

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Definitive radiation therapy (RT) for cervical cancer has changed dramatically over the last few decades in terms of two major advances, the combination use of chemotherapy and RT technological advances. Concomitant chemoradiation therapy (CRT) has become widely accepted as the standard care for locally advanced cervical cancer according to the Clinical Announcement by the US National Cancer Institute in 1999 [12]. Chemotherapy serves as a radiosensitizer that enhances the activity of radiation, and as a direct cytotoxin to local tumor cells and subclinical distant metastases beyond the radiation field [3]. A recent meta-analysis of 13 randomized controlled trials comparing CRT versus RT found a 6% improvement in 5-year survival in favor of CRT, with a hazard ratio of 0.81 (p<0.001) [45]. CRT also reduced local and distant cervical cancer recurrence and progression, and improved disease-free survival, in particular, in the International Federation of Gynecology and Obstetrics (FIGO) stages I–II disease [4]. At the same time, extensive RT technological advances have been made, especially in the field of brachytherapy. Image-guided brachytherapy (IGBT) has allowed the delineation of clinical target volumes (CTVs) and organs at risk, resulting in a dose prescription for these volumes. IGBT has also allowed for adaptive brachytherapy to the tumor at the time of treatment, taking tumor regression into account [6]. Thus, IGBT have provided improvements in dose distribution and dose escalation to the target, leading to high local control rates, even in advanced stages of cervical cancer [7].
However, locoregional and distant failures were still encountered. Once recurrence occurs, further treatment options are severely limited and the outcome is usually dismal. Up until now, recurrence patterns have been shown in only a few studies [68]; it seems that distant metastases became the first site of recurrence, caused by increased locoregional control rates [69]. Mazeron et al. [6] reported that among 163 patients, with a median follow-up of 36 months, who were treated with CRT for FIGO stages IB–IVA diseases, those who developed distant metastasis as the first relapse accounted for 68.7% of all relapses, and, of these, half were isolated; however, details remain to be investigated. The purpose of this retrospective study was to clarify the details of recurrence patterns and sites in a large cohort of cervical cancer patients treated with modern definitive RT at a single institution.
MATERIALS AND METHODS
1. Patient population
Between 2001 and 2013, data was obtained on consecutive patients who met the following eligibility requirements: a diagnosis of pathologically confirmed cervical cancer, FIGO clinical stages IB to IVA disease, and received definitive RT consisted of external beam radiation therapy (EBRT) and high-dose rate intracavitary or interstitial brachytherapy (HDR-ICBT and HDR-ISBT, respectively) at our institution. Patients with para-aortic lymph node (PALN) metastasis were included. Patients were excluded if they: did not complete the planned RT, received any prior treatment for cervical cancer except conization, had other simultaneous uncontrollable malignancies, and/or were not followed at our institution.
This research was reviewed and approved by the Institutional Review Board of the University of Tokyo Hospital. All patient identifiers were removed prior to the analysis of data.
2. Pretreatment evaluation
All patients were clinically evaluated for their pretreatment state by a physical and pelvic examination without anesthesia, a biopsy of the primary tumor, a complete blood cell count and biochemistry profile, a computed tomography (CT) of chest, abdomen and pelvis, and by magnetic resonance imaging (MRI) of the pelvis. Drip infusion pyelography, cystoscopy, and rectoscopy were performed when possible. Prior to 2008, [18F]-fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) was performed when possible, and from 2008, it was routinely performed. Pelvic lymph nodes (PLNs) greater than or equal to 10 mm in diameter on CT or MRI, considered to be metastases by specialists in diagnostic radiology, or positive by FDG-PET (diagnosed by specialists in nuclear medicine) were assessed as positive. All patients were assigned to a clinical stage on the basis of their FIGO classification.
3. Treatment schedule
RT consisted of EBRT to the whole pelvis as well as HDR-ICBT. EBRT was administered with 6 or 10 MV photon-beams to the whole pelvis using a four-field box technique. The CTV included the whole uterus, vagina, parametrial region, as well as the regional lymph node (LN) area, and for PALN-positive patients, the PALN area was also irradiated. The planning target volume consisted of the CTV plus a 0.5 to 1.0 cm margin. The daily dose was 1.8 to 2.0 Gy, delivered once a day, 5 days a week. Depending on tumor size, the whole pelvis was irradiated with up to 20 to 40 Gy, then a boost was performed, to between 50 to 50.4 Gy, to the parametrium with a 4 cm-wide central block using the anteroposterior parallel two-field technique. For PLN metastasis greater than or equal to 10 mm minimum in diameter on CT or MRI, a boost of 10 Gy in 2 Gy fractions was delivered to PLN metastases at the clinician’s discretion.
