

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Myocarditis is an acute or chronic inflammatory disease of the myocardium that can be caused by infectious pathogens such as viruses, bacteria, toxic fungi and Chlamydia, as well as by toxic and hyper-sensitivity reactions (1). The short-term prognosis for acute myocarditis is typically good, but dilated cardiomyopathy or sudden cardiac death can also occur (123). Several parameters, including clinical symptoms such as advanced New York Heart Association (NYHA) functional classes, certain viruses or immunohistologic signs of inflammation identified by endomyocardial biopsy (EMB), left ventricle (LV) function, and late gadolinium enhancement (LGE), are predictors of poor outcomes (456). Because EMB is invasive, has a complication rate of 6% and is not appropriate for all patients (7), cardiovascular magnetic resonance (CMR) can be an alternative tool for the prediction of poor outcomes. CMR is non-invasive and can assess LV size, function and LGE simultaneously.
Left ventricular myocardial systolic strain and deformation parameters are altered during early-stage pathogenesis, and can be measured with CMR (8910). Tagged-CMR, in which magnetization saturation bands arranged in a grid format are placed onto the myocardium, is an established method for the assessment of regional LV function. However, myocardial tagging has not been widely adopted due to the necessity for additional scans and complex, time-consuming post-processing of images (1112). Recently developed feature tracking software enables the measurement of myocardial strain using CMR cine images. The software tracks endocardial and epicardial borders across frames to quantify the LV wall motion during the cardiac cycle. CMR-derived feature tracking methods are vendor-independent and thus do not require additional sequences (13). Furthermore, feature tracking-derived measurements of circumference have acceptable inter-observer reproducibility, and feature tracking-derived myocardial strain can predict acute myocarditis with high sensitivity and specificity (914). However, there have been no reports on the prognostic value of CMR-derived myocardial strain measurements in acute myocarditis patients.
Therefore, the primary objective of this study was to evaluate the utility of CMR-derived myocardial strain measurements for the prediction of poor outcomes, defined as major adverse cardiac events (MACE) or incomplete LV functional recovery, in patients with acute myocarditis.
MATERIALS AND METHODS
Study Population
This retrospective study was approved by the Institutional Review Board of our hospitals. This study reviewed the database of 42 patients with suspected myocarditis who underwent CMR between August 2004 and March 2014 in Pusan National University Hospital or Pusan National University Yangsan Hospital. Based on previous descriptions of myocarditis (101516171819), acute myocarditis patients were included who presented with the following: 1) symptoms and signs suggestive of acute myocarditis, such as fever, viral prodrome, chest pain, dyspnea, palpitation, effort intolerance or presyncope, or syncope within 6 weeks of admission; 2) evidence of structural or functional abnormalities on echocardiography or CMR, or of myocardial injury indicated by elevated biomarkers (troponin I level > 0.1 ng/mL or creatine kinase MB [CK-MB] fraction > 6.2 ng/mL); and 3) no evidence of coronary artery disease observed on coronary angiography in patients older than 35 years. Patients with coronary artery disease (n = 3), chronic myocarditis (n = 1), and a patient who did not undergo coronary angiography (n = 1) were excluded. A total of 37 patients comprised the study population. Medical records were reviewed for clinical symptoms, demographic factors (age, sex, weight, and height), past history (hypertension, hypercholesterolemia, diabetes, smoking), electrocardiogram (ECG) findings, initial troponin I, brain natriuretic peptide and CK-MB levels, pathologic EMB results, CMR findings and beta-blocker medication status. Control study subjects were 10 normal individuals (mean age, 36.2 ± 10 years; 5 females) with no history of cardiovascular disease, unremarkable findings on physical examination, and a low probability of heart disease.
