

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Insulin resistance is the main pathologic mechanism of type 2 diabetes mellitus and cardiovascular disease.1-3 For evaluation of insulin sensitivity, the euglycemic hyperinsulinemic clamp is the gold standard method in both animal and human.4 However, this technique is very difficult and complex and has been replaced by other simple and rapid methods such as the Homeostatic Model Assessment (HOMA) and the short insulin tolerance test (Kitt).5 Kitt was shown to have a close correlation with glucose clamp studies and could be suitable for estimating insulin sensitivity over a long period.6
Thiazolidinediones (TZDs) are a more recently discovered antidiabetic agents thought to increase peripheral glucose utilization or inhibit hepatic gluconeogenesis by binding the nuclear peroxisome proliferators-activated receptors gamma (PPAR-γ).7-9 The beneficial effects of TZDs on glycemic control by improving the insulin resistance in type 2 diabetic patients are already known, but no data are available to determine the effects of TZDs by Kitt.10,11
In this study, we investigated the insulin sensitizing effects of TZDs in Korean type 2 diabetic patients by using Kitt.
PATIENTS AND METHODS
Subjects
Eighty-three subjects (mean age = 57.87 ± 10.78) who visited the diabetes clinic at Wonju Christian Hospital, South Korea from January 2004 to December 2006 were enrolled. Patients with type 2 diabetes who were inadequately treated with sulfonylurea or metformin (glimepiride, 50/83; gliclazide, 15/83; metformin, 18/83) were included in this study. Patients daily received either 4 mg of rosiglitazone or 15 mg of pioglitazone in a single dose regimen (rosiglitazone, 60/83; pioglitazone, 23/83), and medication was not changed throughout the study. Mean follow-up duration was 25.39 ± 9.66 months.
Assessment of insulin resistance
Insulin resistance was evaluated by means of Kitt and HOMA-IR. Insulin resistance was determined in all subjects at baseline and after 2 years. Plasma glucose disposal rate (Kitt; %/min) was calculated as previously described6: Kitt was the ratio between 0.693 and t1/2, where t1/2 is the time necessary to reduce the basal glucose level by one half. The t1/2 value was calculated from the slope of least square analysis of the glycemic concentrations, starting at the 3rd minute until the 15th minute after intravenous regular insulin injection (0.1 U/kg). We set our definition of insulin resistant state as a Kitt value below 2.5%/min, according to a previous study.12 HOMA-IR was calculated using fasting serum insulin (pmol/L) and fasting plasma glucose (mmol/L; fasting insulin fasting glucose ÷ 22.5).13
Clinical and biochemical measurements
Height, weight, waist circumference, hip circumference, waist-hip ratio (WHR), and body mass index (BMI) were measured in all subjects. BMI was calculated as weight divided by height squared (kg/m2). Waist circumference was measured with soft tape at midway between the lowest rib and the iliac crest. The hip circumference was measured at the widest part of the gluteus region. The waist-to-hip ratio was then calculated. Systolic and diastolic blood pressure (SBP and DBP) was taken after 5 minutes rest and cessation of smoking by an automatic sphygmomanometer. Blood samples for fasting glucose, fasting insulin (RIA, Cobra II, Packard, MI, USA), HbA1C (high performance liquid chromatography, variant II, Bio-Rad, Richmond, CA, USA), total cholesterol (TBA-200FR, Hitachi 7170, Tokyo, Japan), triglyceride, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol were collected after more than 10 hours of overnight fasting.
Statistical analysis
Data are expressed as means ± standard deviations unless stated otherwise. We used the Student's t test to compare characteristics between men and women and the values between insulin resistance and insulin sensitive states, as defined by Kitt. Paired t-test was used to compare values obtained before and after TZDs administration. A chi-square test was performed to validate differences in insulin resistance when variables were stratified. Pearson's correlation coefficient was used to establish the association between Kitt and clinical and laboratory parameters of subjects. All analyses were performed using the Windows-based SPSS statistical package (ver. 12.0, Chicago, IL, USA), and p < 0.05 were considered significant.
RESULTS
Clinical and biochemical characteristics of subjects
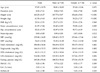
The main characteristics of study subjects are shown in Table 1. Male subjects were characterized by greater weight, waist circumference, waist-hip-ratio, and lower HDL cholesterol levels. Average BMI was 23.16 ± 2.51 kg/m2 (males 23.17 ± 2.51 kg/m2, females 23.14 ± 2.56 kg/m2), and waist circumference was 81.97 ± 7.04 cm (males 83.49 ± 6.90 cm, females 78.98 ± 6.43). Insulin sensitivity markers were not different between males and females.
Parameter changes
Subjects showed improved glycemic control after the addition of TZDs to their oral hypoglycemic drugs. As shown in Table 2, there were significant changes in fasting glucose (183.28 ± 55.04 mg/dL to 137.34 ± 36.4 mg/dL, p < 0.001) and HbA1C levels (9.24 ± 1.96% to 8.11 ± 1.39%, p < 0.001) after 2-year treatment with TZDs. Both body weight and BMI were significantly increased when compared with baseline values. Also, both waist and hip circumference increased significantly. No significant changes were observed in total cholesterol, LDL-cholesterol, and triglyceride levels. However, HDL-cholesterol levels significantly increased at 24 months when compared with baseline values (44.04 ± 11.17 mg/dL to 49.69 ± 14.97 mg/dL, p < 0.001; Table 2).
