

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Telomeres are repetitive structures of the sequence of bases (TTAGGG) that appear at the ends of mammalian chromosomes,1 and which contribute to the stability and function of chromosomes by preventing degradation and end-to-end fusion. Because of end replication problems, telomeres undergo attrition in groups of 20-200 base pairs for each cell division until the critical telomere length is reached. When the critical length is reached, cells eventually enter into replicative senescence.2,3 In humans, the telomere appears to be a major component of cell senescence and aging.4 Alteration of telomere biology is shown in genetic disorders or syndromes of accelerated aging.5-7 Telomere length is also associated with cardiovascular aging in males,8,9 the severity of Alzheimer's disease,10 and the mortality of elderly people older than 60 years.11
The rate of telomere attrition is modified by gender12 and oxidative stress.13 At birth, telomere length is the same in both men and women,14 but by adulthood telomeres are longer in women than in men.8,9 This discrepancy between genders is probably caused by the effects of estrogen. It has been suggested that estrogen can protect telomeres against reactive oxygen species (ROS) and induced DNA damage. Estrogen can also stimulate telomerase directly or indirectly by stimulating nitric oxide production.15,16 Based upon these observations, it is hypothesized that estrogen's positive effects on telomere attrition may affect postmenopausal women treated with long-term hormone therapy (HT).
The aim of this study was to investigate the influence of long-term HT on telomere attrition. The differences of telomere length in both postmenopausal women taking HT for more than five years and in postmenopausal women without a history of HT were compared to determine the effects of long-term HT.
MATERIALS AND METHODS
Study population
Study subjects were recruited using an advertisement from the health promotion center in a women's hospital in Seoul, South Korea. All subjects signed an informed consent form approved by the hospital's Ethical Committee.
Two groups of study subjects were created on the basis of hormone therapy history: the HT group and the age-matched, non-HT group. The HT group was defined as postmenopausal women ranging in age from 55 to 69 years old who had been taking estrogen (0.625 mg of conjugated equine estrogen or 2 mg of estradiol combined with progesterone) for more than five years. The non-HT group was defined as postmenopausal women ages 55 to 69 years old who had not taken hormone therapy after menopause.
Exclusion criteria were high blood pressure (mean systolic blood pressure ≥150 mmHg or mean diastolic blood pressure ≥95 mmHg after two consecutive measurements), high fasting blood glucose (>126 mg/dL), abnormal liver function test (AST >35 IU/L, or ALT >35 IU/L), and a medical history of hysterectomy or other illness (hypertension, diabetes mellitus, liver disease).
The questionnaire assessed the medical history of the study subjects, and included illness, age at menopause, duration of HT, and vitamin use, as well as lifestyles such as exercise, alcohol ingestion, and cigarette smoking. Vitamin use was defined as daily use of vitamin C, vitamin E, or a multivitamin. Jogging, walking, swimming, cycling, dancing or participating in alternate forms of exercise more than three times a week for at least 30 minutes defined the exercise criteria. Alcohol ingestion was defined as the ingestion of alcohol more than one time each week. Smoking was defined by current cigarette smoking. Sixty-five postmenopausal women having had HT and 65 age-matched postmenopausal women with no history of HT were eligible for participation in this study after assessing the inclusion and exclusion criteria. The mean duration of HT (± SD) was 8.4 ± 2.3 years.
Biochemical assays
Biochemical tests were performed on blood samples collected after more than 12 hours of fasting. Venous blood was drawn and centrifuged, and then the serum was immediately frozen in a refrigerator at -80℃. Serum levels of blood glucose, high-sensitivity C-reactive protein (hs-CRP), total cholesterol, HDL-cholesterol, and triglycerides were assayed by enzymatic techniques (Bayer, Tarrytown, NY, USA) using an auto-analyzer ADVIA 1650 (Bayer, Tarrytown, NY, USA). LDL-cholesterol was calculated using a Friedewald formular.17 Estradiol was assayed by electrochemiluminescence immunoassay using Elecsys 2010 (Roche, Indianapolis, IN, USA). Plasma total antioxidant status (TAS) was measured using a kit supplied by Randox Laboratories (Diamond, Crumlin, UK) following the methods previously described by Re et al.18
Quantitative PCR
Relative ratios of telomere repeat copy number to single copy gene number (T/S ratio) in study subjects was compared with a reference DNA obtained from a healthy young female genes were measured by quantitative PCR as previously described by Cawthon,19 but with the newly revised primer set designed by Cawthon. This new primer set, which has equal Guanine and Cytosine (GC) content and a higher annealing temperature than other published primers, shows improved correlation with the relative mean terminal restriction fragment(TRF) lengths (r2=0.971 vs 0.794, unpublished data by Cawthon RM). This study used β-globin as a single copy gene because it enhanced PCR efficiency and reproducibility better than 36B4 did.
