

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Autoantibodies to thyroid-stimulating hormone (TSH, also called thyrotropin) receptor (thyrotropin receptor antibody [TRAb]) have two different main functions; stimulation or blocking of the TSH receptor (TSHR) [1234]. Graves disease (GD) is an autoimmune disorder that is mediated by the TRAbs that activate TSHR, thereby stimulating thyroid hormone synthesis, secretion, and thyroid cell growth [12]. The presence of circulating TRAbs is an important pathogenic indicator of GD [567]. Administering an antithyroid drug (ATD) is an effective therapeutic modality for the treatment of GD patients [18]. ATDs have beneficial immunosuppressive effects and reduce the production of thyroid hormones, as well as maintain the euthyroid state while patients wait for spontaneous remission [18].
The main drawback of ATD treatment for GD hyperthyroidism is the relapse rate after the withdrawal of ATDs, which is as high as 50% to 60% [69]. A useful predictive parameter for relapse would help to prevent long and complicated drug regimens that carry potentially serious adverse effects. The ability to predict the course and relapse of GD would also facilitate the selection of patients who require early definitive therapy including radioactive iodine ablation (RAI) or surgery. Many clinical factors have been suggested for predicting relapse, such as age, sex, presence of a goiter, family history of GD, thyroid hormone levels, thyroid echogenicity on ultrasonography (US), the results of Doppler US, and technetium-99m (99mTc) pertechnetate uptake [310111213]. TRAbs measurement is known to be useful for predicting GD relapse because of the active pathogenic role of TRAbs [3101415161718192021222324].
Assays for TRAb detection include the competitive thyrotropin-binding inhibitory immunoglobulin (TBII) assay and the thyroid stimulatory antibody (TSAb) bioassay [34]. The TBII assay can detect immunoglobulins that inhibit the binding of radio-labeled TSH to TSHRs [4252627]. This assay measures not only thyroid-stimulating immunoglobulins (TSIs), but also thyroid-blocking immunoglobulins (TBIs) and neutral immunoglobulins [42526]. However, the TSAb bioassay measures the production of cyclic adenosine monophosphate (cAMP) in response to interactions between TSHR and TSI. It can distinguish TSI from TBI and neutral TRAb [42526]. TSI in a patient's serum results in the increased production of cAMP, whereas TBI inhibits cAMP production [34].
The aim of this study was to compare the value of TSAb and TBII measurements at the time of ATD withdrawal for predicting relapse in GD patients. This study evaluated GD hyperthyroidism relapse during a median follow-up period of 21 months after ATD discontinuation.
METHODS
Patients
This retrospective study enrolled 74 GD patients who were treated between 2005 and 2012 at Asan Medical Center in Seoul, Korea. Patients with newly diagnosed GD who were treated with ATDs for the first time were enrolled. The diagnosis of GD was based on the following criteria: serum free thyroxine (fT4) level >24.45 pmol/L, decreased serum TSH level <0.3 mIU/L, increased serum TRAb levels (TSAb levels ≥ 140% or TBII titers ≥1.5 IU/L), increased uptake on 99mTc thyroid scan, and the presence of the appropriate clinical features such as a diffuse goiter, thyroid-associated orbitopathy (TAO), or symptoms of hyperthyroidism. A goiter was defined as the abnormal enlargement of the thyroid gland and diagnosed at the time of initial physical examination. The TAO diagnosis was based on the symptoms (dry eyes, diplopia, visual loss, visual field loss, and ocular pain) and signs (lid retraction, lid lag, glabellar furrows, proptosis). Patients who became pregnant during the follow-up period were excluded from this study. Those who required RAI therapy due to intractable GD or major side effects associated with ATDs were also excluded. This study was approved by institutional review board of Asan Medical Center, Seoul, Korea.
Patients were divided into the TSAb or TBII groups. Patients in the TSAb group received follow-up using the TSAb bioassay (n=35), and patients in the TBII group received follow-up using the TBII assay (n=39). ATD therapy and follow-up examinations were performed using a uniform protocol using a dose titrating regimen, mostly with methimazole (MMI) throughout the study period. Some patients were changed to receiving propylthiouracil (PTU) or carbimazole due to minor side effects associated with MMI. ATDs were discontinued when the serum fT4 and TSH levels of the patients were within the normal range for ≥6 months while receiving the minimum maintenance dose of ATDs (MMI ≤5 mg/day, carbimazole ≤10 mg/day, and PTU ≤100 mg/day), regardless of TRAb status. Median treatment duration with ATDs was 21 months (interquartile range [IQR], 10.0 to 27.5). All patients received follow-up using thyroid function tests (fT4, total triiodothyronine [T3], and TSH), and measurement of their TRAb levels (TSAb or TBII). These tests were performed at the time of ATD withdrawal and 3, 9, 15, and 21 months afterward.