Cardiovascular Magnetic Resonance
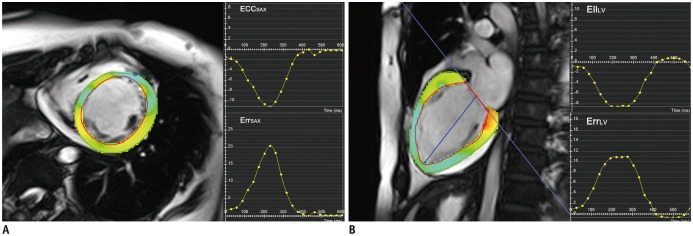
Cardiovascular magnetic resonance was performed using 1.5T (Magnetom Sonata, Siemens Healthcare, Berlin, Germany [12 patients]; Magnetom Avanto, Siemens Healthcare, Erlangen, Germany [16 patients]), and 3T (Achieva, Philips Healthcare, Best, the Netherlands [7 patients and 10 normal subjects]; Magnetom Skyra, Siemens Healthcare, Erlangen, Germany [2 patients]) CMR imaging scanners. All cine images were acquired using a balanced, steady-state, free precession sequence during a gentle expiratory breath-hold. Short-axis cine images from cardiac base to apex, and long-axis cine images in 2- and 4-chamber views were obtained using the following scan parameters: echo time (TE)/repetition time (TR)/flip-angle = 1.1 ms/54.8 ms/50°, slice thickness = 8 mm, gap = 2 mm, matrix = 192 × 119 (Magnetom Sonata); TE/TR/flip-angle = 1.2 ms/60.1 ms/79°, slice thickness = 8 mm, gap = 2 mm, matrix = 192 × 109 (Magnetom Avanto); TE/TR/flip-angle = 1.5 ms/2.9 ms/40°, slice thickness = 10 mm, no gap, matrix = 176 × 168 (Achieva); TE/TR/flip-angle = 1.1 ms/57.9 ms/79°, slice thickness = 8 mm, gap = 2 mm, matrix = 192 × 109 (Magnetom Skyra). LGE imaging was performed with whole-heart coverage of the short-axis following administration of 0.2 mmol/kg gadobutrol (Gadovist, Bayer Healthcare, Leverkusen, Germany), using a T1-weighted mid-diastolic inversion recovery sequence and a patient-adapted prepulse delay (TE/TR/flip-angle = 4.3 ms/750 ms/30°, slice thickness = 8 mm, gap = 2 mm, matrix = 256 × 148 [Magnetom Sonata]; TE/TR/flip-angle = 5.6 ms/488 ms/25°, slice thickness = 8 mm, gap = 2 mm, matrix = 256 × 134 [Magnetom Avanto]; TE/TR/flip-angle = 3 ms/6.1 ms/25°, slice thickness 10 mm, no gap, matrix = 224 × 166 [Achieva]; TE/TR/flip-angle = 3.2 ms/751 ms/25°, slice thickness = 8 mm, gap = 2 mm, matrix = 256 × 156 [Magnetom Skyra]). Images were analyzed by a blinded radiologist with 7 years' experience with cardiac imaging. All routine CMR analyses, except strain and strain rate, were performed using commercially available software (IntelliSpace Portal, Philips Healthcare, Cleveland, OH, USA). LV end-diastolic volume index (LVEDVI), LV end-systolic volume index (LVESVI), LV myocardial mass index (LVMI), LV ejection fraction (EF) and right ventricle EF (RVEF) were derived from short axis-segmentation of CMR. All strain parameters were measured using dedicated software (CVI42, Circle Cardiovascular Imaging Inc., Calgary, Canada) (Fig. 1). LV circumferential strain (EccSAX) and radial strain (ErrSAX) measurements were obtained using mid-ventricular level short-axis cine views. LV longitudinal strain (EllLV) and radial strain (ErrLax) measurements were obtained from a 2-chamber long-axis view. All strain values were calculated by averaging the peak segmental values of radial, circumferential, and longitudinal strain for each strain direction. To assess intra-observer agreement, all measurements were repeated after 1 month in 20 randomly selected subjects. To assess inter-observer agreement for myocardial strain, all myocardial strains were measured in those subjects by another radiologist with 5 years' experience with cardiac imaging. Patterns and presence of myocardial LGE were assessed visually. Patterns of LGE were classified as subendocardial, subepicardial, mid-wall or transmural enhancement.
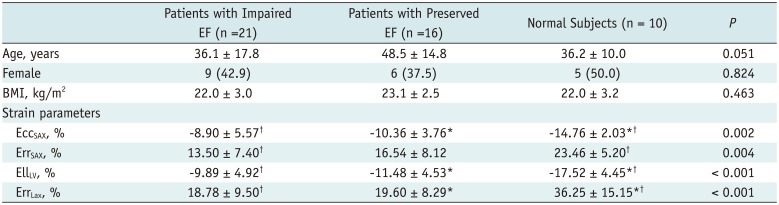
We performed a subgroup analysis between myocarditis patients with a preserved LVEF (≥ 55%, n = 16), myocarditis patients with impaired LVEF (< 55%, n = 21), and normal subjects (n = 10).
