

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Edema of the breast is characterized by an increased skin thickness and breast parenchymal density with prominent interstitial markings.1 It may co-occur with inflammatory breast carcinoma, lymphatic obstruction (due to axillary, chest wall or intrathoracic lesions), mastitis, fat necrosis, trauma, postirradiation changes, granulomatous diseases, nephrotic syndrome, lymphoma, progressive systemic sclerosis, leukemia, pemphigus and other skin conditions, subclavian or innominate vein occlusion, or congestive heart failure. Thus a knowledge of the etiologies of the entities that cause unilateral breast edema and their typical appearances can aid accurate diagnosis. Here, we describe a spectrum of etiologies and imaging appearances related to unilateral breast edema.
LESIONS RELATED TO MALIGNANCY
Inflammatory Breast Carcinoma
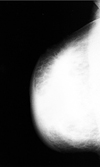
Inflammatory breast carcinoma is an unusual variant of locally advanced breast cancer. Inflammatory breast carcinoma of the breast accounts for 1 - 4% of breast cancers.2 Its clinical manifestations include a redness or purplish discoloration of at least one-third of the breast skin, peau d'orange, and a palpable ridge at the margin of induration. Mass, tenderness or pain, increased temperature of the involved breast, and breast enlargement are often present. Pathologically, any subtype of primary breast carcinoma may be present, but dermal lymphatic vessels must be involved3 and subepidermal capillaries and venules may also be occluded. Tumor involvement and obstruction of lymphatic vessels and capillaries result in mammographic findings of stromal coarsening, and the thickening of Cooper ligaments and the skin.4
The mammographic findings of inflammatory breast carcinoma are a mass, malignant-type calcifications, and skin changes4 (Fig. 1). Moreover, because inflammatory breast carcinoma has the nature of an advanced cancer, axillary lymphadenpathy is commonly present. Sometimes breast infection has similar mammographic findings, but without malignant microcalcifications. And thus, a careful evaluation of imaging findings and clinical history is needed, because the detection of malignant microcalcifications by mammography and axillary lymphadenopathy can be underestimated.5
Metastasis
Paulus et al. reported that metastasis to the breast may occur by two distinct routes, i.e., lymphatic or blood borne.6 Of these, lymphangitic metastasis to the breast usually occurs via transthoracic or cross-lymphatic metastasis from contralateral primary breast cancer.
Mammographic findings of lymphangitic metastasis are skin thickening, denser subcutaneous tissue with a thicker trabecular pattern, and denser and more irregular glandular stroma.6 Lymphangitic metastasis of the breast has clinical symptoms that are similar to inflammatory breast cancer, however, radiographically detected by mammography and US microcalcifications or masses are more frequent in lymphangitic metastasis than in inflammatory breast cancer. Thus cases of lymphangitic metastasis with mass formation7 are difficult to differentiate from inflammatory breast carcinoma.
The breast is a relatively uncommon hematogenous metastasis site from an extramammary malignancy. Melanoma and lymphomas are the most common sources of metastasis. According to a recent report,7 stomach cancer is the second most common cause of breast metastasis in South Korea, possibly because of the high incidence of stomach cancer. The most common radiographic appearance of metastasis is the presence of one or more round, discrete nodules without microcalcifications, although metastatic ovarian carcinoma is an exception in this report. In addition some have reported breast metastasis mimicking inflammatory breast carcinoma (Fig. 2).
