

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Malignant melanoma is less common than non-melanoma skin cancer, but its incidence has increased substantially over the past two decades.1 However, it accounts for the majority of mortality associated with skin cancer.2 Even though primary tumor excision is the choice of treatment, melanomas are occasionally beyond surgical margins when diagnosed, and are usually resistant to chemotherapy and radiotherapy.3 Therefore many other therapeutic modalities are being investigated, and one of them is a dendritic cell (DC)-based cancer vaccine. In 1996, the DC-based vaccine was first introduced to treat B-cell lymphoma.4 Further clinical trials of the DC vaccination have been performed for treatment of melanoma, colorectal carcinoma, lung carcinoma, renal cancer, prostatic cancer, and multiple myeloma.5 However, the DC vaccination for malignant melanoma is still in its early phases in South Korea. Here, we report the results of a clinical trial with six Korean patients with advanced malignant melanoma who were treated with vaccination with mature, monocyte-derived DCs.
MATERIALS AND METHODS
Study design and eligibility criteria
The study was designed as an investigator-initiated clinical study to evaluate the safety and effectiveness of autologous monocyte-derived DC vaccination for malignant melanoma. Five patients had stage IV melanoma and one patient had stage II melanoma according to the AJCC staging system (Fig. 1). The eligibility criteria stated that patients were required to have histologically proven metastatic melano991ma, ECOG performance status 0 or 1, sufficient tumor tissue (more than 2 gm) for tumor antigen, available monocyte for DC culture, and lack of benefit from conventional cancer treatments such as well-established chemotherapy, radiotherapy and surgical operations. The exclusion criteria stated that patients could not have any other severe medical conditions or psychiatric diseases that would contraindicate study participation. Previous treatment with chemotherapy, cytokines, or active immunotherapy including systemic corticosteroids within three months of the study was not allowed. The clinical study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patients before they began the study. Patients were enrolled from May 2006 to March 2008 at the Yonsei Cell Therapy Center of Severance Hospital, Yonsei University Health System, Seoul, Korea. The study protocol was approved by the Institutional Review Board of Yonsei University Health System's Clinical Trial Center and by the Korea Food & Drug Administration.
Preparation of monocyte-derived DC
For the preparation of monocyte-derived DC, we referred to the previous publication of our group.6 Peripheral blood mononuclear cells (PBMCs) were isolated from leukapheresis products using a commercially available apheresis system (COBE Spectra, Lakewood, CO, USA). In brief, the leukapheresis product was loaded via the inlet pump into the constantly rotating (2,400 rpm) elutriation chamber. The automation mode produced five elutriation fractions, each specified by centrifuge speed, loading or elutriation buffer flow rate, and process volume. The final monocyte-rich fraction (Fraction 5) was collected from the chamber into the final collection bag when the centrifuge was stopped. All procedures were conducted according to the manufacturer's recommendations, except that we used Hanks' buffered salt solution (HBSS; Bio-Whittaker, East Rutherford, NJ, USA) as an elutriation buffer. Enriched monocytes were cultured on T75 culture flasks (Greiner Bio-One GmbH, Monroe, NC, USA) in X-VIVO 15 (Bio-Whittaker), 20 µg/mL gentamicin, 2 mM glutamine, 5% heat-inactivated AB human plasma, 250 ng/mL recombinant human (rHu) GM-CSF (Leucogen, Singapore), and 20 ng/mL rHu IL-4 (Pharmingen, San Diego, CA, USA). Cultures were fed every other day by removing half of the supernatant and adding fresh medium with full doses of cytokines. On day 6, immature DC (iDC) were generated and harvested for tumor antigen loading. Several other papers give more detailed information on monocyte enrichment and DC identification using surface markers.6,7
Preparation of tumor lysate-pulsed mature DC for vaccination
Tumor lysate was prepared using freezing/thawing techniques previously described by Nakai, et al.8 In brief, tumor specimens were immediately placed in phosphate-buffered saline (PBS). Subsequently, adjacent normal tissue was removed using a scalpel, and tumor cells were dispersed to create a single-cell suspension. The cells were lysed by four to five freeze cycles (on liquid nitrogen) and thaw cycles (room temperature). The larger particles were removed by centrifugation (10 min, 400 g). The supernatants were passed through a 0.22-µm filter, protein concentration was determined and aliquots were stored at -80℃ until use. To induce maturation, immature DCs were cultured for 48 hours in medium containing 100 µg/mL of autologous tumor lysate, keyhole limpet hemocyanin (KLH), cytokine cocktail (20 ng/mL TNF-α, 500 U/mL IL-1β, 500 U/mL IL-6 (all from Pharmingen), and 10-7 mol/L PGE2 (Sigma Chemical Co., St. Louis, MO, USA). After 48 hours, the cells were harvested and analyzed. Before injection, we performed endotoxin and mycoplasma tests with supernatants. Endotoxin and mycoplasma tests were performed using a kinetic method at the Celltec Bio-research Center (Bucheon, Korea). Sterility tests were performed at our own facility by members of the Department of Laboratory Medicine.