Whole blood samples were collected by venipuncture and stored in EDTA-containing tubes. Genomic DNA was extracted from white blood cells by phenol/chloroform extraction using a standard protocol. All DNA samples were diluted to the same concentration (based on absorbance) and stored at -80℃ until time of use.
Real time PCR was performed using a Light Cycler (Roche, Mannheim, Germany). The rate of accumulation of amplified DNA was measured by continuous monitoring of SYBR Green I (Molecular Probes, Eugene, Oregon, USA) as fluorescent dye. Quantitative values were obtained from the threshold cycle value (CT) at which a signal increase associated with exponential growth of PCR products was detected using Light Cycler analysis software. Twelve microliters of the genomic DNA were used to obtain the quantitative PCR in a final volume of 20 µL. The concentrations of reagents for telomere PCRs were 20 mM Tris-HCl pH 8.4, 50 mM KCl, 200µM each dNTP, 1% DMSO, 2.5 mM DTT, 0.4×SYBR Green I, 0.08 U Platinum Taq Polymerase (Invitrogen, Carlsbad, California, USA), 1.5 mM MgCl2, and 300 nM of each telomere primer. The concentrations of reagents for β-globin PCRs were 20 mM Tris-HCl pH 8.4, 50 mM KCl, 200 µM each dNTP, 1% DMSO, 2.5 mM DTT, 0.4×SYBR Green I, 0.05 U Platinum Taq Polymerase, 3.5 mM MgCl2, 300 nM β-globin primer 1, and 500 nM β-globin primer 2.
Telomere primer sequences were 5'-CGGTTTGTTTGGGTTTGGGTTTGGGTTT-GGGTTTGGGTT-3' and 5'-GGCTTGCCTTACCCTTACCCTTACCCTTACCCTTA-CCCT-3'. β-globin primer sequences were 5'-GCTTCTGACACAACTGTGTTCACTAGC-3' and 5'-CACCAACTTCATCCACGTTCACC-3'. The thermal cycling conditions for both amplicons began with two-minute incubation at 94℃ to activate the Platinum Taq DNA polymerase and denature the DNA. For telomere PCRs, 30 cycles were conducted for 15 sec at 95℃ and for one minute at 56℃. Thirty-five cycles of 15 sec at 95℃, 20 sec at 56℃, and 20 sec at 72℃ were conducted for β-globin PCR. At the end of the amplification cycles, a melting temperature analysis was performed using a slow increase in temperature (0.1℃/sec, up to 95℃). Each sample was analyzed using duplicates, and mean values were used for the study.
For the inter-assay coefficient of variation (CV), nine DNA samples with the same concentration were tested on three different days: inter-assay CV for telomere and β-globin PCR were 1.5 ± 0.7% and 1.3 ± 0.9%, respectively. Nine different allocations for intra-assay CV were tested in triplicate with one DNA sample in the same plate: intraassay CV for telomere and β-globin PCR were 1.0 ± 0.7% and 1.0 ± 1.1%, respectively.
Calculation of relative T/ S ratio
In order to reduce the inter-assay variation, the same number of HT and non HT DNA were allocated with reference DNA in each plate. Then the CT values of both telomere and β-globin were measured using quantitative PCR in each plate, and the T/S ratio and relative T/S ratio were calculated as follows:
Total amount of telomere in a DNA sample=2-CT (telomere)
Total amount of β globulin in a DNA sample=2-CT (β-globin)
T/S ratio in a DNA sample={2 CT (telomere)/2CT (β-globin)}-1=2-Δ CT
The relative T/S ratio is the T/S ratio of one sample relative to the T/S ratio of a reference gene from a healthy young female, and this ratio was calculated as follows:
Relative T/S ratio of study subjects={2Δ CT (telomere)/2Δ CT (reference gene)}-1=2-ΔΔCT.