Breast lymphoma
Malignant lymphoma can originate as a primary breast tumor, or it may involve the breast secondarily as part of a diffuse metastatic process. Primary malignant lymphomas of the breast comprise 0.05% to 0.53% of malignant breast tumors.10 Most reported cases of primary breast lymphoma have been of the non-Hodgkin's variety. Secondary involvement in patients with a history of malignant lymphoma is somewhat more common. Clinically breast lymphoma can occasionally present as a diffuse rapid breast enlargement in younger age groups, or as breast skin thickening due to lymphatic blockage by lymphoma resulting in retrograde edema.11
The mammographic findings of lymphoma are a solitary noncalcified mass, multiple masses, diffuse increased opacity with skin thickening (Fig. 3), and negative descriptive findings. Breast lymphomas lack the calcification and spiculated margin, features characteristic of breast carcinoma. By US they are often hypoechoic and may be almost anechoic.12 Because of their nonspecific appearance by radiographic examination, Paulus suggested that the only significant clue concerning the presence of lymphomatous disease in the breast, is the presence of bilateral axillary lymph node enlargement.6
The diagnosis of primary lymphoma of the breast requires pathologic evidence of the close apposition of a lymphomatous infiltrate and normal breast tissue in patients with neither a previous nor a concurrent lymphoma at another site. Ipsilateral axillary nodes are acceptable, provided that these lesions develop in parallel with tumors. Axillary node involvement in patients with lymphoma of the breast has been reported to occur in 30 - 40%.13 The prognosis of lymphoma of the breast appears to be similar to that of nodal lymphoma, given an equivalent stage and histology.14
BENIGN LESIONS
Mastitis
Most commonly, breast infection occurs in young women, especially in the lactating state. But sometimes, breast infection occurs in a reduced immune state, such as, in those with diabetes mellitus, ductectasia, or galactocele. Because the breast is filled with milk, it tends to be susceptible to bacterial infections. Common organisms are staphylococcus and streptococcus, though tuberculosis may sometimes be encountered.
The most common mammographic finding is an irregular mass, whereas diffuse breast edema is observed in only a minority of patients15 (Fig. 4). These findings overlap with those of inflammatory breast carcinoma. But, diffuse skin thickening and dense lymph nodes favor inflammatory breast carcinoma,15 and are rare in cases of breast infection, except when the breast infection is unusual.
Tuberculosis of the breast has variable findings, including a coarse parenchymal texture, skin thickening, nipple retraction, the absence of microcalcifications, and a cloudy breast density with a sinus tract and skin bulge.16 Moreover, later the affected breast becomes smaller that the unaffected breast (Fig. 5). Three forms of tuberculosis have been reported, namely, the nodular, disseminated and sclerosing forms.17 In the disseminated form, mammography shows diffuse edema. Tuberculosis of the breast is difficult to differentiate from advanced breast carcinoma. However, in cases of malignancy, microcalcifications, nodular or spiculated masses, and axillary lymphadenopathy are more common. Furthermore, in malignancy, the affected breast is often larger, which contrasts with the situation in tuberculosis of the breast.
If inflammatory signs are not improved by treatment, a biopsy is indicated to eliminate inflammatory breast carcinoma. Ultrasound may be a useful adjunct by delineating a hypoechoic irregularly shaped nodule or by demonstrating focal abnormal acoustic shadowing.
Congestive heart failure
Unilateral breast edema may be due to a tendency to lie on one side, causing dependent edema18 (Fig. 6), and the atrophic breasts of elderly women may be more susceptible. If changes are unilateral, the possibility of carcinoma is of particular concern since systemic diseases usually give rise to bilateral abnormalities. Pitting edema of the breast and the absence of a palpable breast mass are helpful for distinguishing between breast edema due to congestive heart failure and malignancy,19 and after treatment for heart failure the breast edema should resolve.
Postirradiation or Post-partial mastectomy state
Postoperative edema has been reported to occur in 41%, and to be related to the axillary staging procedure.20 The usual mammographic findings are skin thickening, coarsening of stroma, an increased breast density (Fig. 7), and later benign calcifications.21 Responses of tissue to lumpectomy and radiation, such as, breast edema and skin thickening, are most pronounced 6 to 12 months after treatment, and gradually resolve within 1 to 3 years.22 Histologically, architectural distortion, fibrosis, and atrophy develop in treated breasts to various extents. Moreover, the same breast may show several types of change, which are not necessarily related to the radiation dose. Although the definite pathophysiologies of postsurgical changes are not known, it has been suggested that they are caused by the interruption of lymphatic vessels and associated lymphostasis.
To differentiate post-operative edema from other causes of unilateral breast edema, knowledge of clinical history is important. However, when sequential mammograms reveal persistent or increased breast edema recurrent carcinoma should be considered.
Other benign causes
Mechanical problems such as obstruction due to lymph node enlargement, subclavian vein occlusion, and especially arteriovenous hemodialysis complications, may cause unilateral breast edema.23 In such cases, patient history and enlarged lymph nodes by ultrasonography are useful guidelines for differentiating them from other diseases which cause unilateral breast edema.






 XML Download
XML Download