

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It is well known that epithelial ovarian cancer (EOC) is one of the main life-threatening genital tract malignancies in women throughout the world. In Japan, approximately 7,000 cases of EOC are diagnosed every year, and an estimated 4,467 women died of this disease in 2007 [1]. Despite the use of advanced strategic therapies, including surgery and chemotherapy, the 5-year overall survival (OS) rate is approximately 30% [2,3,4,5]. EOC accounts for approximately 90% of ovarian malignancies, and it is commonly diagnosed at a menopausal age. Previous reports have indicated that EOC in women of reproductive age account for 3%-17% of all cases [6,7,8,9]; these patients are often concerned with preserving their fertility in spite of their anxiety regarding the clinical outcome. Accordingly, fertility-sparing surgery has been selected for patients with EOC on the basis of several criteria, including the patients' strong desire, disease stage, histological type, and tumor differentiation [10,11,12,13,14]. On the basis of a previous study, younger women with EOC showed a better prognosis than older patients; however, age was not an independent prognostic factor because of a strong association with increasing rates of an early Federation of Gynecology and Obstetrics (FIGO) stage, borderline malignancy tumors, and a lower grade [7]. On the other hand, Chan et al. [15] reported that a younger age independently leads to a better prognosis. Therefore, it is controversial whether age is a prognostic factor. The majority of previous reports were from European countries or the United States. However, patients' characteristics at reproductive age differ between Western and Asian countries. For example, clear-cell carcinoma of the ovary is the second most frequent subtype of EOC in Japan, although it represents <10% of all cases of EOC diagnosed in the United States [16,17]. In addition, after restricting study participants to those of reproductive age with a stage I tumor, mucinous adenocarcinoma is the most common histology among all pathological subtypes [12]. However, there are few reports on the clinical characteristics of younger patients with EOC from Japan and other Asian countries.
In this study, we examined the long-term oncologic outcome and clarified the clinicopathologic features of younger patients with EOC in Japan compared to older patients.
MATERIALS AND METHODS
1. Patients
We reviewed the medical records of the Tokai Ovarian Tumor Study Group, composed of Nagoya University Hospital and affiliated, cooperating hospitals. Data on women with EOC were collected between 1987 and 2010. This study was approved by the ethics committee of Nagoya University. All surgical specimens were pathologically reviewed by 1 or 2 pathologists blinded to the patients' clinical data. Patients who received neoadjuvant chemotherapy or were lost to follow-up after surgery were excluded from this analysis. Borderline tumors were not included. Inclusion criteria for selecting patients were as follows: (1) those who received primary surgery and whose histological types were known; and (2) those with clinical staging based on the findings of clinical examination and a computed tomography (CT) scan, and/or surgical staging. Primary laparotomy was performed in all patients to assess their abdominal contents. In principle, standard primary surgical treatment includes a hysterectomy, bilateral salpingo-oophorectomy, infracolic omentectomy, retroperitoneal lymphadenectomy, or sampling. If young patients desired fertility preservation, we performed conservative surgery (n=64), including at least unilateral salpingo-oophorectomy with peritoneal staging. Detailed criteria of fertility-sparing surgery were described previously [18]. If patients were at an advanced age with a gross residual tumor or showed severe complications that were a physical burden for radical surgery, retroperitoneal lymphadenectomy was not performed. When retroperitoneal lymphadenectomy was not performed, the absence of swollen lymph nodes >1 cm in diameter was confirmed on a preoperative CT scan, and, if present, palpable nodes were sampled. Staging was evaluated according to the International FIGO classification system. We selected a cutoff of 40 years of age, as this age is widely viewed as a period of transition from a fertile to an infertile age [12,19,20,21,22]. In this study, we divided patients into 2 groups: group A, patients aged ≤40 years of age at the time of the primary operation; and group B, patients aged >40 years.
2. Follow-up and analysis
At the end of treatment, all patients underwent a strict follow-up consisting of several clinical checkups, including a pelvic examination, transvaginal and/or transabdominal ultrasonography, CA-125 evaluation, magnetic resonance imaging, and periodic CT scans. The OS was defined as the time between the date of surgery and last date of follow-up or death from any cause. The distributions of clinicopathologic events were evaluated by using the chi-squared test or Student t-test. Survival curves were determined by using the Kaplan-Meier method. Comparison between the curves was conducted by using the log-rank test. Univariate and multivariate analyses were performed with the Cox proportional hazards model to evaluate the independent factors affecting survival. A p-value of <0.05 was considered statistically significant.
RESULTS
The clinicopathologic characteristics of all patients are shown in Table 1. The median follow-up time was 45.1 months (range, 1 to 257 months). In group A, 134 patients (67.3%) had stage I tumors. On the other hand, the proportion of patients with stage I tumors was only 42.6% in group B. Patients in group B had significantly more advanced tumors than those in group A (p<0.001). With respect to the histological type, patients in group A were more likely to be diagnosed with mucinous adenocarcinoma than those in group B. There was a significant difference in the CA-125 level between group A and B (p<0.001).