Clinical Outcomes
Outcomes were assessed by chart review or telephone interview. As a primary outcome, all patients were followed up to assess the incidence rate of MACE, defined in terms of cardiac death, heart transplantation, implanted cardioverter defibrillator or pacemaker, rehospitalization following a cardiac event, or embolic stroke. Time to MACE is provided in days. Incomplete LV functional recovery was a secondary outcome in the patient group (n = 31) who underwent follow-up echocardiography after 1 year. Incomplete LV functional recovery was defined as an LVEF value < 60% (5). Two-dimensional transthoracic echocardiography was performed by a diagnostic cardiac sonographer using commercial echocardiographic systems (iE33, Philips Electronics, Amsterdam, the Netherlands; Vivid-Q, GE Medical Systems Israel Ltd., Tirat Carmel, Israel; Sequoia, Siemens AG, Munich, Germany) according to a standardized protocol in the cardiac laboratories of Pusan National University Hospital and Pusan National University Yangsan Hospital. The LVEF was measured using the modified Simpson's method as recommended by the American Society of Echocardiography (20).
Statistical Analysis
Statistical analysis was performed using the SPSS for Windows (SPSS Inc., Chicago, IL, USA) and MedCalc (ver. 14.10.2, MedCalc Software, Mariakerke, Belgium) software packages. Categorical group data, presented as percentages, were compared using the chi-square test or Fisher's exact test as appropriate. Continuous variables are presented as means ± SDs and were compared using the Student's t test for normally distributed data or the Mann-Whitney U-test for non-normally distributed data. Normality was tested with the Kolmogorov-Smirnov test. Subgroup analysis between normal subjects, myocarditis patients with impaired EF, and myocarditis patients with preserved EF was performed with a one-way analysis of variance with Bonferroni's correction for normally distributed data, and the Kruskal-Wallis test with a Mann-Whitney U test for ordinary data or non-normally distributed data. Univariate and backward multivariate Cox proportional hazards models were used to assess independent associations