

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Surgical decompression of the facial nerve in patients with acute facial paralysis associated with Bell's palsy or herpes zoster oticus has been discussed and debated for more than 70 years.1 One of the reasons is that clinicians remain unsure about the appropriate management of complete facial paralysis. And another is the potentially life-threatening surgical procedure necessary to expose the peri-geniculate ganglion of the facial nerve. Although many approaches have been proposed for surgical exposure of this area, the middle cranial fossa and transmastoid approaches are the most commonly used ones.234
Successful decompression of the facial nerve greatly depends on successful exposure of the first genu of the facial nerve including the labyrinthine segment, geniculate ganglion, and proximal tympanic segment. The middle cranial fossa approach is known to be the best approach for complete exposure of the first genu of the facial nerve. However, when using this approach, patients must be ready to undergo temporal craniotomy, a potentially somewhat aggressive procedure. An alternative approach is the transmastoid approach; this approach, however, provides only restricted view of the peri-geniculate area, which can be a "key area" for facial nerve decompression, and sometimes requires the performance of some type of ossicular procedure.56
A few clinicians have reported new approaches to expose the geniculate ganglion and labyrinthine segment of the facial nerve without craniotomy, which combine the advantages of the middle cranial fossa and transmastoid approaches.78 The advantages of these new approaches include obviating the need for craniotomy, lack of temporal lobe retraction, wide exposure of the peri-geniculate ganglion, and familiarity of the approach for experienced otologists.
When conducting facial nerve decompression via the transmastoid approach, we have experienced difficulty in approaching the peri-geniculate area because of restricted view due to excessive bleeding, which is attributable to the rich blood supply in this area, and the proximity of the labyrinthine segment to the dura mater of the temporal lobe. For wide exposure of the peri-geniculate area, retraction of temporal lobe after bony removal of tegmen mastoideum has been designed, since it as effective as the middle cranial fossa approach and does not involve craniotomy.
We propose such a new surgical technique of temporal lobe retraction for wider exposure of the peri-geniculate ganglion when using the transmastoid approach without craniotomy and report post-operative facial function.
MATERIALS AND METHODS
Patients
Fifteen patients with traumatic facial paralysis [House-Brackmann (HB) grade IV–VI], 3 patients with Bell's palsy (HB grade V–VI), and 2 patients with herpes zoster oticus (HB grade V–VI) underwent facial nerve decompression surgery between January 2008 and July 2014. All types of traumatic facial paralysis were otic capsule sparing. The surgery was performed via the transmastoid approach using temporal lobe retraction. The mean age of the patients was 39.95 years, and they included 7 women and 13 men.
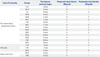
One patient was diagnosed as HB grade IV, 7 as HB grade V, and 12 as HB grade VI. All the patients underwent preoperative tests including high-resolution computed tomography, temporal magnetic resonance imaging with gadolinium enhance-ment, pure tone audiometry, and electroneurography or electromyography (Table 1). Pre- and post-surgical (more than 6 months) evaluation of facial function was performed to assess the effectiveness of the surgery.
In order to determine the improvement of facial function through the facial nerve decompression, it was compared using the HB scale. In this scale, grade I is assigned to normal function, and grade VI represents complete paralysis. Intermediate grades vary according to function at rest and with effort. Pre-and post-operative patients hearing were compared through the pure tone audiometry (Table 1).
Surgical procedure
For the transmastoid approach, the patient should be in a supine position tilting to the contralateral side at approximately a 45-degree angle. At this surgical position, the peri-geniculate ganglion is located at the lowest position, which results in convergence of surgical bleeding. Using the transmastoid approach, the intra-temporal facial nerve was decompressed from the proximal end of the labyrinthine segment to the stylomastoid foramen. A posterior tympanotomy was made after mastoidectomy through a retroauricular incision. To obtain wide access to the geniculate ganglion and the tympanic segment, the incus was removed temporarily. By wide remove of the supralabyrinthine cells anterior to the bony superior semicircular canal, the geniculate ganglion and distal part of the labyrinthine segment of the facial nerve were exposed. The tegmen tympani above the geniculate ganglion should be removed by careful drilling. In order to avoid injury of the superior semicircular canal and dura of the temporal lobe, a bony defect of tegmen mastoideum with 10–15-mm diameter was created to seat the temporal lobe retractor from the peri-geniculate area to the lateral end of tegmen mastoideum.
