

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thyroid disease is one of the most common endocrine disorders in Korea, with the incidence of thyroid cancer increasing rapidly [1]. According to the Korea Central Cancer Registry 2010 annual report, the incidence of thyroid cancer accounted for 17.8% of all cancers (30.1% for women and 6.0% for men), with an annual growth rate as high as 25.5% for men and 24.5% for women, making it the fastest growing cancer type in Korea [2]. Such a spike in thyroid cancer cases, while not as spectacular as in Korea, is seen throughout the world, including in the United States (5th fastest rate of growth among cancers in women) and Japan (10th fastest in women) [3].
In addition to thyroid cancer, other thyroid diseases include hyperthyroidism, thyroiditis, and benign thyroid nodules. In the United States, the incidences of hyperthyroidism and thyroiditis were 1.3% and 4.6%, respectively [4]. In contrast, the comparable figure in a local community in Korea for individuals older than 40 years of age with subclinical hyperthyroidism was 11.7% (6.3% for men and 16.1% for women). The incidence rate increased as the average age increased, with the incidence of subclinical hyperthyroidism for those between 65 and 70 years reaching 10.8% for men and 18.9% for women [5].
The incidence rate of thyroid disease may have grown explosively in the 2000s in Korea due to the fact that high-resolution thyroid ultrasonography became widely available at that time, with a concurrent heightening of awareness of thyroid cancer among the general public, in addition to the natural increase in diagnosis of thyroid nodules including thyroid cancer [3]. Thyroid cancer, unlike many other cancers, shows a relatively excellent prognosis. Contrary to public perceptions; however, all patients diagnosed with thyroid cancer must undergo surgery to remove the thyroid tissue and long-term regular follow-up is needed to detect the cancer recurrence for the remainder of their lives [6]. In addition, patients may experience physical and psychological inconveniences such as depression and negative emotions due to thyroid dysfunction [7,8]. These caveats are equally applicable to other thyroid diseases, with wide variation among patients in terms of psychological and physical symptoms depending on thyroid hormone levels [9]. Once diagnosed with any of the thyroid diseases, patient will experience a host of symptoms that diminish quality of life. In addition, the treatment of thyroid dysfunction incurs high medical costs for the patient and family, as well as preventing the patient from engaging in gainful activities.
The fact that premature deaths from thyroid diseases reduce future income means, that the increase in such diseases is not just an issue limited to patients' families, but an economic issue that affects all of society. Nonetheless, studies of the social costs of disease have thus far been limited to the areas of respiratory disease, liver disorders, and digestive illnesses [10,11,12]. In the area of endocrine disorders, a previous study examined endocrine, nutrition, and metabolic disease as a whole [13], with no specific exploration of thyroid conditions.
Despite the important role of the thyroid gland in coordinating different organs through hormone secretion [14], and the fact that thyroid disorders are relatively easy to diagnose, these diseases have been ignored in social cost-of-disease studies and disease management policy priorities. In this study, we focus on data regarding the social costs of thyroid diseases in Korea for five biennial data points collected since 2002. These will serve as basic data to illustrate the importance of thyroid disease prevention and management for healthcare policy makers.
METHODS
Subjects and data
Items used in social cost-of-disease studies to represent cost include direct, indirect, and intangible costs. The viewpoints of these studies may represent the government, patient, or program-supplying organization, as well as society at large. The items of cost may differ widely depending on what point of view is chosen, which in turn affects the final outcomes of the study. In most such studies, the social cost of illness is measured from the viewpoint of society at large to track costs in the broadest possible way [15].
In this study, we classified social costs into direct and indirect costs and estimated the cost of disease due to thyroid conditions based on biennial data points collected over 5 years in Korea (2002, 2004, 2006, 2008, and 2010). We used the definition of thyroid disease delineated by the Korean Standard Classification of Diseases (KCD), which includes malignant and benign thyroid tumors, functional abnormalities and inflammation, and thyroid abnormalities in newborns. Detailed codes for diseases under examination include C73 and D093 for malignant tumors, D34 and D440 for benign tumors, E01 to E890, O905, R946, and H062 for functional abnormalities and inflammation, and P720 to P722 for thyroid abnormalities in newborns, all based on KCD-6 standards.
Direct costs were divided into direct medical and direct nonmedical costs. The first category includes patient expenditures associated with making outpatient visits to the hospital, inpatient costs, and expenses for drugs. Direct nonmedical costs are incidental expenses such as transportation costs and expenses for care during treatment.
