number of patients with febrile seizure, the number of patients who had gastrointestinal symptoms including vomiting, diarrhea or abdominal pain, the number of patients who received oxygen therapy, the median hospital stay and the number of patients who were admitted to the intensive care unit (ICU) were not different between two periods (Table 1).
2. Clinical spectrum of pandemic (H1N1) 2009 at admission
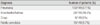
Pneumonia was diagnosed in 100 of 149 patients (67.1%) who were admitted to the hospital over the 6 month period; bronchiolitis or asthma was diagnosed in 28 (18.8%); acute pharyngitis with febrile convulsion was diagnosed in 18 (8.7%); and croup was diagnosed in 9 (6%). There was no case of acute respiratory distress syndrome or meningoencephalitis (Table 2). In terms of the underlying diseases, 11 patients had known asthma (7.3%), 7 patients had known cerebral palsy (4.7%), 2 patients had known nephrotic syndrome, 2 patients had known congenital heart diseases, 1 patient had Kawasaki disease, and 1 patient had brain tumor.
Although there was no case of culture-confirmed bacterial pneumonia, 39 cases among the 100 patients with pneumonia (39%) were suspected as having secondary bacterial pneumonia by authors own definition described in Materials and methods.
3. Critical cases due to pandemic (H1N1) 2009
Four of the 149 patients (2.7%) were admitted to the ICU, and there was no fatal case. All four patients in ICU had no underlying diseases and they had been previously healthy. Thirty four of the 149 patients (22.1%) received oxygen supplement and 3 patients among the 34 patients received ventilator care.
4. Radiologic findings
Various radiologic findings were observed in the admitted patients. The most frequent finding was increased interstitial marking in 62 cases of 149, followed by minimal change (50 cases), bilateral patchy infiltrates (39 cases), perihilar haziness (27 cases), focal segmental infiltrates (25 cases), atelectasis (14 cases), ground-glass opacity and air bronchogram (12 cases), pleural effusion (4 cases) and pneumomediastinum or pneumothorax (3 cases). Thirty nine cases out of the 100 patients with pneumonia (39%) showed bilateral patchy infiltraties or lobar infiltrates, which suggest secondary bacterial pneumonia.
5. Co-infection with mycoplasma
The incidence of co-infection with M. pneumoniae was 27 cases out of a total of 137 patients who took this test (19.7%). The median age of the pandemic (H1N1) 2009 patients who were co-infected with M. pneumoniae was 5 years of age (range: 1.3-8).
6. Lymphopenia and the clinical severity
A total of 52 patients were included in the PL and 57 patients were included in the nonPL. Age, the CRP level and the hospital stay were compared (Fig. 1). The median age of the PL was significantly older than that of the nonPL (7 years of age vs 2 years of age, P<0.0001) (Fig. 1A). The median serum level of CRP of the PL was higher than that of the nonPL (5±0.6 mg/dL vs. 1.9±0.4 mg/dL, P<0.0001) (Fig. 1B). Furthermore, the median hospital stay of the PL was longer than that of the nonPL (5.5±0.2 days vs. 4.5±0.2 days, P<0.01) (Fig. 1C).
Discussion
Our data showed that 35% of the total admitted patients younger than 15 years of age had lymphopenia on admission day. This rate is similar to the data reported by Chien et al. [18]. Cunha et al. also reported that lymphopenia is one of the unfavorable predictors when a rapid diagnostic test for influenza is negative and the confirmative test is delayed [10]. The report from the herald wave of the pandemic in Mexico showed a higher rate of lymphopenia (61%) [7] than our data.
In an animal model of influenza infection, increased pulmonary interferon (IFN)-γ was related with the suppression of phagocytosis and this led to enhanced susceptibility to secondary pneumococcal infection [11]. Furthermore, IFN-γ has pro-apoptotic activity by reducing the survival of T cells [19]. Taken together, when the host is infected by influenza virus, the phenomena of lymphopenia and secondary bacterial infection may be mediated by increased serum level of IFN-γ.
In addition, it has been reported that the higher expression of apoptotic factors due to antigenic stimuli is correlated with the age of the host [20]. The severe clinical manifestations in older children may be explained by the higher rate of lymphopenia due to the higher expression of various apoptotic factors than those of young infants. Interestingly, the median age of the PL group was significantly higher than that of the nonPL group (7 vs. 2 years of age) in this study. This result also supports the hypothesis about the relationship among apoptosis, age and the clinical severity.
The admission rate of infants was increased in the post-vaccination period, and the clinical severity of the admitted infant cases in the post-vaccination period seemed to be milder than those of the admitted infant cases in the pre-vaccination period. The most common cause of their admission was a decreased amount of oral feeding. The clinical severity as represented by the length of hospital stay, ICU admission and oxygen therapy, was decreased in the post-vaccination period, although there was no statistically significance. The rate of lymphopenia was also significantly decreased in the post-vaccination period compared with that of the pre-vaccination period. Therefore, we may speculate that the majority of admitted patients with pandemic (H1N1) 2009 were infants in the post-vaccine era because they had not yet received pandemic (H1N1) 2009 vaccination. The apoptotic capacity of unvaccinated infants by viral stimulation may have been lower than that of the older unvaccinated children in the pre-vaccine era.
Okada et al. reported that the apoptosis of lymphocytes by measles infection is age-dependent [21]. They also showed that the clinical severity of measles was correlated with age and the immunosuppression due to lymphopenia as a result of apoptosis was also correlated with age. Although our concern is the apoptosis of lymphocytes caused by H1N1 not by measles virus, the primary host immune response against new virus may show a similar pattern according to age. Therefore, our observation of the lower proportion of lymphopenia and the milder clinical outcomes in infants may be explained by this hypothesis.
The limitations of this study were as follows. First, vaccination against H1N1 was performed partially and it was started at the peak period of the pandemic. Therefore, we could not exactly estimate the vaccine effectiveness. Second, because this study was performed retrospectively, we could not directly measure the apoptotic factors that may affect the depletion of lymphocytes. Hence, we could suspect the relationship of lymphopenia and the clinical severity according to age only by clinical data.
In conclusion, the clinical manifestations of the pandemic (H1N1) 2009 seemed to be more severe during the pre-vaccination period than those during the post-vaccination period in pediatric patients. Our study showed that the higher proportion of lymphopenia may be related with the clinical severity in the pre-vaccination period.


 XML Download
XML Download