Fifty-eight of 74 patients were treated with MMI, nine patients were treated with carbimazole, and seven patients were treated with PTU. Patients were considered to have relapsed if their fT4 levels were above the upper limit of the normal range (>24.45 pmol/L) and their serum TSH concentrations were low (<0.3 mIU/L).
Thyroid function tests
As previously described, the serum TSH concentrations (reference range, 0.3 to 4 mIU/L; lower detection limit, 0.01 mIU/L) were measured using an immunoradiometric assay (TSH-CTK-3; DiaSorin S.p.A., Saluggia, Italy) with a functional sensitivity of 0.07 mIU/L [28]. The serum fT4 level (normal range, 10.30 to 24.45 pmol/L) was measured using the fT4 radioimmunoassay (RIA) KIT (Immunotech, Prague, Czech Republic). The serum total T3 level (reference range, 1.51 to 2.77 nmol/L) was measured by RIA using T3-CTK (DiaSorin S.p.A.).
TSAb assays
For the TSAb assays, the Thyretai TSI reporter Bio Assay (Diagnostic Hybrids Inc., Athens, OH, USA) was used according to the manufacturer's instructions. The Thyretai kit is a Mc4 assay. The specimen-to-reference ratio (SRR), which is defined as the mean specimen TSI/mean reference TSI, is equal to 100. A specimen was considered positive if SRR was ≥140%.
TBII assays
For the TBII assays, the values were detected using the B. R.A.H.M.S. TRAK human RIA (B.R.A.H.M.S. GmbH, Hennigsdorf/Berlin, Germany) according to the manufacturer's recommendation. TBII titers ≥1.5 IU/L were considered positive. The analytical sensitivity was 0.3 IU/L and the functional assay sensitivity was 1.0±0.2 IU/L.
Statistical analysis
The statistical analysis was conducted using using SPSS version 21.0 (IBM Co., Armonk, NY, USA). Graphs were produced using Prism version 5.01 (GraphPad Software Inc., La Jolla, CA, USA). The continuous variables are presented as the mean±SD or medians with IQR. The continuous variables were compared between groups using the Student t test or Mann-Whitney test. The categorical variables are presented as numbers with percentages. The categorical variables were compared between groups using the chi-square test or Fisher exact test. The relapse-free survival (RFS) curves were calculated using the Kaplan-Meier method and the log-rank test was used to compare RFSs according to TRAb titers. The hazard ratio (HR) and 95% confidence interval (CI) used to evaluate the risk of relapse in the TSAb group were derived using Cox proportional hazards modeling. The multivariate analysis included age, sex, presence of a goiter and orbitopathy, thyroid function at baseline, treatment duration of any ATDs, and TSAb. All P values were 2-sided, with P<0.05 considered statistically significant.
RESULTS
Baseline characteristics
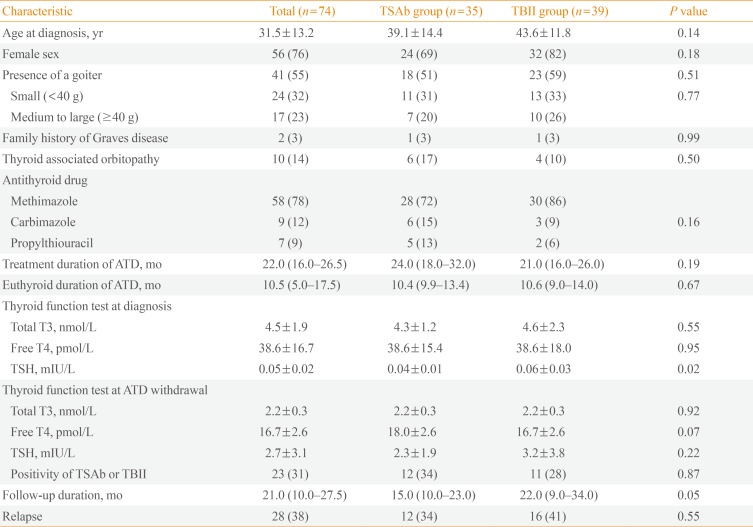
The baseline characteristics are listed in Table 1. The mean age of the 74 patients was 31.5±13.2 years, and 56 patients (76%) were female (Table 1). In the median follow-up period of 21.0 months (IQR, 10.0 to 27.5), 28 of 74 patients (38%) demonstrated GD relapse.