The total treatment cost, including hospital bills and pharmacy prescription drug costs, can be estimated for patients with thyroid diseases in Korea by compiling data from the National Health Insurance Service. For this study, we estimated medical treatment costs related to thyroid gland diseases by combining the treatment amounts of inpatient, outpatient, and pharmacy costs by gender, age, and year, as described in the National Health Insurance Statistical Yearbook.
It was impossible to determine the figures for the items not covered by the health insurance scheme based on official statistical data. Given the health care insurance coverage ratio of 62.7%, the legally designated deductible ratio of 21.3%, and the noncoverage deductible ratio of 16.0% [16], the direct costs may have been underestimated because we did not count items not covered by the national health insurance scheme, including hospitalization, outpatient, and pharmacy costs. These values were estimated by imputing the deductible ratio to the total annual treatment cost by gender, age, and year. For example, the ratio of the deductible in the total treatment cost in 2010 was 25.79% for hospitalization (40.25% in 2004, 27.71% in 2006, and 30.38% in 2008), 25.79% for outpatient (20.63% in 2004, 17.37% in 2006, and 21.07% in 2008), and 2.99% for pharmacy (2.04% in 2004, 1.42% in 2006, and 2.04% in 2008). There were no data for the deductible ratio in 2002, which necessitated the use of 2004 data.
Direct nonmedical costs are incurred when the patient makes inpatient or outpatient visits to the hospital. In this study, these costs included transportation expenses and cost for care during treatment. To estimate nonmedical costs more precisely, it is necessary to have data on the number of hospitalization days for thyroid patients and the number of outpatient visit days. Since all Korean citizens are covered by the national health insurance scheme, all of this information can be obtained by examining data provided by the National Health Insurance Service.
The transportation cost was calculated by multiplying the average round-trip transportation cost needed to make one outpatient visit per thyroid patient (by gender and age) by the number of outpatient visits. In this case, the number of outpatient visits was based on data from the National Health Insurance Statistical Yearbook [17] and the average round-trip transportation cost was based on average round-trip transportation cost data from the 2008 Report of Korea Health Panel Survey [18]. The transportation costs per patient (1,475 won) were then calculated for each year by multiplying the consumer price index deflator [19] to produce costs for each year (993 won in 2002, 1,185 won in 2004, 1,332 won in 2006, 1,504 won in 2008, and 1,510 won in 2010).
The cost of hiring a professional caregiver to treat a thyroid patient was used to calculate care expenses. If the care was given by a family member, it was treated as an opportunity cost for the family caregiver. The number of hospitalization days due to thyroid conditions was extracted from the National Health Insurance Statistical Yearbook [16], with cost care based on the daily average caregiver cost (60,000 won) suggested by the Korea Caregivers Association applicable to both professional and family caregivers multiplied by the number of hospitalization days.
Future income loss from premature death due to thyroid diseases and productivity loss arising from absence for the treatment of the condition are included in indirect costs. The future income loss from premature death is calculated by multiplying the number of deaths (by gender and age) by per-capita loss from the following year of death to the year of life expectancy (by gender and age).
The number of deaths due to thyroid diseases was based on data from the Annual Report on the Cause of Death Statistics [20], which is published annually by the National Statistical Office, and per capita loss estimated by taking into account survival and employment rates, annual average wage level, and wage growth rates from the year following death to the expected end of life (Appendix 1).
The estimation of future income losses due to premature death was therefore based on the number of deaths by gender and age in the Annual Report on the Cause of Death Statistics [20], life expectancy and survival ratio figures in the Life Tables for Korea [21], employment ratio by gender and age in the Annual Report on the Economically Active Population Survey [22], annual average nominal wages in the Survey Report on Labor Conditions by Employment Type [23], and nominal wage growth rate figures in Current Economic Trends [24].
We included discount rates in the estimation equation to calculate the present value of future loss from premature death. This reflects an interest rate that is applicable when a subject gives up current consumption in favor of future consumption, which represents a time preference. In this study, we calculated future costs by dividing current costs by the discount rate of 5%.
Finally, productivity loss when the patient is absent from work due to visiting the hospital for thyroid treatment was estimated by multiplying the number of hospitalization days and outpatient visits (by gender, age, and year) by the daily average wage (by gender, age, and year) from the Survey Report on Labor Conditions by Employment Type [23], in the same way as the estimation of direct nomedical costs.
