

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Papillary thyroid carcinoma (PTC) is the most common type of thyroid cancer, accounting for approximately 80% of all thyroid malignancies[1]. Recently, a number of histologic variants of PTC have been described[2~6]. The follicular variant is the most common subtype of PTC[7]. The clinical behavior of the follicular variant is generally regarded as being similar to that of classic PTC[7~9]. On the other hand, some variants have been identified as being more aggressive and show higher rates of morbidity and mortality than the classic PTC[3~5,10,11]. These aggressive types include the tall cell variant, columnar cell variant, diffuse sclerosing variant, solid variant and oncocytic variant[4,5]. Although several studies on the outcomes of such variants have been performed[2~5], the available data are limited due to the low prevalence of these tumors and the absence of long-term follow-up.
Therefore, in this study, we divided the PTC variants into two groups, favorable and aggressive, and studied the patient outcomes compared to those with classic PTC.
Materials and Methods
1. Patients
We included 2,366 patients with classic PTC and 159 patients with PTC variants. The medical records of 2,525 patients with PTC were retrospectively analyzed. All patients underwent thyroidectomy at Samsung Medical Center, Seoul, Korea between 1994 and 2004. The 2,243 patients (89%) underwent total thyroidectomy. Radioactive iodine was given to 2,182 of 2,525 patients (86%). All patients were given TSH suppression therapy. The median postoperative follow-up period was 66 months with a range from 0.2 to 166 months. The 159 patients with PTC variants included 119 patients with follicular variants including 14 encapsulated form, 13 diffuse sclerosing variants, 11 tall cell variants, six solid variants, six oncocytic variants, and four columnar cell variants (Table 1). An experienced pathologist reviewed the pathology findings prior to the study. Each variant was defined as typical nuclear features of PTC including ground glass nuclei, nuclear grooves, overlapping nuclei, and/or nuclear inclusions with the following criteria[12]. Follicular variants were diagnosed when there was exclusively or nearly exclusively a follicular growth pattern. Follicular variants were subdivided into encapsulated follicular variant if the tumor was surrounded totally by a tumor capsule. The diffuse sclerosing variants were diagnosed when there was diffuse involvement of one or both thyroid lobes with extensive squamous metaplasia, numerous psammoma bodies, dense lymphocytic infiltration and stromal fibrosis. The tumor size of diffuse sclerosing variants were determined by a dominant nodule. The tall cell variants were diagnosed when there were 50% or more tall cells with their height three times their width and intensely eosinophilic and finely granular cytoplasm. The solid variants were diagnosed when there was a predominantly (> 70%) solid growth pattern without tumor necrosis. The oncocytic variants were diagnosed when there was a papillary or follicular architecture with oncocytic, granular cytoplasm accounting for more than 70% of the tumor. The columnar cell variants were diagnosed when there were pseudostratified columnar cells with hyperchromatic nuclei accounting for more than 50% of the tumor. We divided the PTC variants into two groups, favorable and aggressive. The favorable variant included the follicular type, and the aggressive variants included the diffuse sclerosing, tall cell, solid, oncocytic, and columnar cell variants (Table 1).
Staging was performed using the TNM classification based on the American Joint Committee on Cancer (AJCC) staging (2002)[13]. We normally followed up the patients by ultrasonography with chest X-ray once or twice per year. And thyroglobulin levels were measured. We defined distant metastasis as histological confirmation of the tumor or as the presence of the typical features detected by radiological studies, radioactive iodine whole body scanning or positron emission tomography (PET). The survival period was calculated from the date of pathology confirmation to the date of disease-specific death. Deaths from causes other than thyroid carcinoma were treated as censored observations. We also calculated the recurrence-free survival rate. Recurrence was established on the basis of histological examination of recurrent tumor, typical features on radiological studies or radioactive iodine scanning, as well as unstimulated or stimulated thyroglobulin levels greater than 2 ng/mL that increase over time. Recurrences diagnosed within 4 months after the primary surgery were regarded as part of the primary tumor status and were referred to the time of diagnosis[3].