In the TSAb group (n=35), the mean age was 39.1±14.4 years, and 24 patients (69%) were female (Table 1). Eighteen patients (51%) had a goiter, and six patients (17%) had TAO at the diagnosis of GD. Twenty-eight patients (72%) were treated with MMI, and the median treatment duration using ATDs was 24.0 months (IQR, 18.0 to 32.0). The median duration of euthyroid status while using the minimum dose of ATDs was 10.4 months (IQR, 9.9 to 13.4). Twelve patients (34%) relapsed during the median follow-up period of 15.0 months (IQR, 10.0 to 23.0).
In the TBII group (n=39), the mean patient age was 43.6±11.8 years, and 32 patients (82%) were female (Table 1). Twenty-three patients (59%) had a goiter, and four patients (10%) had TAO at the diagnosis of GD. Thirty patients (86%) were treated with MMI, and the median treatment duration with ATDs was 21.0 months (IQR, 16.0 to 26.0). The median duration of euthyroid with the minimal maintenance dose of ATDs was 10.6 months (IQR, 9.0 to 14.0). Sixteen patients (41%) relapsed during a median follow-up period of 22.0 months (IQR, 9.0 to 34.0).
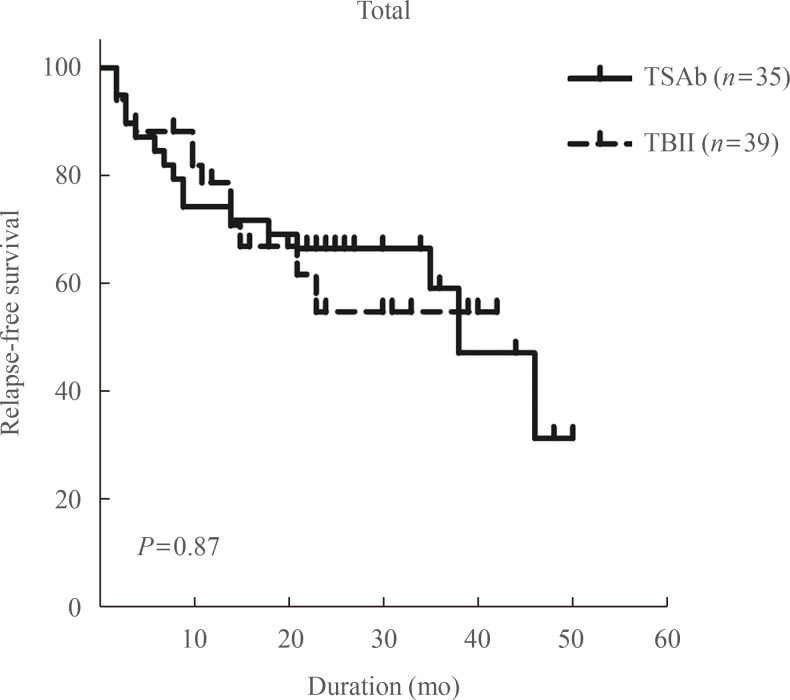
There were no significant differences in age, sex, presence of a goiter, 99mTc uptake on the thyroid scans, family history of GD, presence of TAO, treatment duration with ATDs, duration of euthyroid status while using a minimal maintenance dose of ATDs, thyroid function at diagnosis (except initial serum TSH levels), TRAbs positivity at withdrawal of ATD, or RFS between the TSAb and TBII groups (Table 1, Fig. 1).