Temporal lobe retraction after partial removal of the tegmen mastoideum provides a better surgical view from above and allows for widening of the fallopian canal containing the proximal labyrinthine segment by using a sharp instrument like a pic or curved small curettage, but not by drilling, for the prevention of neural injury. For the widening of meatal foramen, sharp and small curettage could be used very effectively for removal of the pneumatized temporal bone with sheet-like fallopian canal.
Next, an half of the bony facial canal was uncapped from the distal part of the labyrinthine segment of the facial nerve to the stylomastoid foramen. A longitudinal incision was made into the sheath of the facial nerve to decompress the nerve with sharp sickle knife. The nerve was protected by pieces of gel foam soaked in dexamethasone solution. Then, the incus was precisely replaced to its original position and both the incudostapedial and incudomalleolar joints were connected with fibrin glue.
This retrospective study was approved by the Institutional Review Board (ISPAIK 2015-10-005-001).
Statistical analysis
Improvement of the facial function is showed by comparing the HB grade. Results for the hearing are presented as mean±standard deviation. In addition, a paired t-test was performed to compare the degree of hearing loss after surgery. A p values <0.05 were considered to be statistically significant. Data analysis was performed using the SPSS 21.0 software package (SPSS Inc., Chicago, IL, USA).
RESULTS
Compared to contracted mastoid induced by ear disease, well-pneumatized mastoid that had been free from any otologic diseases had made to access easily and expose widely on peri-geniculate ganglion via temporal lobe retraction. Retraction of temporal lobe provided superior view on labyrinthine segment behind superior semicircular canal which could not be seen via transmastoid view (Fig. 1). Intraoperative pathology of the facial nerve was as follows: the integrity of the nerve was not interrupted as seen during surgery. Hematoma, multiple bone chips compression, granulation tissue, and edema were the main findings. In most of cases, this surgical approach made possible to access from labyrinthine segment to tympanic segment. Through the comparison of pre and post-operative temporal bone CT, a sufficient decompression to the labyrin-thine segment and geniculate ganglion was confirmed (Fig. 2).
Postsurgery, facial function recovered to HB grade I in 9 patients and to grade II in 11 patients (Table 2). After the surgery, 3 patients complained of decreased hearing and 2 patients had newly developed tinnitus and ear fullness due to ossicular reconstruction.
However, post-operative patients hearing was not statisti-cally different, even though it looks a little worse. In traumatic facial paralysis patients, pre and postoperative patients hearing was not statistically different (air conduction: 51.26±15.94 dB vs. 51.06±20.21 dB; p=0.210, bone conduction: 32.06±16.69 dB vs. 34.40±14.38 dB; p=0.052). In addition, perioperative hearing was not statistically different in patients with Bell's palsy and herpes zoster oticus (perioperative air conduction in Bell's palsy: 12.00±2.82 dB vs. 19.00±8.48 dB; p=0.10, bone conduction: 10.33±2.51 dB vs. 15.33±3.78 dB; p=0.082, perioperative air conduction in herpes zoster oticus: 24.50±7.77 dB vs. 33.50±2.12 dB; p=0.260, bone conduction: 22.50±7.77 dB vs. 21.00±7.07 dB; p=0.20) (Table 3).
No complications related to surgical retraction of the temporal lobe were noted. In all cases, we could achieve a wider surgical view of the peri-geniculate ganglion than that achieved by using the standard transmastoid approach.
DISCUSSION
Although the best method for surgical decompression of the facial nerve has been debated over a long time, surgery remains a preferred method for treating complete facial paralysis of acute onset resulting from any causes. In 1974, Fisch3 proposed the middle cranial fossa approach for nerve decompression because the narrowest portion of the fallopian canal is the meatal foramen, located at the fundus of the internal auditory canal, which is at the beginning of the proximal labyrinthine segment of the facial nerve. This most narrow portion of the fallopian canal forms a "bottle neck," and its surgical release of narrowest canal is crucial for adequate middle cranial fossa decompression. It was considered to be impossible to expose the meatal foramen via a transmastoid approach.56
To avoid craniotomy and its associated risks, new approaches without craniotomy have been introduced, such as the zygomatic root approach proposed by Ulug9 and the superior pre-labyrinthine cell tract approach of Takeda, et al.10 These surgical techniques are thought to be good alternatives and as effective as the middle cranial fossa approach to expose around geniculate ganglion by transmastoid approach which had been familiar to neuro-otologic surgeons.