Estimation
Direct cost (DC) consists of direct medical costs (hospitalization, outpatient visit, and pharmacy costs) and indirect medical cost (transportation and caregiver costs). As seen in the estimation equation below, direct cost can be represented by multiplying the total medical cost of insurance-covered hospitalization, outpatient visit, and pharmacy cost by gender, age, and disease with the noncoverage ratios for each item (α, β, γ). Transportation costs subsumed in direct nonmedical costs were estimated by multiplying the number of outpatient visits for gender, age, and disease by the average transportation cost per visit. Caregiver cost was estimated by multiplying the number of hospitalization days by gender, age, and disease by the average daily caregiver cost.
DC=direct cost
i=1, 2,..., n disease, j=gender, k=0, 1,..., n age
IPijk=insurance-covered total hospitalization cost; i disease, j gender, k age
OPijk=insurance-covered total outpatient visit cost; i disease, j gender, k age
Pijk=insurance-covered total pharmacy drug cost i disease, j gender, age
α=ratio of noncoverage deductible in total hospitalization cost
β=ratio of noncoverage deductible in total outpatient visit cost
γ=ratio of noncoverage deductible in total pharmacy drug cost
OVijk=number of outpatient visits; i disease, j gender, k age
MTj=average round-trip transportation cost; j gender
IVijk=number of hospitalization days; i disease, j gender, k age
MC=daily average caregiver cost
Indirect costs consist of loss of future income due to premature death and productivity loss as a result of absence from work. We adopted gross loss of output or human capital approach to estimate loss of future income [25]. This is the most widely used methodology for estimating future income loss from premature death. As noted below, the estimation equation for future income loss is calculated by multiplying the per-capita human loss by gender and age (Appendix 1), as referred to the survival rate by gender and age, employment rate, annual average wage, wage growth rate, and discount rate, by the number of deaths from thyroid diseases.

HCC=future income loss from premature death
i=1, 2,..., n disease, j=gender, k= 0, 1,..., n age, τ=number of years
Dijk = number of deaths; i disease, j gender, k age
S =age; j gender, k age person's survival ratio at the time of k+τ
=age; j gender, k age person's survival ratio at the time of k+τ
=age; j gender, k age person's survival ratio at the time of k+τE=employment rate; j gender, k age person's employment rate at the time of k+τ
=employment rate; j gender, k age person's employment rate at the time of k+τYW=annual average wage; j gender, k age person's annual average wage at the time of k+τ
=annual average wage; j gender, k age person's annual average wage at the time of k+τWRk+τ=wage growth rate at the time of k+τ, r=discount rate
Productivity loss arising from the patient's absence from work while visiting the hospital is calculated by adding a third of the hospitalization days by gender, age, and disease and outpatient visits and multiplying the sum by the employment rate by gender and age and daily average wage. To adjust for productivity loss differences between outpatient visits and hospitalization, the productivity ratio used in Noh et al. [26] (1997) and Jung and Ko [27] (2003) was applied.
PLC=Σ [(IVijk +1/3OVijk)×Ejk×DWjk]
PLC =productivity loss from absence from work
i=1, 2,..., n disease, j= 1, 2 gender, k= 0, 1,..., n age
IVijk=hospitalization days; i disease, j gender, k age
OVijk=outpatient visits; i disease, j gender, k age
Ejk=employment rate; j gender, k age
DWjk=daily average wage; j gender, k age
RESULTS
Direct costs
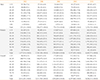
The direct medical costs, which included hospitalization, outpatient visits, and pharmacy prescriptions regardless of whether costs were covered by the national health insurance scheme was 531.4 billion won in 2010, a four-fold increase from 131.7 billion won in 2002. By gender, the figure for men increased to 95.5 billion won from 23.6 billion won for the same period, while that for women grew more than four-fold to 435.8 billion won from 108.1 billion won. As of 2010, the gender ratio was 18:82 between men and women, showing a prevalence of female patients by 4.6 to 1. By age group, patients in their 50s comprised the largest share (27.6%), followed by those in their 40s (24.5%), 30s (16.5%), 70s (6.9%), 20s (5.6%), and 60s (5.6%) (Table 1).
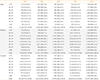
Transportation costs involved in outpatient treatment for thyroid conditions were 8 billion won in 2010, up from 2 billion won in 2002. By gender, the amount for men rose 4.1 times to 1.4 billion won from 300 million won during the same time period, while that for women increased 4.0 times to 6.6 billion won from 1.7 billion won. The gender ratio as of 2010 was 17.2:82.8, with a prevalence of female patients by 4.8 to 1. By age, patients in their 50s spent the most (26.6%), followed by those in their 40s (24.2%), 30s (17.9%), 60s (14.8%), and 20s (6.7%) (Table 2).