A total of 0.9% of patients with PTC died of thyroid carcinoma, and 1% developed recurrent disease during the observation period.
2. Statistical Analyses
Results are presented as the mean ± standard deviation, percents or medians as indicated. Age and tumor size were compared using the Mann-Whitney U test for independent samples, and two-by-two tables were analyzed using the Pearson's chi-square test or Fisher's exact test. Disease-specific and recurrent-free survival were evaluated by the Kaplan-Meier method and compared by the log rank test using the Bonferroni correction. P values less than 0.05 were considered statistically significant.
Results
1. Comparison of Clinicopathologic Features of Favorable PTC Variant Compared to Classic PTC (Table 2)
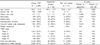
The mean age of the patients with favorable PTC variant was 46.4 years (range, 15~76) compared to 45.6 years (range, 9~81) in the patients with classic PTC. The proportion of male patients in the favorable variant was significantly higher than in the classic PTC group (29% vs. 13%, P < 0.001). The tumor size of the patients with favorable variant was significantly larger than the classic PTC patients (2.3 ± 2.0 cm vs. 1.5 ± 1.2 cm, P < 0.001). The patients with favorable variant had significantly less aggressive pathological findings compared to the classic PTC patients including the following: bilaterality (15% vs. 24%, P = 0.032), multifocality (22% vs. 32%, P = 0.021), extrathyroidal invasion (27% vs. 58%, P < 0.001), and cervical lymph node metastasis (18% vs. 39%, P < 0.001). In addition, the patients with favorable variant presented with less advanced disease (stage I & II, 83% vs. 64%; stage III & IV, 17% vs. 36%; P < 0.05). Among 119 patients with favorable variant, only one patient (0.8%) had distant metastasis to the lung at the time of diagnosis. By contrast, distant metastasis was found in 47 patients (2%) among the classic PTC patients. Among the patients with favorable variant, none of the 14 patients with an encapsulated follicular variant had bilaterality, multifocality, extrathyroidal invasion, cervical lymph node metastasis, distant metastasis, and stage III or IV disease.
2. Comparison of the Clinicopathologic Features of Aggressive PTC Variants Compared to Classic PTC (Table 3)
The mean age of the patients with aggressive PTC variants was 44.6 with a range from 20 to 74 years of age. The proportion of male patients among the aggressive variants was similar to the classic PTC patients (18% vs. 13%). The tumor size of the patients with aggressive variants was significantly larger than the classic PTC patients (3.2 ± 2.3 cm vs. 1.5 ± 1.2 cm, P < 0.001). There were no significant differences in multifocality, extrathyroidal invasion, distant metastasis, and disease stage. However, bilaterality (38% vs. 24%, P = 0.041) and cervical lymph node metastasis (58% vs. 39%, P = 0.015) were more frequently found in the patients with the aggressive variants compared to those with classic PTC. Among 40 patients with aggressive variants, tumors metastasized to the lung in one patient with the tall cell variant, and to the chest wall in one patient with the oncocytic variant. When we evaluated 11 patients with the tall cell variant and compared them to those with classic PTC, we found they presented at an older age (56 years vs. 46 years, P = 0.007), had larger tumors (3.9 ± 3.5 cm vs. 1.5 ± 1.2 cm, P = 0.043) and more frequently had bilateral tumors (55% vs. 24%, P = 0.027). There was no significant difference in the TNM stage between the two groups.
3. Survival Analysis (Fig. 1)
Eighteen patients (0.8%) with classic PTC, two (1.7%) with favorable variant and two (5%) with aggressive variants died during the follow-up period. The disease-specific survival rate of the patients with classic PTC was not significantly different from that of the patients with favorable variant (P = 0.336). However, it was significantly decreased among the patients with aggressive variants compared to the patients with classic PTC (P = 0.003). Among 40 patients with aggressive variants, two patients died of thyroid carcinoma with tall cell variant. When we evaluated 11 patients with the tall cell variant and compared them to patients with classic PTC, their disease-specific survival rate was significantly lower than the patients with classic PTC (P < 0.001).