Clinical characteristics of the patients in the TSAb group according to TSAb at ATD withdrawal
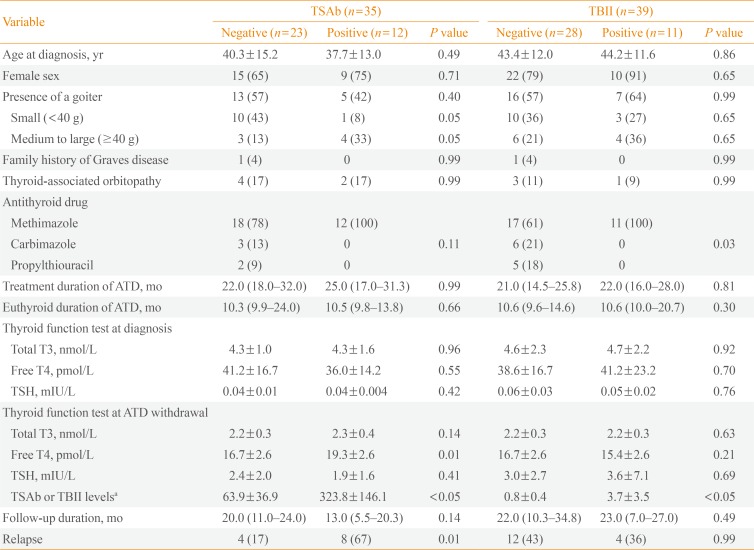
In the TSAb group (n=35), 23 patients (66%) were negative for TSAb and 12 patients were positive for TSAb at the time of ATD withdrawal. There were no significant differences in age, sex, presence of a goiter, 99mTc uptake on the thyroid scans, family history of GD, presence of TAO, treatment duration with ATDs, duration of the euthyroid status using the minimal maintenance dose of ATDs, and thyroid function at diagnosis between the TSAb-positive and -negative patients (Table 2). The fT4 level at ATD withdrawal was higher in TSAb-positive patients (19.31±2.57 pmol/L) than TSAb-negative patients (16.73±2.57 pmol/L, P=0.01). There were significantly more cases of relapse in TSAb-positive patients (8 of 12 patients, 67%) than TSAb-negative patients (4 of 23 patients, 17%) during the median follow-up period of 15.0 months (IQR, 10.0 to 23.0; odds ratio, 9.5; 95% CI, 1.9 to 47.7; P=0.007) (Table 2).
Clinical characteristics of the patients in the TBII group according to TBII at ATD withdrawal
In the TBII group (n=39), 28 patients (72%) were negative for TBII and 11 patients (28%) were positive for TBII at the time of ATD withdrawal. There were no significant differences in age, sex, presence of a goiter, 99mTc uptake on thyroid scans, family history of GD, presence of TAO, treatment duration with ATDs, duration of euthyroid status using the minimal maintenance dose of ATDs, and thyroid function at diagnosis between the TBII-positive and -negative patients (Table 2). There was no significant difference in the relapse rate between TBII-positive patients (4 of 11 patients, 36%) and -negative patients (12 of 28 patients, 43%) during the median follow-up of 22.0 months (IQR, 9.0 to 34.0) (Table 2).
RFS according to TSAb or TBII positivity at ATD withdrawal
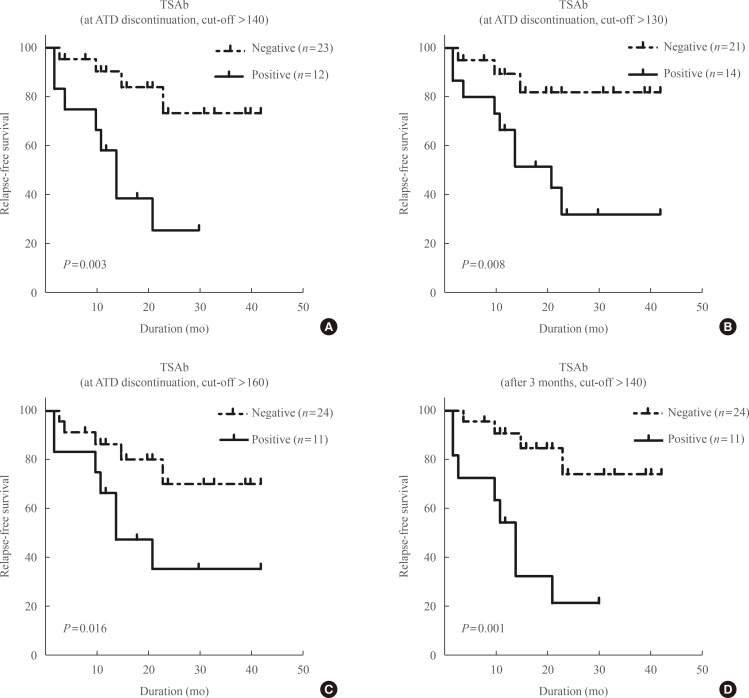
In the TSAb group, TSAb-positive patients demonstrated shorter RFS than TSAb-negative patients (P=0.003) (Fig. 2A). When we applied various cut-off values for TSAb positivity at ATD withdrawal, TSAb-positive patients still demonstrated significantly shorter RFS in comparison with TSAb-negative patients (Fig. 2B, C). When we compared TSAb levels at 3 months after ATD withdrawal, the RFS of TSAb-positive patients was also significantly shorter than TSAb-negative patients (Fig. 2D).
