

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Hypothyroidism should be treated in pregnancy, because it has been associated with an increased risk of adverse pregnancy complications, as well as detrimental effects upon fetal neurocognitive development. The goal of L-thyroxine (LT4) treatment is to normalize maternal serum TSH values within the trimester-specific pregnancy reference range. 50% to 85% of hypothyroid women being treated with exogenous LT4 need to increase the dose during pregnancy. In this study, we report a case of a 29-year-old woman with hypothyroidism who had been in remission and discontinued LT4 treatment during her pregnancy. Three months after delivery she had a relapse of hypothyroidism and was retreated with LT4. Many factors can influence the gestational requirement for LT4, therefore maternal serum TSH should be monitored and the LT4 dose should be adjusted in pregnant patients with treated hypothyroidism.
Figures and Tables
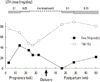
Fig. 1
Serum free thyroxine (T4) and thyroid stimulating hormone binding inhibitory immunoglobulin (TBII) change during pregnancy and postpartum. The dosage of L-thyroxine (LT4) treatment is shown at the top. LT4 treatment was discontinued at 23 weeks of pregnancy, and restarted at 16 weeks after delivery.
References
1. Abalovich M, Gutierrez S, Alcaraz G, Maccallini G, Garcia A, Levalle O. Overt and subclinical hypothyroidism complicating pregnancy. Thyroid. 2002. 12:63–68.
2. Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, O'Heir CE, Mitchell ML, Hermos RJ, Waisbren SE, Faix JD, Klein RZ. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999. 341:549–555.
3. Alexander EK, Marqusee E, Lawrence J, Jarolim P, Fischer GA, Larsen PR. Timing and magnitude of increases in levothyroxine requirements during pregnancy in women with hypothyroidism. N Engl J Med. 2004. 351:241–249.
4. Stagnaro-Green A, Abalovich M, Alexander E, Azizi F, Mestman J, Negro R, Nixon A, Pearce EN, Soldin OP, Sullivan S, Wiersinga W. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011. 21:1081–1125.
5. Nelson JC, Palmer FJ. A remission of goitrous hypothyroidism during pregnancy. J Clin Endocrinol Metab. 1975. 40:383–386.
6. Lu R, Burman KD, Jonklaas J. Transient Graves' hyperthyroidism during pregnancy in a patient with Hashimoto's hypothyroidism. Thyroid. 2005. 15:725–729.
7. Abalovich M, Amino N, Barbour LA, Cobin RH, De Groot LJ, Glinoer D, Mandel SJ, Stagnaro-Green A. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2007. 92:8 Suppl. S1–S47.
8. Glinoer D, Abalovich M. Unresolved questions in managing hypothyroidism during pregnancy. BMJ. 2007. 335:300–302.
9. Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study. Clin Endocrinol (Oxf). 2003. 59:282–288.
10. Negro R, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Stagnaro-Green A. Increased pregnancy loss rate in thyroid antibody negative women with TSH levels between 2.5 and 5.0 in the first trimester of pregnancy. J Clin Endocrinol Metab. 2010. 95:E44–E48.
11. Yassa L, Marqusee E, Fawcett R, Alexander EK. Thyroid hormone early adjustment in pregnancy (the THERAPY) trial. J Clin Endocrinol Metab. 2010. 95:3234–3241.
12. Kaplan MM. Monitoring thyroxine treatment during pregnancy. Thyroid. 1992. 2:147–152.
13. Glinoer D. The regulation of thyroid function in pregnancy: pathways of endocrine adaptation from physiology to pathology. Endocr Rev. 1997. 18:404–433.
14. Loh JA, Wartofsky L, Jonklaas J, Burman KD. The magnitude of increased levothyroxine requirements in hypothyroid pregnant women depends upon the etiology of the hypothyroidism. Thyroid. 2009. 19:269–275.
15. Feingold SB, Smith J, Houtz J, Popovsky E, Brown RS. Prevalence and functional significance of thyrotropin receptor blocking antibodies in children and adolescents with chronic lymphocytic thyroiditis. J Clin Endocrinol Metab. 2009. 94:4742–4748.
16. Amino N, Izumi Y, Hidaka Y, Takeoka K, Nakata Y, Tatsumi KI, Nagata A, Takano T. No increase of blocking type anti-thyrotropin receptor antibodies during pregnancy in patients with Graves' disease. J Clin Endocrinol Metab. 2003. 88:5871–5874.
17. Brown RS, Bellisario RL, Botero D, Fournier L, Abrams CA, Cowger ML, David R, Fort P, Richman RA. Incidence of transient congenital hypothyroidism due to maternal thyrotropin receptor-blocking antibodies in over one million babies. J Clin Endocrinol Metab. 1996. 81:1147–1151.
 XML Download
XML Download