4. Recurrence Analysis (Fig. 2)
Recurrence was detected in 18 patients (0.8%) with classic PTC, two (1.7%) with favorable variant, and six (15%) with aggressive variants. Among the recurred patients with favorable and aggressive variants, two patients had the follicular variant, two the diffuse sclerosing variant, two the solid variant, one the oncocytic variant, and one the tall cell variant. The recurrent sites were the thyroid beds or cervical lymph nodes in most patients; the lung was the site in one patient with the oncocytic variant. Recurrence-free survival rate was not different between the classic PTC and favorable variant patients (P = 0.213). The median recurrence-free survival time was significantly decreased in the patients with aggressive variants or the tall cell variant compared to the patients with classic PTC (P < 0.001).
Discussion
The results of this study showed that the prevalence of PTC variants was 6.8%. The prevalence of the favorable variant was approximately three times higher than that of the aggressive variants (4.7% vs. 1.6%). The follicular variant has been the most common histological subtype reported, accounting for about two-thirds of all PTC variants. However, its prevalence in this study was lower than previously reported (4.7% vs. 9~24%)[7,14,15]. Among the aggressive variants, the tall cell variant has been reported to be the most common subtype, accounting for 3~12% of all PTC[16,17]. In this study, the diffuse sclerosing variant was the most common subtype among the aggressive variants, with a prevalence of 0.5% among all subjects. The next most common subtype was the tall cell variant (Table 1).
The favorable variant had significantly less aggressive clinical and pathological features compared to the classic PTC patients including: less frequent bilaterality, multifocality, extrathyroidal invasion, cervical lymph node metastasis, and stage III & IV disease (P < 0.05). Disease-specific survival and recurrence-free survival rate were similar between the favorable variant and the classic PTC patients. Some investigators have reported that the behavior of the follicular variant was similar to classic PTC[7~9,18]; however, others have suggested that its behavior might be more aggressive than that of classic PTC[19,20]. The results of this study demonstrated that the clinical and pathological features and prognoses were similar between the two groups: less frequent extrathyroidal invasion (31% vs. 58%, P < 0.001), less frequent cervical lymph node metastasis (20% vs. 39%, P < 0.001) in the follicular variant group, and no differences in the disease-specific survival and recurrence-free survival rate between the two groups. However, the limitation of this study is the insufficient follow-up period. Further study with long-term follow-up is required.
Although follicular variant of PTC occurs more frequently in women than man, the male to female ratio has been reported to be similar between the follicular variant and the classic PTC[7,8,19], its ratio, in this study, was higher than in the classic PTC patients (P < 0.001). Such a difference may be due to some endemic factors, but the reasons to be elucidated. Liu et al.[21] reported that the encapsulated follicular variant did not develop nodal metastases or recurrences and could be treated by lobectomy alone. Our findings were consistent with this prior report; none of the encapsulated follicular variants had aggressive clinical or pathological features and none of the patients with these tumors died or had disease recurrence during follow up. On the other hand, Baloch and LiVolsi[22] reported five cases of encapsulated follicular variant that showed distant bone metastasis.
This study included 40 cases with aggressive variants, accounting for 1.6% of all PTC. Patients with the aggressive variants had significantly lower disease-specific survival (P = 0.003) and recurrence-free survival (P < 0.001) than did the patients with classic PTC. Interestingly, the clinical and pathological features including multifocality, extrathyroidal invasion and advanced stage disease did not differ between the two groups. However, bilaterality (38% vs. 24%, P = 0.041) and cervical lymph node metastasis (58% vs. 39%; P = 0.015) were more frequent in the aggressive variants than in the classic PTC. These findings suggest that bilaterality and cervical lymph node metastasis might be associated with a worse prognosis in the patients with aggressive PTC variants. Therefore, with such high rates of mortality and recurrence, it is important to identify these variants for appropriate management.