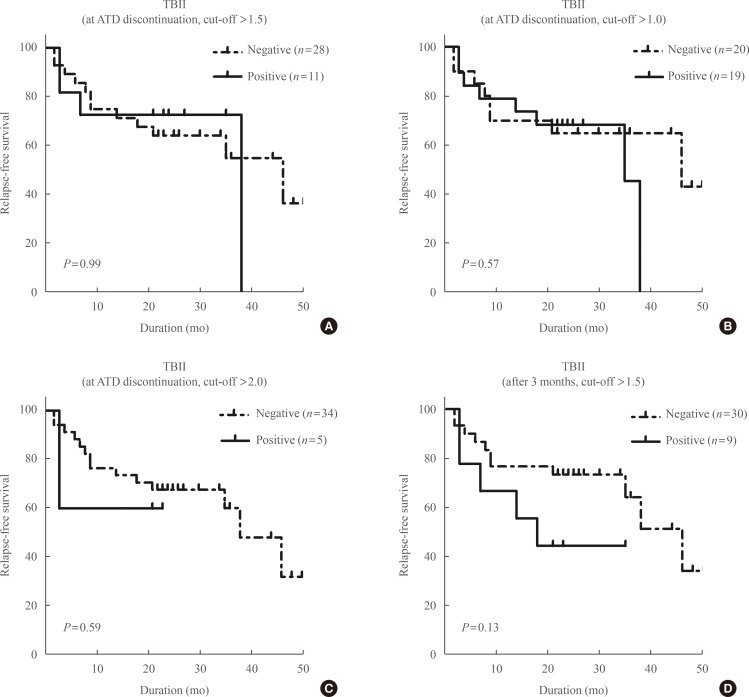
In the TBII group, there was no significant difference in RFS between TBII-positive and -negative patients at ATD withdrawal (using three different cut-off values) or at 3 months after withdrawal (Fig. 3).
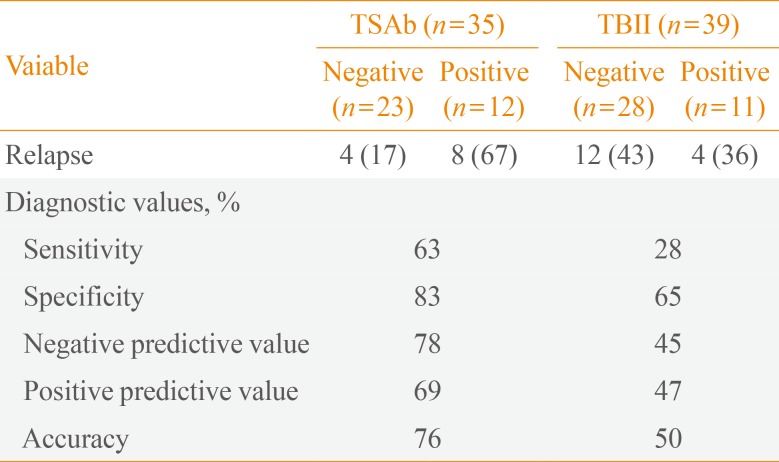
Diagnostic values of TSAb and TBII for predicting GD relapse
For predicting GD relapse, the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of a positive TSAb value at ATD withdrawal were 63%, 83%, 78%, 69%, and 76%, respectively (Table 3). For a positive TBI, these values were 28%, 65%, 45%, 47%, and 50%, respectively (Table 3).