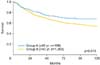
Firstly, we compared the prognosis between the 2 groups. On Kaplan-Meier analysis, the 5- and 10-year OS rates in group A were 73.3% and 68.8%, and those in group B were 64.4% and 54.0%, respectively. There was a significant difference between the 2 groups in the OS (p=0.013) (Fig. 1). However, upon stratification according to the stage of the tumor, there were no significant differences in the OS between the 2 groups (group A vs. B: stage I, p=0.533; stage II-IV, p=0.407) (Fig. 2). Moreover, there was a significant difference in the OS between the 2 groups stratified according to their preoperative CA-125 level (≤200 vs. >200; p<0.001).
With regard to univariate analysis, we subsequently stratified patients according to their age, FIGO stage, histological type, and preoperative CA-125 level (Table 2). As a result, all the above-mentioned factors were identified as factors associated with a poorer OS. To eliminate selection bias from a number of clinicopathologic factors, these categories were entered into a multivariate OS analysis system. The FIGO stage, histological type, and CA-125 level retained significance as prognostic factors for OS. However, age was not an independent prognostic indicator for the OS (age, 41-65 years vs. ≤40 years: hazard ratio [HR], 0.922; 95% confidence interval [CI], 0.693 to 1.250, p=0.592; age, ≥66 years vs. ≤40 years: HR, 1.180, 95% CI, 0.839 to 1.677, p=0.344) (Table 2).
DISCUSSION
EOC is a life-threatening malignancy in women, and it is commonly diagnosed at a menopausal age. To minimize the adverse effects of aggressive surgical procedures and to preserve fertility in young patients, it is desirable for prognostic factors to be accurately evaluated. Most of the previous reports were from the United States and European countries; genetic background and ethnicity may influence prognosis. In this study, we investigated the clinical features of Japanese patients stratified into younger and older age groups. Our data showed that the 199 patients aged ≤40 years comprised 12.7% of all patients, which was consistent with previous studies [6,7,8,9]. With respect to the FIGO stage, 67.3% of the younger group had stage I disease as opposed to 42.6% of the older group, while 20.6% of the younger group had stage III-IV disease compared with 43.8% of the older group. Moreover, younger patients more frequently showed a mucinous pathology (36.7% vs. 13.5%, respectively) and less frequently showed a serous type (14.6% vs. 39.0%) compared with older patients. Bozas et al. [6] reported that, in patients with EOC aged ≤40 years, 30% had stage I disease and 8% had a mucinous type. The rate of clear-cell histology in both young and old patient groups was approximately 25%. According to a report by Duska et al. [7], in younger patients aged ≤40 years, 42.4% had stage I disease and 21% had a mucinous type. Another report showed that 39.2% had stage I disease and 29.7% had a mucinous type [23]. In these 3 studies, less than 10% of all cases of EOC have clear-cell histology. It is well known that clear-cell carcinoma is more frequent in Japan than in Western countries; the clear-cell type may be associated with a poorer prognosis. In comparison with these 3 previous reports, our results showed a higher rate of stage I disease.
In the present study, univariate analysis showed that a younger age was a significantly favorable prognostic factor, but the significance was not apparent on multivariate analysis. This suggests that the results were biased according to the distribution of the stage of the tumor and histological type. The prognostic value of patient age has been controversial. Most previous studies demonstrated that age is not an independent prognostic factor, although younger women with EOC have a better prognosis than older women [15,24]. On the other hand, Chan et al. [25] reported that a younger age was an independent prognostic factor after limiting the analysis to patients with stage III-IV disease. Indeed, most previous studies regarding EOC were limited to European countries. Unfortunately, there are few reports from Japan or other Asian countries on the clinicopathologic features of EOC. Herrinton et al. [26] reported that the annual incidence of ovarian cancer of Asian migrants in the US and native Asian people was lower than in US-born white women. The genetic background and heredity of the patients may be associated with the different frequencies of the histological subtypes. Taken together, it is important to consider ethnicity when evaluating prognostic factors. Our data were all from Japanese women, and it may reflect the unique features of Asian populations.
In conclusion, on the basis of our data, younger patients have a different clinical profile than older patients. However, they showed a similar long-term prognosis upon stratification according to the stage of the tumor. Younger patients had a significantly higher frequency of mucinous-type, stage I disease than older patients. In addition, a young age was not shown to be an independent prognostic factor for OS. The present study had several limitations because of its retrospective nature, a heterogeneous follow-up period, the possibility of type II error, and a variety of treatment protocols such as different chemotherapy regimens and types of surgery. Identifying prognostic factors of EOC after stratification according to age and ethnicity is essential to assess the effects of treatment, and this will also facilitate the personalized selection of optimal therapeutic modalities for each patient.



 XML Download
XML Download