However, as encountered excessive bleeding around the geniculate ganglion due to rich blood supply from the labyrinthine artery which is derived from middle meningeal artery, it is somewhat difficult for neuro-otologic surgeons to effectively create surgical exposure around the geniculate ganglion and handle critical point to be decompressed.
Excessive bleeding around the geniculate ganglion can occur especially in case of traumatic facial paralysis. Destruction of the microcirculation around the geniculate ganglion by linear temporal bone fracture and newly developed arterioles formed to compensate for breakage can make it difficult to expose the deepest point of facial nerve more than non-traumatic temporal bone. To compensate, we created a wider surgical exposure around the geniculate ganglion to provide a wider fallopian canal to allow delicate handling of the compressed facial nerve than previously proposed surgical approaches. Especially in traumatic facial paralysis, the decompressed facial nerve segment could be tympanic segment or geniculate ganglion in most cases, but it is very important to follow up to the normalized neural fascicle in decompression of swollen facial nerve. Therefore, we always had checked the labyrinthine segment for the confirmation of normal fascicle of facial nerve in order to obtain the effective surgical gain.
Many studies have reported anatomic variations of the intratemporal facial canal related to adjacent structures, especially from the labyrinthine segment to the tympanic segment.81112 The length of the labyrinthine segment is different for each person, and its length is about 3.14 mm to 5.27 mm.13 The labyrinthine segment is the most narrow region in the facial canal and it extends from the anterosuperior region of the fundus to the geniculate ganglion. To reach the geniculate fossa, it passes between the ampulla of the superior semicircular canal and the cochlea and travels forward and downward; it passes close to the dura of the temporal lobe. As mentioned by other authors, surgical exposure via transmastoid approach has the limitation that the distal labyrinthine segment is hidden behind the superior semi-circular canal. To access the proximal labyrinthine segment of the facial nerve, an additional procedure is required when using the transmastoid approach. Temporal lobe retraction after partial removal of the tegmen mastoideum provides a better surgical view from above and allows for widening of the fallopian canal containing the proximal labyrinthine segment by using a sharp instrument like a pic or small curettage, but not by drilling. Retraction of the temporal lobe and partial removal of the mastoid tegmen do not induce any neurological or olotogical problems.
There are no statistical differences in hearing change caused by surgery. However, it is a known fact that postoperative hearing was worse in some patients. However, in one stage ossiculoplasty, we could not expect effective hearing gain even after incus interposition due to post-operative middle ear shrinkage. In these cases, we should examine the middle ear for the better hearing gain after several months, and we could use any commercial partial ossicular replacement prosthesis or revision incus interposition.
Although the additional procedure of temporal lobe retraction creates a wider surgical field, there could be complications as retraction itself may stress the temporal lobe. Mechanical damage and iatrogenic compressive injury on the temporal lobe might lead to temporal lobe epilepsy, brain hematoma, or brain herniation.
In this study, all patients had healthy pneumatic temporal bone without any sclerotic or inflammatory change after surgery. However, if a patient has chronic otitis media with atrophic and sclerotic change in the mastoid cavity, the transmastoid approach using temporal lobe retraction could be limited in providing enough surgical view of the peri-geniculate ganglion.
We propose this surgical approach because of wide surgical view, short operation time, and familiarity to neuro-otological surgeon compared to other surgical technique. This surgical approach could be useful for facial nerve decompression without the need for a fatal craniotomy for treating severe facial paralysis.
In conclusion, facial nerve decompression via the transmastoid approach with temporal lobe retraction provides effective exposure of the key areas around the geniculate ganglion without any complications. As this is a relatively simple procedure and familiar to an experienced neuro-otologic surgeon, it can be used to achieve a better surgical view on the critical and limited labyrinthine segment of the facial nerve.




 XML Download
XML Download