Caregiver costs may be incurred by hospitalized patients when they hire professional caregivers or rely on family members in whose case opportunity costs must be imputed. The caregiver cost has increased 3.2 times to 33.0 billion won in 2010 from 10.2 billion won in 2002. For men, the cost rose 2.7 times to 6.1 billion won from 2.2 billion won for the same period. For women, it increased 3.4 times to 26.9 billion won from 8.0 billion won. The gender share of caregiver costs between men and women in 2010 was 18.5:81.5, or 4.4 times higher for women than men. By age group, patients in their 50s comprise the largest portion (27.3%), followed by those in their 40s (25.1%), 30s (14.5%), 60s (14.0%), and 70s (9.1%) (Table 3).
Indirect costs
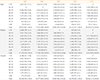
Indirect costs include loss of future income due to premature death and productivity loss as a result of the patient's absence from work. The estimated loss for the former in 2010 was 38.4 billion won, down 9.1 percent from 42.2 billion won in 2002. By gender, the loss for men rose 17.7 percent during the same period to 29.4 billion won from 25.0 billion won, while for women it declined 48% to 8.9 billion won from 17.2 billion won. The gender ratio for future income loss between men and women in 2010 was 76.7 to 23.3, 3.3 times higher for men. By age, patients in their 50s comprised the highest share (27.2%), followed by those in their 30s (26.0%), 40s (22.7%), 20s (9.2%), and 60s (8.3%), indicating that the social cost of premature death from thyroid disease is significant (Table 4).
The amount of productivity loss due to absence from work for thyroid treatment was 151.5 billion won in 2010, an almost four-fold increase from 38.1 billion won in 2002. By gender, the loss for men increased to 38.9 billion won from 9.8 billion won during the same period. For women, it was the same, a four-fold increase to 112.6 billion won from 28.3 billion won.
The loss ratio between men and women in 2010 was 25.7 to 74.3, with losses for women 2.9 times higher than for men. By age group, patients in their 40s comprised the highest portion (28.9%), followed by those in their 50s (27.9%), 30s (21.8%), 60s (11.5%), and 20s (5.6%) (Table 5).
Overall comments
The overall cost of thyroid diseases in Korea according to biennial data collected from 2002 to 2010 was 224.2 billion won in 2002, 303.4 billion won in 2004, 400.3 billion won in 2006, 570.4 billion won in 2008, and 762.2 billion won in 2010. Broken down into detailed items, direct costs in 2010 accounted for as much as 69.7%, followed by productivity loss resulting from the absence from work (19.9%), future income loss from premature death (5.0%), caregivers' cost (4.3%), and transportation cost (1.1%).
All cost items excluding future income loss from premature death showed rapidly increasing trends from 2002 to 2010. The share of future income loss due to premature death contributing to total cost declined, while that for direct costs exhibited an upward trend, signaling that policy measures to address medical expenditures related to thyroid conditions in Korea are urgently needed (Table 6).
A cost-of-illness analysis of thyroid diseases according to gender and age indicates that as much as 77.5% of total costs were incurred for the treatment of women as of 2010. By age, patients in their 50s comprised the largest portion with 27.6%, followed by those in their 40s (25.3%) and 30s (18.0%). These results indicate that thyroid diseases occur in age groups that are economically active, which leads to high current and future social costs.
DISCUSSION
The thyroid gland plays an important role in the body by coordinating different organs through hormone secretion. Since the introduction of high-resolution thyroid ultrasonography in the early 2000s, combined with the natural increase in thyroid nodules including thyroid cancer, the number of patients diagnosed with thyroid diseases in Korea has increased explosively. Nonetheless, there is a widespread public perception that thyroid cancer is a type of cancer that is relatively easy to treat.
In this study, we estimated social costs-of-illness for different types of thyroid disease including malignant and benign thyroid tumors, functional disorders and inflammation, and thyroid abnormalities in newborns, based on biennial data points collected for 5 years in Korea (2002, 2004, 2006, 2008, and 2010). Our findings serve as basic data and underscore the importance of thyroid disease prevention and management for healthcare policy makers.
The cost items included in this study are divided into direct and indirect costs. Direct costs include hospitalization, outpatient visits, and pharmacy prescription costs (all of which are direct medical costs), as well as transportation costs for outpatient visits and caregivers' cost (indirect medical costs). Indirect costs included future income loss from premature death and productivity loss as a result of absence from work due to hospital treatment.