Among the aggressive variants, the tall cell variant is widely regarded as an aggressive form, which accounts for 3~17% of all PTC[16,17,23~28]. Patients with the tall cell variant are reported to present at an older age than classic PTC, with the mean age during the fifth to the sixth decade[17,24]. The prevalence of the tall cell variant was extremely low (0.4%) in this study, and the mean age of the patients at presentation was 56 years of age, an older age than in the patients with classic PTC (55.6 ± 16.3 vs. 45.6 ± 12.3, P = 0.007). Some studies have reported that the tumor size of the tall cell variant was greater than that of the classic PTC[4,24,26]. This larger size might be associated with its extrathyroidal invasion, and result in local recurrence and distant metastasis[3]. Most investigators have found a poorer prognosis associated with an older age at presentation, larger tumor size, and higher frequency of extrathyroidal invasion[29]. Our data also revealed an older age at the time of diagnosis (P = 0.007), larger tumor size (P = 0.043), and higher frequency of bilaterality (P = 0.027) in the aggressive variants compared to the classic PTC; however, there was no statistically significant increase in extrathyroidal invasion (82% vs. 58%). The aggressive variants did show a significantly lower disease-specific survival and recurrence-free survival (P < 0.001), consistent with the findings of previous studies[17,30,31].
We found that both the favorable and aggressive variants had a significantly larger tumor size than the classic PTC. Whereas the mean tumor diameter of the classic PTC was 1.5 cm, that of the favorable variant was 2.3 cm (P < 0.001) and that of the aggressive variants was 3.2 cm (P < 0.001). Furthermore, each of the subtypes showed similar results. The mean tumor diameter for the follicular variant was 2.4 cm (P < 0.001), diffuse sclerosing variant 3.2 cm (P = 0.003), tall cell variant 3.9 cm (P = 0.043), solid variant 2.8 cm (P = 0.006), and oncocytic variant 2.8 cm (P = 0.005). There have been debates about the tumor size of the follicular variant. Burningham et al.[32] suggested the follicular variants are larger tumors than the classic PTC. However, Carcangiu et al.[14] reported that it was smaller than the classic PTC. In addition, other investigators have reported that the tumor size of the follicular variant was similar to that of the classic PTC[12,16,17]. Moreover, there have been debates about the tumor size of the tall cell variant[30,33,34] and the diffuse sclerosing variant[35,36].
In this study, we defined the recurrence stringently. Recurrences diagnosed within 4 months after the primary surgery were regarded as part of the primary tumor status and were referred to the time of diagnosis[3]. Only 18 patients (0.8%) with classic PTC developed disease recurrence during follow-up.
Because the prevalence of PTC variants is very low, we could not analyze the prognostic factors related to survival or recurrence. Further studies with a larger number of cases are necessary to determine these parameters with greater certainty.
In summary, the tumor size of the favorable and the aggressive PTC variants were larger than that of the classic PTC. Although the favorable variant had less aggressive clinical and pathological features, their disease-specific survival and recurrence-free survival were similar to the classic PTC patients. The encapsulated follicular variant was associated with localized disease. By contrast, there was a tendency for the aggressive variants to have more aggressive clinical and pathological features, with significant bilaterality and cervical lymph node metastasis. They had significantly lower disease-specific survival and recurrence-free survival than the classic PTC patients. Among the aggressive variants, the tall cell variant presented with larger tumors at an older age and with more frequent bilateral tumors. Their disease-specific survival rate was significantly lower than the patients with classic PTC. These findings illustrate the importance of understanding the behavior of PTC variants for appropriate management. Further study is needed to elucidate the natural history of PTC variants especially those with aggressive behavior to improve patient outcome.



 XML Download
XML Download