At the insertion of the central block to EBRT, HDR-ICBT was started, using an Iridium-192 remote after loading technique, in 6 Gy fractions, once or twice a week, for a minimum of 3 to 4 fractions (microSelectron, Nucletron BV, Veenendaal, The Netherlands). In most cases, the combination of a tandem and ovoid applicator was used for the prescription at point A with CT-based image-guided volume optimization. In cases with lower vaginal extension, a tandem-cylinder was used for the prescription at the 2 cm-line from a tandem in the uterine cavity, and at a 5 mm-line from the applicator surface in the vagina, in order to fully cover the target. Implantation was performed under intravenous anesthesia. At the clinician’s discretion, patients with residual tumors received additional ICBT doses of 4.0 to 4.5 Gy per fraction. For patients with an anatomy not allowing for the application of standard ICBT wherein the tumor could not be encompassed, ISBT was selected. In such cases, EBRT was administered to the whole pelvis, without a central block, up to 45 Gy, and then ISBT was started. Implantation was performed under intravenous and epidural anesthesia through a transperineal route mainly using the Martinez Universal Perineal Interstitial Template (ELEKTA, Stockholm, Sweden). The irradiation was administered twice a day to the primary tumor, with at least 6 hours between each treatment session, for up to 24 Gy in 6 Gy fractions. Prior to 2013, brachytherapy was planned based on CT using PLATO software ver. 14. 2. 6 (Nucletron). From 2013, Oncentra Brachy Treatment Planning (ELEKTA) was used.
The doses to the tumor from both EBRT and HDR-ICBT (or HDR-ISBT) were normalized to the biologically equivalent doses in 2 Gy fractions (GyEQD2) based on the linear-quadratic model using an α/β ratio of 10 Gy.
Combined chemotherapy was used for patients with locally advanced disease (IIB–IVA), a bulky tumor larger than 4 cm as the minimum diameter, and/or LN metastasis. A chemotherapy agent was administered on the first day of RT. From 2001 to 2007, cisplatin was administered at 75 mg/m2, tri-weekly, for 3 cycles. After 2007, cisplatin (40 mg/m2 weekly for 6 cycles) or nedaplatin (75 to 100 mg/m2 tri-weekly for 3 cycles) became the principal drugs of the chemotherapy regimen. At the clinician’s discretion, cases with advanced age, lower performance status, or renal dysfunction were given a reduction in dose.
4. Follow-up and analysis of response and survival
Follow-up was performed every month for the first year, every 2 to 3 months for the second year, and every 3 to 6 months thereafter. Follow-up procedures included physical and pelvic examinations, cervical Papanicolaou smears, and tumor markers. Chest to pelvic CT was scanned at an interval of 3 to 6 months for the first 2 years, and 6 to 12 months thereafter. Pelvic MRI or FDG-PET was performed when necessary.
A complete response (CR) was defined as no evidence of disease 3 months after the end of RT, evaluated by clinical and radiographic examinations. If there was persistence or progression of disease at that time, the effect of treatment was determined as “non-CR.” Disease after achieving of CR was defined as recurrence. A diagnosis of residual disease, progression, or recurrence was based on physical or radiographic examinations or pathological confirmation.
Statistical analyses were performed using JMP 11 (SAS Institute Inc., Cary, NC, USA). The survival period was defined as the time between the start of RT and either progression, death from any cause, or the last follow-up date. Survival curves were calculated using the Kaplan-Meier method, and log-rank tests were used to compare survival distributions. Differences in patient or tumor characteristics were analyzed by the chi-square test or Fisher exact test for 2×2 columns. Differences with values of p<0.05 were considered statistically significant.