It was found that the overall cost from thyroid diseases collected from biennial data from 2002 to 2010 was 224.2 billion won in 2002, 303.4 billion won in 2004, 400.3 billion won in 2006, 570.4 billion won in 2008, and 762.2 billion won in 2010. Over the eight-year period from 2002 to 2010, the cost volume associated with thyroid disease in Korea increased 3.4 times. Although their studies were not limited to thyroid diseases, Jung [13] and Jung and Ko [28] found that the social costs of endocrine, nutritional, and metabolic diseases exceeded 2.1 trillion won in 2007, a 1.7-fold increase from more than 1.2 trillion won in 2003. Our findings therefore indicate that the cost growth rate of thyroid conditions was twice that for endocrine, nutritional and metabolic diseases over the same time period. Even the costs of endocrine, nutritional, and metabolic cancers increased 70% for the same period, demonstrating a significant spike in costs associated with thyroid conditions.
The breakdown of thyroid diseases-related cost as of 2010 reveals that direct costs accounted for the lion's share (69.7%), followed by productivity loss (19.9%), future income loss from premature death (5.0%), caregiver cost (4.3%), and transportation cost (1.1%). These figures are consistent with the results of a previous study of the social costs due to endocrine, nutritional, and metabolic diseases [13] that showed the share of direct costs at 38.1%. Individual categories were also similar, such as productivity loss (20.2%), caregivers' cost (3.6%), and transportation cost (1.7%), but the rate of future income loss for thyroid-related disease was markedly less (5.0%) than that for endocrine, nutritional and metabolic diseases (36.4%).
By gender and age as of 2010, as much as 77.5% of the cost was incurred by women, with those in their 50s accounting for 27.6%, followed by those in their 40s (25.3%) and 30s (18.0%). Comparing these patterns to those for endocrine, nutritional and metabolic diseases, the gender share was 54.4 to 45.6; while by age group, patients in their 50s comprised a 25.1% share, followed by those in their 40s (24.9%) and 60s (22.5%). These results indicate that the cost share for thyroid diseases is higher for younger age groups.
Our findings are meaningful because this study was the first attempt to quantify the socioeconomic impact of thyroid diseases in Korea, but it also has the following limitations. First, we included noncoverage cost items by relying on the percentage of deductible data in the national health care scheme, but deductible data published regularly by the National Health Insurance Service do not include drugs prescribed by practitioners of traditional Asian medicine or health supplements such as vitamins, which means that our results underestimate the direct medical costs incurred by patients making those purchases.
Second, in this study we included hospitalization days and outpatient visits for patients who were diagnosed with thyroid conditions as the primary cause of illness, but we may have underestimated these costs by not including costs for patients diagnosed with thyroid conditions as a secondary cause.
Third, the cost of caregivers differs widely depending on the severity of the illness, so it is possible that a patient may have received care service at home instead of at the hospital. As there is no way of determining these details under the current statistical practice of providing aggregate data, our data were limited to cases in which caregiver cost was incurred in hospitals only. For hospitalized patients, we assumed the caregiver costs by default.
Fourth, to ascertain precise figures when estimating future income loss from premature death and productivity loss resulting from absence from work, we excluded patients who were not currently in the labor market, such as the unemployed (job seekers) and the economically inactive (homemakers, students, and individuals waiting to serve in the military). We may have underestimated the costs due to unremunerated economic activity of unemployed and economically inactive populations.
Fifth, productivity loss resulting from absence from work due to thyroid conditions consists mainly of wage loss, which was estimated using data for hospitalization days and outpatient visits. Although some patients may not have visited medical service providers and instead taken sick leave, there is no way of obtaining these figures, so there is a possibility that true productivity loss may have been underestimated.
For the 8 years between 2002 and 2010, the social cost-of-illness from thyroid conditions increased 3.4 times, from 224.2 billion won to 762.2 billion won. This is twice that for all endocrine, nutritional and metabolic diseases, or for cancer. The total portion of direct costs was 69.7%, with the lion's share associated with the most economically active age groups between 30 and 50. Despite the public perception that thyroid diseases are relatively easy to treat medical conditions, the statistics tell a different story. This is a disease associated with rapidly rising costs in comparison to other medical conditions.
As thyroid diseases occur in age groups that are economically active, high social costs are expected in the future. We hope that this study provides momentum for raising public awareness of the importance of thyroid disease prevention and management in Korea, while encouraging the assignment of higher policy priority to this significant health issue.


 XML Download
XML Download