

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Patients with pheochromocytoma manifest with headache, perspiration, and palpitation. Although most patients have either sustained or paroxysmal hypertension, some patients present with hypotension. However, severe orthostatic hypotension is relatively rare in patients with pheochromocytoma. We report here on a 72-year-old woman with pheochromocytoma and she presented with recurrent syncope due to hypotension and blood pressure fluctuation. Syncope due to hypotension is unusual in patients with pheochromocytoma and only a few such cases have been reported. The present case serves to illustrate an unexpected presentation of this tumor.
Figures and Tables
Fig. 1
Preoperative 3D thoracic aorta CT showed a 3.3-cm-sized mass with irregular margin (arrow) in left upper lobe suggesting lung cancer (A), and a 5.5-cm-sized hypodense mass with internal hemorrhage (arrow) in left adrenal gland (B).

Fig. 3
Preoperative imaging study. A. On whole body PET/CT scan, the mass in left upper lobe showed mild 18F-FDG uptake (max SUV > 2.97). B. On 131I-MIBG scan, moderate radiotracer uptake was showed around the left supra-adrenal area (corresponding the mass in left adrenal area on CT scan) throughout all images on 24 hours, 48 hours, and 72 hours.
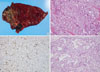
Fig. 4
Histopathological findings of the adrenal pheochromocytoma (A-C) and lung adenocarcinoma (D). A. Cross-section of tumor showed cystic change with necrosis and hemorrhage. B. Microscopic finding of tumor showed typical zellballen pattern. Tumor cells had basophilic granular cytoplasm and round nuclei (H&E staining, × 200). C. Immunohistochemical staining of tumor cells revealed brownish S-100 positive sustentacular cells at the peripheries of the tumor cell clusters (S-100 protein staining, × 200). D. Microscopic finding of lung adenocarcinoma in the left upper lobe. The tumor showed irregular glandular cells having hyperchromatic nuclei in a fibrous stroma (H&E staining, × 200).
References
1. Ilias I, Pacak K. Current approaches and recommended algorithm for the diagnostic localization of pheochromocytoma. J Clin Endocrinol Metab. 2004. 89:479–491.
2. Pacak K, Linehan WM, Eisenhofer G, Walther MM, Goldstein DS. Recent advances in genetics, diagnosis, localization, and treatment of pheochromocytoma. Ann Intern Med. 2001. 134:315–329.
3. Shaw TR, Rafferty P, Tait GW. Transient shock and myocardial impairment caused by phaeochromocytoma crisis. Br Heart J. 1987. 57:194–198.
4. Kobal SL, Paran E, Jamali A, Mizrahi S, Siegel RJ, Leor J. Pheochromocytoma: cyclic attacks of hypertension alternating with hypotension. Nat Clin Pract Cardiovasc Med. 2008. 5:53–57.
5. Ueda T, Oka N, Matsumoto A, Miyazaki H, Ohmura H, Kikuchi T, Nakayama M, Kato S, Imaizumi T. Pheochromocytoma presenting as recurrent hypotension and syncope. Intern Med. 2005. 44:222–227.
6. Guzik P, Wykretowicz A, Wesseling IK, Wysocki H. Adrenal pheochromocytoma associated with dramatic cyclic hemodynamic fluctuations. Int J Cardiol. 2005. 103:351–353.
7. Baxter MA, Hunter P, Thompson GR, London DR. Phaeochromocytomas as a cause of hypotension. Clin Endocrinol (Oxf). 1992. 37:304–306.
8. Streeten DH, Anderson GH Jr. Mechanisms of orthostatic hypotension and tachycardia in patients with pheochromocytoma. Am J Hypertens. 1996. 9:760–769.
9. Song IA, Jung HJ, Cho DS, Yun JY. Unpredicted tachycardia and hypotension in a patient with medullary thyroid cancer and undiagnosed pheochromocytoma: A case report. Korean J Anesthesiol. 2009. 57:254–258.
10. Bortnik M, Occhetta E, Marino P. Orthostatic hypotension as an unusual clinical manifestation of pheochromocytoma: a case report. J Cardiovasc Med (Hagerstown). 2008. 9:839–841.
11. Shin DH, Kim SG, Kim DR, Kim NH, Choi KM, Baik SY, Choi DS, Suh SO. Clinical study of the pheochromocytoma. J Korean Soc Endocrinol. 2002. 17:554–563.
12. Ramsay ID, Langlands JH. Phaeochromocytoma with hypotension and polycythaemia. Lancet. 1962. 2:126–128.
13. Page LB, Raker JW, Berberich FR. Pheochromocytoma with predominant epinephrine secretion. Am J Med. 1969. 47:648–652.
14. de Leeuw PW, Waltman FL, Birkenhager WH. Noncardiogenic pulmonary edema as the sole manifestation of pheochromocytoma. Hypertension. 1986. 8:810–812.
15. Lever AF, Mowbray JF, Peart WS. Blood flow and blood pressure after noradrenaline infusions. Clin Sci. 1961. 21:69–74.
 XML Download
XML Download