

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As a minimally invasive technique, laparoscopic surgery is widely used in benign gynecologic diseases and may also be used in malignancies such as endometrial cancer [1], cervical cancer [2], and early ovarian cancer. Recent studies have demonstrated that laparoscopic surgical staging of early ovarian cancer is as safe and adequate as open laparotomy [3].
Technologic advances in endoscopic instrumentation and optics have allowed the development of a less invasive alternative to conventional laparoscopy; Single-port access (SPA) laparoscopic surgery. By using a single multichannel port access system, SPA laparoscopy is an attempt to further enhance the cosmetic benefits of minimally invasive surgery while minimizing the potential risks and morbidity associated with multiple working ports. There have been several reports of SPA laparoscopy utilized to treat benign gynecologic disorders [4,5]. In addition, it was proved that SPA laparoscopic adnexal surgery had comparable operative outcomes to conventional laparoscopic adnexal surgery [6]. In gynecologic malignancy, there is one case series that included two patients who had received lymph node dissection during the staging operation [7]. The number of harvested lymph node in the two patients was only 11 and 13, respectively.
Here we report a case of borderline ovarian tumor treated with SPA laparoscopic staging operation.
CASE REPORT
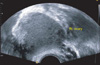
A 34-year-old woman, gravida 2, para 2, visited our clinic with an incidentally found right ovarian cyst. On pelvic examination, she had a palpable non-tender pelvic mass. Transvaginal ultrasonography revealed a 4.0×3.8 cm sized mixed-echogenic right ovarian cyst (Fig. 1). The results of laboratory studies, including analysis of tumor markers, such as CA125, CA19-9, were all within normal limits (CA125, 5.9; CA19-9, 30.2 U/mL). She had received two cesarean sections with a transverse incision, and had no plans for further children. Her height was 160.1 cm and weight was 60.3 kg with a body mass index of 23.53 kg/m2.
We performed a right oophorectomy using the SPA laparoscopy. As the result of intraoperative frozen biopsy of right ovary was a borderline tumor, we decided to change the method of surgery to a staging laparoscopy.
The total operative time was 280 minutes, and the estimated blood loss was 300 mL. On gross examination, the right ovary was enlarged and had a smooth cyst about 4 cm in size, but no other abnormalities were identified. Pathological examination showed a mucinous borderline tumor of the right ovary and patient's surgical stage was diagnosed as Ia. The numbers of resected pelvic lymph nodes were twenty-three. Initial hemoglobin level was 14.3 g/dL, and follow-up level was 13.2 g/dL on the postoperative day 1. There were no intraoperative or postoperative major complications. The abdominopelvic spiral CT was performed postoperatively, and there was no residual lesion. Visual analogue scores for pain at 4 hours and 24 hours after surgery were 6/10 and 4/10 retrospectively. Foley catheter was removed on the morning of the postoperative day 1. She was discharged on the postoperative day 7 after the final pathologic result was confirmed.
1. Surgical technique
The patient was placed in the lithotomic position. The surgeon stood on the left side of the patient, and the first assistant stood on the right side of the patient to handle the scope. The second assistant was positioned between the legs of the patient, manipulating the uterine elevator. The patient's left arm was tied to her body for the surgeon's space. A 2-cm vertical intra-umbilical skin incision was performed via an open Hasson approach. The Alexis® wound retractor (Applied Medical, Rancho Santa Margarita, CA, USA) was inserted through the incision. Then a sterile surgical glove with sheaths inserted into 3 fingers was draped around the rim of the wound retractor. We used a rigid 45-degree, 5-mm laparoscope (IDEAL EYES 5 mm 45 deg, Stryker, San Jose, CA, USA) and 5-mm flexible laparoscope instruments (e.g., Roticulator, Covidien, Mansfield, MA; Cambridge Endoscopic Devices, Framingham, MA, USA) [4]. The abdomen was insufflated to 12 mmHg with CO2 gas and pneumoperitoneum was established. After inspection of the abdominal cavity, washing cytology was performed.
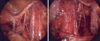
At first, we performed a right salpingo-oophorectomy as previous described [4]. A mucinous borderline ovarian tumor was identified on frozen biopsy. For the staging operation, we used a harmonic scalpel (Harmonic Ace, Ethicon Endo-Surgery Inc., Cincinnati, OH, USA) and a roticular dissector (Fig. 2). Bilateral pelvic lymph node dissection, infracolic omentectomy, and appendectomy were performed using a harmonic scalpel on the right hand and a roticular dissector on the left hand (Fig. 3). Lymph node specimens were extracted using an endobag. Using bipolar and monopolar scissors, SPA laparoscopy-assisted vaginal hysterectomy and left salpingo-oophorectomy was performed [5]. The omentum, appendix, uterus, and left salpinx and ovary were removed through the vagina. Another opening was made on the suprapubic area to place a Jackson-Pratt drain in the pelvic cavity. The trocar was introduced into the pelvic cavity through the suprapubic skin and extracted via the umbilical incision site manipulating with a grasper (Fig. 4). The peritoneum and fascia of the umbilical opening were approximated and closed layer by layer with 2-0 Polysorp (Covidien Syneture, Norwalk, CT, USA) suture. For skin closure, we used dermabond (Ethicon Inc, Somerville, NJ, USA), which provided a good cosmetic outcome and did not require later stitching out.
DISCUSSION
The major principle of minimally invasive surgery is to be less invasive, leading to less physiologic stress, faster recovery, and better cosmetic results. From a technical standpoint, SPA laparoscopy in the field of minimally invasive surgery is the most recently emerging and promising method.
In 1994, Querleu and LeBlanc [8] first demonstrated that laparoscopic surgery may be used to adequately stage ovarian malignancies. Since then, several investigators reported some cases of laparoscopic surgical staging of early ovarian cancer (EOC). Ghezzi et al. [3] described that laparoscopic surgical staging of EOC is as safe and adequate as the standard surgical staging performed via laparotomy, and offers a shorter hospital stay. In 2009 Fader and Escobar [7] first demonstrated in a series of patients referred for staging that SPA laparoscopic surgery may be used to adequately stage ovarian malignancies. The study of two port access staging laparoscopy was reported recently as a feasible procedure in selected gynecologic cancer patients [9].
In accordance with a previous study [7], we demonstrated that staging operation of early ovarian cancer may be performed using SPA laparoscopy. Furthermore, the number of lymph nodes in this case is sufficient compared to the results of other studies. Consequently, SPA laparoscopic staging of early ovarian cancer may be accomplished successfully with pelvic lymph node dissection, for patients whose disease appear to be limited to the adnexa.
The limitations of this case are the following. First, paraaortic lymph node dissection was not done due to technical difficulty and a high risk of complications. Second, at the end of the operation, another 3 mm puncture on the suprapubic area was needed to insert the drain tube. This wound may decrease the benefit of SPA surgery in terms of excellent cosmetics. Recent meta-analysis reveals that placement of retroperitoneal tube drains has no benefit in the prevention of lymphocyst formation after pelvic lymphadenectomy in patients with gynecological malignancies [10]. Based on this analysis, the drainage system may be omitted in future cases.
In conclusion, staging operation using SPA laparoscopy was successfully done, and it may be a feasible procedure in selected gynecologic cancer patients who have early-staged ovarian or endometrial cancer, and who are concerned for postoperative scarring. The efficacy, safety, and potential benefits of this technique in cancer staging operation should be evaluated in further trials.


 XML Download
XML Download