TZDs-induced improvement in insulin sensitivity measured by both Kitt and HOMA-IR was statistically significant (2.03 ± 1.14%/min to 2.67 ± 0.97%/min, p = 0.003 and 3.62 ± 2.98 to 1.61 ± 1.04, p = 0.012; Table 2). When the subjects were divided into insulin sensitive and resistant groups by baseline Kitt values, the changes of fasting glucose, HbA1C, and lipid profile were consistent with total subjects (Table 3). However, Kitt values were increased in insulin resistant subjects (1.51 ± 0.53%/min to 2.63 ± 0.88, p < 0.001) and decreased in insulin sensitive subjects (3.50 ± 0.75%/min to 2.75 ± 1.12%/min, p = 0.002; Table 3 and Fig. 1). In contrast, HOMA-IR was significantly decreased in both insulin resistance and sensitive subjects, defined by baseline Kitt values (Table 2).
DISCUSSION
It is well known that TZDs were efficacious in improving glycemic control and reducing HbA1C by insulin sensitizing action on muscle, adipose tissue, and liver.10,11,14-17 Our data showed that TZDs treatment improved insulin sensitivity approved by both Kitt and HOMA-IR methods in type 2 diabetic patients who had been inadequately treated with sulfonylurea or metformin.
It was reported that metformin or sulfonylurea combined with either pioglitazone or rosiglitazone significantly improve glycemic control.18,19 However, the combination of metformin or sulfonylurea with pioglitazone is associated with significant improvement in lipid and lipoprotein levels, whereas the rosiglitazone combination does not show a significant effect on lipid metabolism. In this study, we did not compare the effects between pioglitazone and rosiglitazone. However, fasting glucose and HbA1C levels were significantly improved, and lipid profiles except for HDL cholesterol levels were not changed after treatment with both pioglitazone and rosiglitazone compared with baseline values. We think that TZDs' effects on lipid metabolism should further be assessed in prospective trials.
Although several studies have provided strong evidence that TZDs may improve β-cell function,20-22 the major effects of TZDs are mediated via their insulin sensitizing effects on muscle and liver by binding to PPAR-γ.7,8,14-17 Previously, the insulin sensitizing effects of TZDs have been assessed by either euglycemic hyperinsulinemic clamp16,23-25 or HOMA index.18,19,26,27 Although the euglycemic hyperinsulinemic clamp is often referred to as the gold standard test, this technique is time-consuming and difficult to perform.28 Consequently, various simpler methods similar to the euglycemic hyperinsulinemic clamp method have been proposed in recent years. HOMA-IR is easily calculated from fasting glucose and insulin concentration, and relates closely with euglycemic hyperinsulinemic clamp.13,29 However, because insulin secretion is pulsatile and HOMA-IR is not a dynamic test, a single sample needs to be carefully interpreted.30 On the other hand, Kitt is a reproducible, inexpensive, and rapid method, allowing easy measurement of insulin sensitivity.5,6,31-33 In this study, we performed HOMA-IR and Kitt to estimate insulin sensitivity. As expected, both measurements for insulin sensitivity were improved after TZDs treatments. However, when we performed subgroup analysis with baseline Kitt values, Kitt values decreased in patients who showed Kitt values above 2.5%/min at baseline, while fasting glucose and HbA1C levels improved consistently in all subjects. HOMA-IR was equally improved regardless of baseline Kitt values. We could not exactly explain the reason of why Kitt values were not consistently changed by the treatment of TZDs. Nevertheless, we speculate various possibilities. First, Kitt may fail to estimate insulin sensitivity in insulin sensitive subjects. The amount of insulin used for Kitt (0.1 U/kg) is a supraphysiological dose and suppresses hepatic gluconeogenesis.31 After insulin injection during Kitt measurement, disappearance of glucose is mainly due to glucose uptake by muscles or adipose tissue. Consequently, Kitt may possibly underestimate the insulin sensitivity when patients have hepatic insulin resistance or show weak insulin resistance. In our study, insulin sensitivity may be improved in insulin sensitive subjects (Kitt > 2.5%/min) in a manner similar to insulin resistant subjects, although Kitt values did not change because of this reason. Second, TZDs may affect glycemic control in insulin sensitive subjects by an another mechanism rather than recovery of insulin resistance. It is well known that both beta cell function and insulin action are lessened in chronic hyperglycemic states34,35 and reversed by improved glycemic control.36,37 As mentioned above, since TZDs have an additional effect of preserving β-cell function,20-22 TZDs may improve the glycemic control by improving glucose toxicity even if Kitt values did not improve. Therefore, it is highly likely that the Kitt rate did not improve when the baseline was above 2.5%/min. However, it is highly desirable to perform clamp studies to clarify why Kitt is not consistently changed, and this is the limitation of the study.
In conclusion, Kitt could be a reliable method to estimate the insulin sensitizing effects of TZDs when Kitt values are less than 2.5%/min.



 XML Download
XML Download