RESULTS
1. Patient characteristics
One hundred and thirty-seven reviewable patients formed the cervical cancer patient cohort for this analysis. The last follow-up was performed on September 2014. The crude median follow-up period for all patients and for surviving patients was 41.3 months (range, 4.0 to 150.1 months) and 57.0 months (range, 5.2 to 150.1 months), respectively. Patient and tumor characteristics are shown in Table 1. Briefly, the median age of all patients was 58 years (range, 28 to 89 years), the most frequent stage was IIIB (n=55, 40%), and the median maximum tumor diameter measured by a T2-weighted image from MRI was 4.8 cm (range, undetectable to 14.3 cm). Usually, HDR-ICBT using a tandem and ovoid applicator was performed; however, a tandem-cylinder applicator was used in 13 patients, and HDR-ISBT was performed in three patients. For 12 out of 15 patients treated during or before 2002, CT scans for HDR-ICBT was not obtained. Out of 48 PLN-positive patients, 12 patients received EBRT boosts.
Table 1
Patient and tumor characteristics

2. Survival outcome
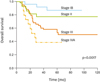
At the time of analysis, 92 patients were alive, and 45 patients had died—40 as a result of their malignancy and five due to other causes. The 5-year overall survival (OS) rate for all patients was 63.9%±4.6%, and those for patients with stages I, II, III, and IVA disease were 87.1%±7.1%, 78.0%±8.0%, 54.3%±7.0%, and 40.0%±12.7%, respectively (Fig. 1). The 5-year progression-free survival (PFS) rate for all patients was 60.6%±4.3%.
3. Patterns of recurrence
The initial response and the patterns of recurrence are shown in Fig. 2. Out of the 137 patients, 121 patients (88%) achieved a CR. On the other hand, 16 patients (12%) experienced persistence and/or progression of disease.
Fig. 2
The initial response and patterns of first recurrence. AWD, alive with disease; CR, complete response; DOD, died of disease; MST, median survival time; NED, no evidence of disease; Rec, recurrence; RT, radiation therapy.

Among the 16 non-CR patients, all but one patient died of disease, with a median survival time (MST) of 10.9 months (95% CI, 7.8 to 13.5) from the start of RT. The remaining patient also died 2 months after the time of analysis.
Among the 121 patients with a CR, 36 patients (30%) developed recurrence, with a median interval of 9.3 months (95% CI, 7.9 to 11.5) from the start of RT. This interval was within 1 year in 69% of patients, and more than 2 years in only three patients (8.3%). The MST from the recurrence was 16.4 months (95% CI, 11.2 to 24.2). The first sites of recurrence were as follows: intra-RT field in nine, outside RT field in 20, and both intra- and outside RT field in seven patients.
4. Details of recurrence sites
The details of the non-CR patients and the first recurrence sites of recurrence patients are shown in Tables 2,3,4,5.
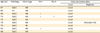
Table 2
Details of non-complete response patients (n=16)

Table 5
Details of both of intra- and outside radiation therapy field recurrence patients (n=7)

Among 16 non-CR patients (Table 2), eight patients showed residual disease, of which three had synchronous distant progression, even though they received concurrent chemotherapy. The remaining eight patients experienced new distant metastasis without residual disease, even though all but one patient also received concurrent chemotherapy. Of these, new isolated PALN metastasis occurred in two patients. In this non-CR group, all patients showed locally advanced disease stages IIB–IVA, and there was a trend of younger patients, with a median age of 54 years. Clinicopathologic factors were compared between CR and non-CR patients by the chi-square test. As a result, non-CR patients significantly correlated with an advanced stage (III–IV vs. I–II, p=0.042), a positive PLN (positive vs. negative, p=0.012), a positive PALN (positive vs. negative, p=0.023), a larger maximum tumor diameter (>5 cm vs. ≤5 cm, p<0.001), and a lower initial hemoglobin level (≤10 g/dL vs. >10 g/dL, p<0.001). All patients died of disease.
In the intra-RT field recurrence group (Table 3), all patients had locally advanced disease. Although the tumor RT dose was not significantly lower (median tumor dose: 69.2 GyEQD2 in patients with intra-field recurrence and 62.1 GyEQD2 in patients without recurrence), all patients developed a local recurrence. Interestingly, however, no one showed an isolated PLN recurrence. In this group, two patients with local recurrence alone were salvaged by surgery and survived for 54.6 and 45.7 months, respectively..