Factors associated with GD relapse in the TSAb group
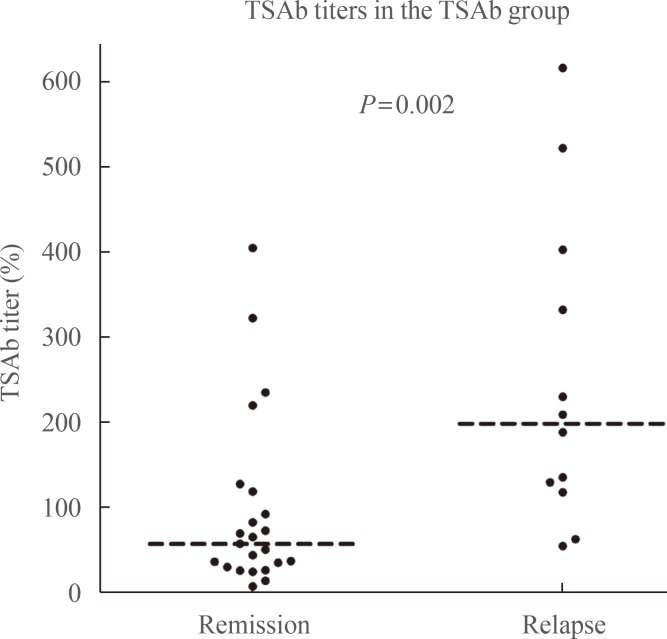
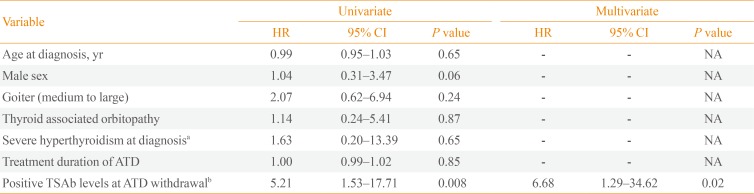
Patients who had higher TSAb titers at ATD discontinuation demonstrated more GD relapses (P=0.002). Patients with GD relapse demonstrated significantly higher TSAb titers at ATD discontinuation (P=0.002) (Fig. 4). The univariate and multivariate analyses were performed to determine the factors associated with relapse in the TSAb group. The TSAb level at ATD withdrawal was the only significant factor associated with relapse on the univariate analysis (HR, 5.21; 95% CI, 1.53 to 17.71; P=0.008) (Table 4). On the multivariate analysis, the TSAb level was a significant factor associated with relapse (HR, 6.68; 95% CI, 1.29 to 34.62; P=0.02) (Table 4).
DISCUSSION
In our current study, TSAb-positive patients demonstrated a higher risk for GD relapse after ATD withdrawal. The TSAb bioassay at ATD withdrawal was more useful for predicting the relapse of GD hyperthyroidism in comparison with the TBII assay. This study is the first study demonstrating RFS of the GD patients in the TSAb (Mc4 assay) and TBII (second-generation assay) groups. This study enrolled patients with newly diagnosed GD who were initially treated by dose titrating regimens of ATDs, and they maintained an euthyroid state with a minimum dose of ATDs for ≥6 months. All patients were followed using the same protocol after ATD withdrawal. We found statistically significant differences between the TSAb and the TBII assay for predicting the GD hyperthyroidism relapse. The cut-off values for TSAb and TBII at ATD withdrawal were the same as those used for diagnosing of GD.
Measuring TRAbs at the time of ATD withdrawal is useful for predicting GD relapse [3101415161718192021222324]. GD is characterized by remission and relapse, like many autoimmune diseases. In a meta-analysis conducted 20 years ago, TRAb assays could not demonstrate a sufficient predictive value for GD relapse, mainly due to the low sensitivity and specificity values of earlier assays [6]. However, a recent study reported a significant correlation between serum TRAb levels at the end of MMI treatment and percentage of patients with recurrent hyperthyroidism (r=0.56, P<0.001) and time to recurrent hyperthyroidism (r=–0.38, P=0.03) [29].
The TBII assay can detect immunoglobulins that inhibit the binding of radio-labeled TSH to TSHRs [25262730]. TBII as says that initially used porcine TSHR were shown to have a sensitivity of 50% to 90% [27]. Second-generation assays, such as solid-phase enzyme-linked immunosorbent assays and radio receptor assay, demonstrated much higher sensitivities (90% to 99%) and specificities (95% to 100%) [27].