Vaccination protocol
Patients received subcutaneous injections of 2-4×107 cells of tumor-lysate-pulsed DC into the groin, axilla and neck at two week intervals. Each patient was assigned to receive four DC vaccinations. Complete response was defined as the disappearance of all targeted lesions. Partial response (PR) was defined as a decrease of at least 30% in the sum of the longest diameter (LD) of the target lesions, with the baseline sum LD as a reference. Progression of disease (PD) was defined as an increase of at least 20% in the sum of the LD sum value recorded at the start of treatment. Stable disease (SD) was defined as neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD, with the smallest sum LD as a reference.
Clinical outcome assessment
The patients were evaluated for toxicity and clinical response after undergoing four vaccinations. Clinical outcome was evaluated based on the analysis of whole body PET-CT images before and after the fourth vaccination.
Delayed type hypersensitivity response (DTH)
DTH was examined before and after each vaccination. Patients received intradermal injections of 100 uL of normal saline, tumor lysate 100 ug, KLH 50 ug and tumor antigen 100 ug plus KLH 50 ug at different sites on the forearm. The concentration of tumor antigen was 100 µg/mL and of KLH was 50 µg/mL. Forty-eight hours later, DTH was scored positive if the areas of erythema and induration were greater than 5 mm.
Flow cytometry analysis
To assure the characters of immature and mature DC, the surface molecules were identified using flow cytometry analysis. In brief, the cells were washed with 0.4% BSA/PBS and stained for 30 minutes at 4℃ with monoclonal antibodies conjugated to fluorochromes against CD1a, CD3, CD4, CD8, CD14, CD16, CD19, CD45, CD56, CD80, CD83, CD86, HLA-ABC and HLA-DR (all from Pharmingen). After two washes with 0.4% BSA/PBS, flow cytometric analysis was performed by FACSCalibur (BD Biosciences, Franklin Lakes, NJ, USA).
Interferon-γ enzyme-linked immunosorbent spot (IFN-γ ELISPOT) assay
PBMC (5×105 cells/well) were added to plates pre-coated with 5 µg/mL of a primary anti-IFN-γ monoclonal antibody (BD Biosiences) in the presence of 10 µg/mL tumor lysate as an antigen and incubated for 48 hours. The negative controls for the assay were unstimulated PBMCs. A positive response was arbitrarily defined as at least a two-fold increase in antigen-specific IFN-γ ELISPOT and at least 10 spots/5×105 PBMC at any time point post-DC vaccination.
Enzyme-linked immunosorbent assay (ELISA)
To measure IL-10, IL-12p70, IFN-γ and TGF-β in the peripheral blood, ELISA was performed before first vaccination and after the fourth vaccination. Quantities of IL-10, IL-12p70, IFN-γ and TGF-β were measured by using OptEIA (BD OptEIA human ELISA kit; BD Bioscience) as described by the manufacturer.
RESULTS
Patients
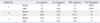
This clinical trial was conducted on six patients with advanced malignant melanoma. Table 1 shows the patient characteristics at the time of study entry. Their mean age was 58 years (range: 39-81 years). There were four males and two females. Five patients had stage IV disease and one patient had stage II disease. The site of the primary tumor varied. Three patients had primary acral lentiginous melanoma, which is the most common type of malignant melanoma in Asians. The others had primary tumors on the posterior neck skin, small intestines and tonsils. All patients had received surgery, two patients had received prior chemotherapy, and one patient received prior radiofrequency ablation for metastatic liver disease. Although patient 2 had stage II disease, recurrent tumors in the oral cavity were neither operable nor responsive to chemotherapy.