Table 3
Details of first recurrence sites of intra-radiation therapy field recurrence patients (n=9)
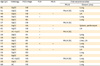
Among 20 patients with recurrence outside of RT field (Table 4), lung was the most frequent site which was observed in 12 patients (60%). Oligo-recurrence of PALN occurred in only two initially PALN-negative patients. In this group, four patients were salvaged with no evidence of disease at the time of analysis; three with oligo-recurrence of lung were salvaged by surgery or stereotactic RT, and one with oligo-recurrence of mediastinal LN was salvaged by CRT; their survival periods from the time of recurrence were 48.0, 66.9, 36.1, and 74.5 months, respectively. Furthermore, in this group, only four patients experienced a sequential intra-RT field recurrence afterwards no longer than a year. This means that the remaining patients suffered from a distant lesion alone.
Table 4
Details of outside radiation therapy field recurrence patients (n=20)
In seven patients with both intra- and outside RT field recurrence (Table 5), five patients died of the original disease. The remaining two patients, both in the early period of their salvage chemotherapy, were still alive with disease.
In regard to the regional control of all 137 patients, 48 were PLN-positive and 89 were PLN-negative. Of the 48 PLN-positive patients, only 12 received EBRT boosts to the PLN metastasis and 36 did not (the median dose was 49.6 GyEQD2 to the positive PLN, as well as regional areas). Two out of the 12 boosted patients, and four out of the 36 non-boosted patients, developed PLN persistence or recurrence as the first relapse, respectively. Of the 89 PLN-negative patients, one developed PLN recurrence as the first relapse. Thus, only seven patients (5.1%) developed PLN disease, and importantly, all of them were not isolated but showed another synchronous disease. Sites of nodal disease were the common iliac, internal iliac, and obturator LN, mainly (5/7 patients) at initially involved, not new, PLN. No disease was observed at the external iliac or presacral nodes.
PALN progression or recurrence was mostly new to initially PALN-negative patients; failure for initially involved PALN occurred in only one patient, and also with new and synchronous PALN metastasis. Among PALN-negative patients (n=119), isolated PALN metastasis occurred in two patients up to 3 months after RT, and in two patients after achieving a CR (total n=4 [4/119=3.4%]).
DISCUSSION
Several reports concerning patterns of recurrence in cervical cancer have previously been published [6891011]. Mazeron et al. [6] reported that among 163 patients treated with CRT, those who developed distant metastasis as the first relapse amounted to 68.7% of all relapses, and, of these, half were isolated. Teh et al. [8] also reported that distant failures predominated over local failures, with local control rates of 81.7%, whereas distant control rates were 70.8% at 5 years. Our results were also consistent with these reports. Outside RT field recurrence predominated over intra-RT field recurrence (20 patients vs. 9 patients among 36 recurrence patients). However, to our knowledge, this is the first report describing more detailed recurrence sites after definitive RT using modern treatment techniques, with additional findings from this detailed analysis.
Firstly, local persistence and recurrence accounted for half of non-CR patients and all of intra-RT field recurrence patients, respectively. This suggests the need for dose escalation to the primary tumor, especially in patients with locally advanced disease and/or patients who responded poorly to prior EBRT.
Indeed, the cumulative doses prescribed at point A adopted in Japan (62 to 65 GyEQD2) were remarkably lower than those used in global schedules (85 GyEQD2) [12]. In Japan, a phase II trial of concurrent CRT based on this schedule (Japanese Gynecologic Oncology Group 1066) was conducted, and demonstrated that it could provide favorable pelvic control and PFS rates; it appeared to be comparable to previously reported data, with a low incidence of severe late toxicity [12]. However, in this study, the authors also noted that there remained room for improvement in local control, particularly for patients with large tumors who frequently developed pelvic recurrence.
Furthermore, recent RT technology in brachytherapy is becoming highly precise, especially in IGBT. Planning aims have also changed to deliver to 90% of high risk CTV (D90), not to point A, following the recommendation of the Groupe Européen de Curiethérapie-European Society for Radiotherapy & Oncology (GEC-ESTRO) [13]. Dimopoulos et al. [14] demonstrated a dose-effect relationship in patients treated with HDR-MRI-guided brachytherapy. Potter et al. [7] showed excellent local control rates, even in advanced disease, using MRI-guided adaptive ICBT including needle insertion (prescribed to D90 >85 Gy). As a result, presently in our institution, MRI-guided ICBT is administered particularly to advanced cases, and we also prescribe at least 6 Gy per fraction to D90.