The TSAb biologic assays measure the production of cAMP when sera-containing TRAbs are exposed to TSHR on cell preparations [3]. The Mc4 assay, as a third-generation TSAb assay uses genetically engineered Chinese hamster ovary (CHO) Mc4 cells [2526]. Because the substituted C-terminal area of TSHR includes epitopes for TBI, CHO Mc4 cells are capable of specifically detecting serum TSI without interfering with TBI [2526]. A specimen was considered positive if SRR was ≥140%. Using a cut-off SRR of 140%, receiver operating characteristic analysis demonstrated a sensitivity of 93% and a specificity of 100% in 103 untreated GD patients and 80% and 93%, respectively, in 155 treated GD patients in two independent studies [3132].
It remains controversial as to which assay is more useful for predicting GD relapse. Several studies have evaluated the value of the TBII assay for predicting GD relapse [161718202129]. One prospective study showed that the median TRAb levels according to three different TBII assays performed at the time of ATD withdrawal were significantly higher in the relapse group than in the remission group (P<0.05 for each assay) [20]. However, another study showed no significant difference in RFS between patients with positive- and negative-TBII levels at 4 weeks after the withdrawal of ATDs [18].
In our present study, the TSAb bioassay was found to be more useful for predicting GD relapse than the TBII assay. This study demonstrated better RFS of the GD patients in the TSAb (Mc4 assay) than TBII (second-generation assay) groups. Recently, several studies reported the usefulness of the TSAb bioassay for predicting relapse in GD patients. A prospective study with over 5 years of follow-up examinations reported that TSAb measurement using the Mc4 assay (Thyretain) can predict hyperthyroidism relapse after ATD withdrawal [22]. The Mc4 assay demonstrated a trend toward improved NPV (82.6% vs. 76.9%) and sensitivity (80.0% vs. 70.0%) in comparison with the M22 assay [22]. One retrospective study reported no significant differences in terms of sensitivity, specificity, PPV, and NPV between the M22 assay and the Mc4-TSAb assay for predicting GD relapse [14]. Using a high Mc4-TSAb cut-off value (230%), a better specificity (85%), and PPV (69%) were shown in comparison with the best cut-off value for the M22 assay [14]. These findings suggest that the TSAb bioassay is useful for predicting the relapse of GD hyperthyroidism. In our current analyses, patients with positive TSAb demonstrated shorter RFS values than patients with negative TSAb (P= 0.003) (Fig. 2). In contrast, there was no significant difference in RFS between patients with positive and negative TBII titers (P=0.99) (Fig. 3). When we applied various cut-off values for TSAb levels, RFS was still significantly shorter in TSAb-positive patients than TSAb-negative patients (Fig. 2).
In addition to the TRAb measurements, many factors such as age, sex, presence of a goiter, family history of GD, thyroid hormone levels, thyroid echogenicity, the results of Doppler US, and 99mTc uptake on thyroid scans are known to predict relapse [310111213]. However, according to our multivariate analysis, TSAb positivity was the only significant factor associated with relapse (Table 4).
This study has several limitations associated with its retro-spective design. First, we enrolled a relatively small number of patients, although these subjects achieved an euthyroid state for ≥6 months with the minimum maintenance dose of ATDs, and all patients were followed using a uniform protocol. Therefore, we were able to compare the relapse rate and RFS during the follow-up period. Second, we did not evaluate the TSAb and TBII levels in the same patients for direct comparison. However, there was no significant difference in the baseline characteristics or RFS between the TSAb and TBII groups. Third, this study was performed in an iodine-sufficient geographical area, and the results cannot be generalized to other populations [33]. Finally, a second-generation TBII assay was used instead of a third-generation M22-based assay. Comparing the M22-based TRAb assay with the second-generation assay, however, they had similar sensitivities and specificities, but the M22-based assay demonstrated significantly lower precision in some ways including a higher intra-assay coefficient of variation [273435].
In conclusion, TSAb assessment at the time of ATD withdrawal could be useful for predicting relapse in ATD-treated GD patients. However, TBII at ATD withdrawal cannot predict GD hyperthyroidism relapse. Measuring TSAb before ATD withdrawal could assist with clinical decision-making for GD patients.
 XML Download
XML Download