Mean value of Δ CT for a reference gene was 12.73 ± 0.50.
Agarose gel electrophoresis of the telomere PCR product
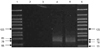
After 30 cycles of telomere PCR, each 20 µL of the amplified product was analyzed by electrophoresis using 4% metaphor agarose gels running for one hr at 50 V in 45 mM tris borate and one mM EDTA with ethidium bromide. Gels were visualized under ultra-violet (UV) illumination. The PCR products were observed as a smear beginning with great intensity at 78 bp, which was the shortest possible product size, and progressively fading to background with larger products. This has been previously described by Cawthon19 (Fig. 1).
Statistical analysis
Data are expressed as means ± SD. Clinical characteristics were compared between the HT and the non-HT groups using t-tests for the continuous variables and Pearson chi-squares (χ2) for the categorical variables. CT value differences were compared between the HT and the non-HT groups using t-tests. Relative T/S ratios were compared between the two groups using the Wilcoxon rank sum test because the distributions were skewed. Multivariate linear regression analyses were performed to determine the association of HT and log2 values of relative T/S ratios (ΔΔCT) after adjusting for potential confounding factors. All data were analyzed using the statistical program SAS 8.01 (SAS Institute, Cary, NC, USA).
RESULTS
Clinical characteristics of study subjects
Clinical characteristics are shown in Table 1. Mean ages of the study subjects were 60.1 ± 3.5 years for the HT group and 60.3 ± 4.4 years for the non-HT group with no statistical difference. No statistical differences were found between the two groups with regards to age, age at menopause, blood pressure, cholesterol, triglyceride, LDL-cholesterol, TAS, and hs-CRP levels. Serum fasting glucose levels were significantly higher in the non-HT group than in the HT group (p < 0.0001), but HDL-cholesterol levels were notably higher in the HT group than in the non-HT group (p < 0.001). Mean (± SD) serum estradiol levels of the HT group were 35.6 (± 35.5) pg/L, which were significantly higher than those in the non-HT group (p < 0.0001). Women who participated in regular exercise or took daily vitamins were better represented in the HT group (p < 0.01 and p < 0.01, respectively) than in the non-HT group.
Comparison of relative T/ S ratios
CT values of telomere PCR in the HT group were significantly lower than those in the non-HT group (p < 0.05). That is, the HT group had a greater amount of telomeres than the non-HT group because the total amount of telomeres in a DNA sample was approximately 2-CT (telomere). ΔCT values. were calculated by subtracting the β globulin (single copy gene) CT value from the telomere CT value, which was also significantly lower in the HT group than in the non-HT group (p<0.01)(Table 2). The HT group had greater T/S ratios than the non-HT group of postmenopausal women because the T/S ratio in a DNA sample was approximately {2CT (telomere)/2CT (β-globin)}-1= 2-Δ CT. Relative T/S ratios of study subjects to a reference (a healthy young female) were greater in the HT group than in the non-HT group (p < 0.01) (Table 3). In other words, telomere lengths were longer in the HT group than in the non-HT group of postmenopausal women.
Because serum fasting glucose levels, HDL cholesterol levels, and the prevalence of regular exercise and daily vitamin use statistically differed between the two groups, and also because several potential confounding factors known to be related to telomere length existed in this study, a multiple linear regression analysis was performed. This was done to determine the association of relative T/S ratios and long-term estrogen replacement after adjusting for potential confounding variables. Log2 values of study subjects' relative T/S ratios (ΔΔ CT) were used in the analysis to account for the skewed distribution. Adjusted regression coefficients for Log2 values of relative T/S ratios are described in Table 4. HT showed significant correlation with relative T/S ratios (β=0.56 SE=0.27 p<0.05), and no significant interaction was found between relative T/S ratios and the other variables.