Therapeutic-DC characteristics
We performed leukapheresis on six melanoma patients and obtained DCs of acceptable quality and quantity for vaccination (Table 2). The average recovery of mononuclear cells and monocytes after leukapheresis were 7.9±5.5×109, 1.9±1.0×109 respectively. After elutriation, average monocyte recovery and monocyte fraction purity were 1.2±1.0×109, 49.9±30.2%. For each vaccination, iDCs were generated from a frozen aliquot of enriched monocytes in the presence of rh GM-CSF, rh IL-4 and 5% heat-inactivated AB human plasma (Fig. 2A). Since autologous plasma from melanoma patients can have a negative influence, we used heat-inactivated AB fresh frozen plasma stored for transfusion, making it not a single lot. We had to use AB plasma from different donors for each injection. On day 6, iDCs obtained were CD80-, CD83-, CD86low+, HLA-DR+ (Fig. 2B). They were co-cultured for 48 hours with autologous tumor lysate, KLH, TNF-α, IL-1β, IL-6 and PGE2. CD80+, CD83+, CD86high+, HLA-DR+ mature DC (mDC) were obtained (Fig. 2C). There was no endotoxin, mycoplasma, or bacterial contamination in the media of the cultured DCs.
Safety
Overall, the vaccine was well-tolerated. Only two patients (patient 2, 3) reported minor flu-like symptoms (grade I). However these symptoms did not lead to early withdrawal from the study. No clinical signs of autoimmune reactions about melanocytes, such as vitiligo and halo nevus, were detected. In all patients, blood tests revealed no treatment-related hematologic, renal or hepatic toxicity.
Clinical responses in vaccinated patients
Of the six enrolled patients, two of them (patients 1, 6) withdrew from the study due to rapidly progressive disease (Table 2). In the cases of patients 3, 4 and 5, reduction of tumor volume was noted on the PET-CT (reviewed by Nuclear Medicine professor, J.D.L.). Improvement was found in the lymph nodes at the left supraclavicular fossa, bilateral retroperitoneal area, right inguinal area and right axilla after the fourth vaccination in patient 3 (Fig. 3). Patient 4 showed improvement in the extrahepatic lymph nodes inferior to liver. In case of patient 5, intensity on PET-CT decreased in the right upper paratracheal lymph nodes, right femur, L4 spine, left distal humerus and left inguinal lymph nodes. Due to rapid disease progression, post treatment PET-CT was not performed in patient 1. After three vaccinations, patient 6 showed no difference in PET-CT. Tumor volume increased in patient 2. In spite of tumor volume reduction in patients 3, 4 and 5, every patient experienced disease progression eventually. Patient 6 was lost during follow up. The other five patients expired within a year of their last vaccination. The mean survival period was 4.6 months for these five patients.
Immune responses
DTH was examined for antigen-specific immunity. DTH reactions were measured before and after each vaccination. None of the patients had positive pre-vaccination DTH reactions. Patient 1 was unable to receive the DTH test due to rapid disease progression. Post-vaccination DTH test revealed vaccination-induced tumor antigen-specific reactivity in the other five patients (Fig. 4). Since some patients quit the clinical trial or expired during the study, we lacked specimens for the assays. Therefore, IFN-γ ELISPOT assay was performed only in patients 2 and 3 (Table 2). ELISPOT assay detected an increase in antigen-specific IFN-γ producing PBMCs in both of these patients (Fig. 5). In patient 3, antigen-specific IFN-γ producing PBMCs increased more than five times after vaccination. Cytokine levels in peripheral blood were measured with ELISA for IL-4, IL-12, IFN-γ and TGF-β before and after the fourth vaccination (Table 3). Only patients 3, 4 and 5 had completed ELISA before and after vaccination. In patient 3, IL-12 increased after vaccination. However, TGF-β also increased. In patients 4 and 5, IFN-γ and IL-12 increased after vaccination.
DISCUSSION
Here, we performed DC vaccinations in six patients with malignant melanoma. In this study, DC vaccination using tumor-antigen loaded DCs led to tumor volume regression in three of the six patients, which was evaluated by PET-CT. DTH responses were positive in five patients. IFN-γ producing PBMCs were detected in two patients by ELISPOT assay. However, rapid disease progression was seen in almost all patients. Since none of the patient survived more than a year after the last vaccination, according to our results, we consider our DC immunotherapy method to be insufficient as a single treatment modality for malignant melanoma with distant metastasis. Nevertheless, positive DTH and tumor volume reduction on the PET-CT showed the possibility of utilizing DC vaccination as an adjuvant therapy.