Secondly, regional control was favorable, even in initially PLN-positive patients. Of all 137 patients, including 48 PLN-positive patients, only seven patients (5.1%) developed PLN disease, and importantly, all of them were not isolated but displayed another synchronous disease. Recently, several researchers have reported the efficacy of EBRT boosts to metastatic PLN to reduce PLN recurrence [151617181920]. However, this current analysis suggests that EBRT boosts may not be necessary for all PLN-positive cases, because nodal control was favorable and PLN persistence and recurrence were always observed with other synchronous relapses. PLN metastasis is reported to be a significant prognostic indicator for developing distant metastasis, including PALN recurrence [1520]. Therefore, additional systemic chemotherapy, with or without prophylactic PALN irradiation, rather than EBRT boosts may be an appropriate treatment option to further improve outcomes for patients with positive PLN.
Additionally in regard to regional areas, sites of nodal disease were the common iliac, internal iliac, and obturator LN, while disease was not observed at the external iliac nor presacral nodes. Kasuya et al. [21] investigated details of distribution patterns of metastatic PLNs in patients with cervical cancer. There were some differences of definition of regional areas between this study and our study, and in this study, regional areas were further divided into some subregions. The majority of patients had positive nodes in the cranial obturator and/or the medial external iliac region. In contrast, few had positive nodes in the lateral external iliac, caudal external iliac, caudal obturator, internal iliac and presacral regions. All these areas have usually been included in standard CTV. However, using intensity-modulated radiation therapy, a dose adjustment in these regional areas, divided into high and low risk areas, will become possible in PLN-negative patients.
Isolated PALN metastasis was less frequent than was first thought, occurring in two patients up to 3 months after RT, and in two patients after achieving CR, among 119 PALN-negative patients (4/119=3.4%). Cervical cancer spreads through the lymphatic route rather than hematogenously [2223] and the first site of distant metastasis is PALN. This has been confirmed in a large population-based study [2223]. Furthermore, RT for oligo-recurrence of PALN has been well reported [24]. However, the benefits of extended field RT plus chemotherapy in PLN-positive patients with a supposedly 20% to 25% risk of subclinical PALN involvement remain unclear. Our findings suggest that such benefits may be limited. Yap et al. [25] also reported, in their prospective study of 228 patients treated with CRT, that the addition of PALN irradiation was not associated with a significant difference in disease-free survival, OS, and the rate of PALN relapse. In their study, isolated PALN relapse rates after pelvic RT alone were 2.6%. They theorized that cisplatin chemotherapy effectively treated micro-metastatic disease in the para-aortic chain and offset the potential benefit of PALN irradiation. Furthermore, our findings suggest that the most frequent isolated distant metastatic site in cervical cancer has changed from PALN to lung in the era of CRT.
The predominance of outside RT field recurrence over intra-RT field recurrence, and that almost all patients with outside RT field recurrence alone were free from intra-RT field recurrence for a long time, both highlight the issue of distant control. Reducing distant failures is a challenge that must be faced in order to improve outcomes. Recently, the need for consolidation chemotherapy for selected patients with locally advanced cervical cancer has been under debate [26]. We think that patients who achieve a benefit from adjuvant chemotherapy will be present in definite proportions. The Gynecologic Oncology Group is also starting a randomized study on adjuvant chemotherapy in high-risk patients (three cycles of carboplatin plus paclitaxel), termed the OUTBACK trial [27]. In addition, several molecular targeting agents are being used for cancer patients [16].
Finally, isolated recurrences may have a chance to be cured with aggressive local cancer treatments such as RT or surgery, with or without chemotherapy. In this current study, two cases with isolated local recurrences were salvaged by surgery, and three cases in the oligo-recurrent state also gained in longer survival times after salvage surgery or RT. Oligo-recurrence has been defined by Niibe et al. [232829] and it is one of the recent topics in oncology. In the state of oligo-recurrence, recurrent sites with a controlled primary lesion were treated with local therapy, meaning that all gross recurrent sites could be treated using local therapy [23]. Careful follow-up plus being alert to an opportunity for salvage therapy were important.
There was a potential limitation in this study in that being a retrospective study in nature, there was a lack of consistency in patients, diseases, treatments, and in assessments of toxicity.
In conclusion, local disease was a major type of intra-RT field recurrence. This suggests that there remains room for improvement in local control. On the other hand, PLN control was favorable, even in initially PLN-positive patients, and PLN may be able to be divided into high and low risk areas. Furthermore, the predominance of outside RT field recurrence alone highlights issues of distant control, including the intensity enhancement of systematic therapy.
 XML Download
XML Download