DISCUSSION
In the present study, we demonstrated that telomere lengths were significantly higher in postmenopausal women who had undergone long-term hormone therapy than in women who had never taken estrogen after menopause. This result suggests that conventional doses of long-term hormone therapy after menopause might have the effect of attenuating telomere attrition. From a broader perspective, long-term hormone therapy may affect human health by influencing telomere biology in a manner that had not been previously explored. Recent reports have demonstrated the association between telomere length and age related diseases,3,8-10 as well as mortality in the elderly.11
There are several factors that regulate telomere attrition. Cellular replication is the principal regulator of telomere attrition due to the so-called end replication problem. Telomerase counteracts telomere erosion in this specific condition. Another important factor contributing to telomere shortening is the oxidative stress. Telomeres are highly sensitive to oxidative stress-mediated damage in vitro. In fact, the telomere shortening rate in human fibroblasts among different cultures varies by more than 1 - 2 orders of magnitude depending on the oxidative stress.20,21 The preferential accumulation of oxidative damage causes single-stranded breaks that result in telomere erosion by mechanisms that are independent of the end replication problem.21-23 Antioxidants aid in the attenuation of telomere shortening.3,24 Considering that estrogen and its derivatives are known to have antioxidant properties via diverse mechanisms,15 the antioxidant capacity of long-term HT might modify the influence of ROS on the telomere shortening rate.
However, we failed to find any significant differences in the serum total antioxidant status (TAS) level between the HT and the non-HT group. Also, there was no significant correlation between the TAS level and the relative T/S ratio. This result was irrelevant because estrogen is believed to influence telomere attrition primarily by its antioxidant effects. This discrepancy raised the possibility that serum levels of the total antioxidant capacity in one point in time might not necessarily indicate the oxidative damages of DNA in vivo. DNA damage is not only caused by oxidative stress but is itself regarded as the most sensitive biological marker for oxidative stress. Despite the status of high sensitivity, there are studies which demonstrate that there is no association between the percentage of DNA damage and serum levels of antioxidant capacity.25,26 Mendoza-Nunez26 proposed that low serum levels of total antioxidants are not always indicative of oxidative stress. Moreover, it would be complicated to measure the full spectrum of estrogen's antioxidant actions by conventional methods. This is because of the diverse mechanisms through which estrogen exerts an antioxidant effect,15 e.g., scavenging free radicals, inhibiting free radical formation and stimulating free radical enzymes.
In addition to its antioxidant effect, estrogen has been shown to stimulate telomerase in a vitro study.27 This mode of action is thought to be mediated by posttranscriptional modification through stimulation of the phosphoinositol 3-Kinase/Akt pathway.28,29 Estrogen can also influence telomerase activation by stimulating NO, which has been proven to activate telomerase in the endothelial cell line in recent vitro studies.30,31 Because serum estrogen levels in the HT group were significantly higher than in the non-HT group, we could hypothesize that telomerase activation aided in the alleviation of telomere attrition in the HT group. Further studies will be needed to confirm this hypothesis.
The traditional method for measuring telomere length in human DNA is to determine a mean TRF length by Southern blot analysis. However, this method is time consuming, requires a large amount of DNA, and shows variability depending upon the particular restriction enzyme used. However, measurement of the relative telomere length ratio by quantitative PCR is simple and allows for the rapid processing of large numbers of samples. In previous research, relative T/S ratios determined using quantitative PCR were found to correlate well with mean TRF lengths.11,19 Also, agarose gel electrophoresis demonstrated that the approximate size of major PCR products was 78 bp with new primer set, as was expected.
In this study, postmenopausal women having had HT were more prone to take vitamins and to exercise regularly, so they may have practiced better health habits than women in the non-HT group. Serum levels of fasting blood glucose and HDL-cholesterol were significantly different between the two groups. These factors might be a source of bias, but estrogen use still showed a significant correlation with the relative telomere length ratio in linear regression models after adjusting for these factors.
There are some limitations to this study. First, the retrospective nature of our study design does not permit us to confirm the effect of estrogen replacement on changes in telomere attrition. Prospective studies are needed to evaluate the role that estrogen therapy may have on the alleviation of telomere attrition. Also, because telomere length has been shown to vary considerably among individuals in previous studies, the small sample size in this study may not offset an enrolling bias.
In conclusion, telomere lengths were longer in postmenopausal women who had taken HT than in postmenopausal women without a history of HT. This suggests that long-term hormone therapy in postmenopausal women might have the effect of alleviating telomere attrition. Further studies are necessary to more clearly understand the relationship between hormone therapy and telomere attrition.




 XML Download
XML Download