The patient in case 3 showed noticeable tumor volume reduction within just three months. The size of the lymph nodes at the left supraclavicular fossa, bilateral retroperitoneal area, right inguinal area and right axilla was markedly reduced after the fourth vaccination according to the PET-CT. Because patient 3 was in his thirties, good clinical responses were expected. He also had positive DTH response, increased antigen-specific IFN-γ producing PBMCs on the ELISPOT assay and increase in IFN-γ as well as TGF-β in the peripheral blood. However, the patient expired one month after the fourth vaccination. This outcome may have been partially related to TGF-β expressing T cells. A recent study indicates that the survival of DC-vaccinated malignant melanoma patient is correlated with the reduction of TGF-β expressing T cells.9 Regulatory T cells (Tregs) are a subpopulation of T cells that constitutively express high levels of CD25.10 Tumor antigen-specific Tregs are known to play an immune suppressive role to the antigen. Liyanage, et al.11 showed that the prevalence of tumor antigen-specific Tregs is higher in patients with advanced tumor disease. A high number of tumor antigen-specific Tregs has also been shown to be related to reduced survival.12 In addition, Tregs are able to induce tolerogenic DC, thereby developing anergic and immunosuppressive T cells.13 Dannull, et al.14 have shown that depleting Tregs enhances the efficiency of DC vaccines in renal cell carcinoma. Considering these results, there is a possibility that melanoma antigen-specific Tregs affected the survival of our patients too, especially patient 3. In a study performed in patients with distant malignant melanoma, intravenous administration of DAB389IL-2 (ONTAK) resulted in a significant decrease in the total number of Tregs. Furthermore, immunization of the same patients with the tumor antigen peptides led to an increase in tumor antigen-specific CD8+ T cells.15 In addition, Rasku, et al.16 reported regression of melanoma metastases after depleting Tregs with ONTAK. Five of sixteen patients experienced partial or near complete regression of melanoma metastases as measured by CT and/or PET imaging. On the contrary, Attia, et al.17 reported that administration of ONTAK does not appear to eliminate Tregs or cause regression of metastatic melanoma. These conflicting results may be due to the difference in duration of ONTAK treatment, but this needs further investigation. To date, there have been no clinical trials of DC-related immunotherapy after depleting Tregs in advanced melanoma patients. Since half of the patients in our study experienced regression of metastatic melanoma by tumor antigen-specific DC vaccine, we think it is possible to obtain better clinical outcomes if Tregs depletion is combined with DC vaccine.
There are many factors other than Tregs depletion to be evaluated and determined in each step of DC-based vaccination in order to standardize and optimize this vaccination treatment.18 Other factors include the source of DC, maturation status of DC, maturation of cocktails, type of antigen, helper antigens, routes of administration, frequency of injections and numbers of injected DCs. Current understandings of these factors have been thoroughly reviewed by Eubel and Enk.7
A large tumor burden impairs the general host immune system and host immune anergy seems to develop commonly in patients with advanced disease.19 Patients with less advanced disease show strong and durable immune responses after DC vaccinations.20 Tumor evasion of the host immune response is another important factor that should be considered in DC vaccination. There are several mechanisms orchestrated by the tumor to escape from the host immune system. In short, these mechanisms include interference with the induction of anti-tumor immune response, inadequate effector cell function in the tumor microenvironment, insufficient recognition signals and development of immunoresistance by the tumor.21 As advanced disease impairs the host immune system and promotes tumor immune evasion, DC vaccination would be more efficient if performed in less advanced disease.
In this study, DC vaccination using tumor antigen loaded with mature, monocyte-derived DC led to tumor regression in individual melanoma patients. However, there was a huge discrepancy between the strong antigen-specific T cell responses ex vivo and the weak clinical responses. Despite this, positive DTH responses and tumor volume reduction on PET-CT showed the possibility of utilizing DC immunotherapy as an adjuvant therapy. As mentioned in the discussion, it would be much more effective if DC vaccines were used as an adjuvant therapy in less advanced melanoma patients after depleting Tregs. Further clinical trials should be conducted in patients with less advanced disease with the elimination of Tregs. In addition, standardized treatment methods are lacking due to the high cost of clinical studies and the associated ethical issues. Hence, clinical studies of numerous patients of melanoma are needed from multiple institutions to determine the ideal parameters for DC immunotherapy in every aspect.







 XML Download
XML Download