with MACE. After setting the cut-off value using receiver-operating characteristics (ROC) curve analysis, Kaplan-Meier curves were calculated to visualize and compare (log-rank test) patients' MACE-free survival curves. Variables that differed significantly between groups, with or without incomplete LV functional recovery on univariate analysis, were analyzed using backward logistic regression analysis to identify independent predictors of incomplete LV functional recovery. ROC analysis was performed to assess the ability of selected variables to predict incomplete LV functional recovery. After setting the cut-off value, the sensitivity and specificity values for incomplete LV recovery were calculated. Finally, intra- and inter-observer reproducibility was calculated using the intra-class correlation coefficient (ICC), where an ICC value < 0.4 represented poor reproducibility, ICC scores between 0.4 and 0.75 indicated fair-to-good reproducibility, and ICC scores > 0.75 indicated excellent reproducibility. A p value < 0.05 was taken to indicate statistical significance.
RESULTS
Study Population
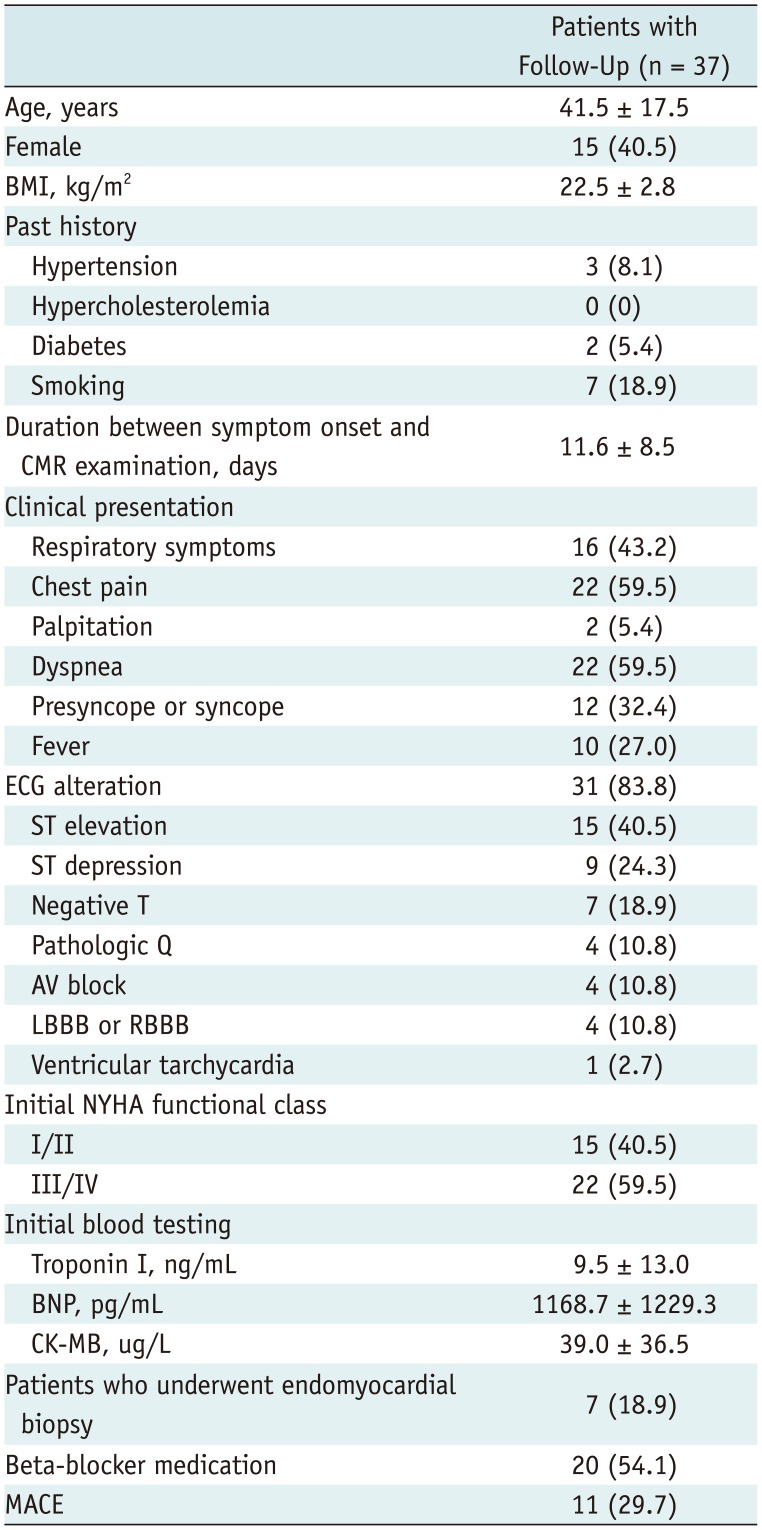
Table 1 summarizes the characteristics of the study cohort. The mean age of the patients was 41.5 ± 17.5 years and 15 (40.5%) patients were female. The most common symptoms were dyspnea and chest pain, followed by respiratory symptoms, and presyncope or syncope. When patients were stratified by the initial clinical manifestation of the disease, 17 patients (45.9%) had infarct-like onsets. Also, 9 patients (24.3%) had arrhythmia such as atrioventricular block (n = 4, 10.8%), left or right bundle branch block (n = 4, 10.8%), and ventricular tachycardia (n = 1, 2.7%). The majority of patients had an abnormal ECG upon admission (n = 31, 83.8%), with ST elevation as the most common finding (n = 15, 40.5%), followed by ST depression (n = 9, 24.3%). EMB was performed in seven patients (18.9%), of whom six were diagnosed with myocarditis using the Dallas criteria. A single patient had a sample insufficient for diagnosis. Beta blockers were used in 20 patients (54.1%).
CMR Findings
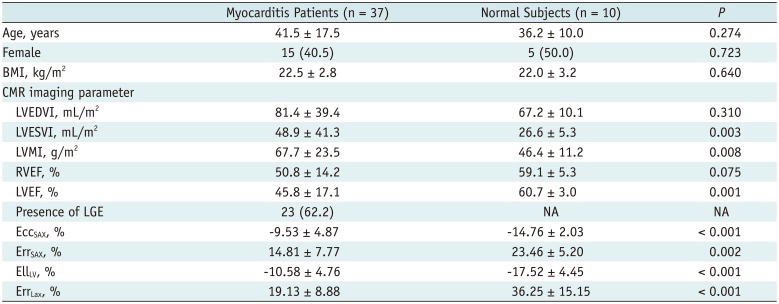
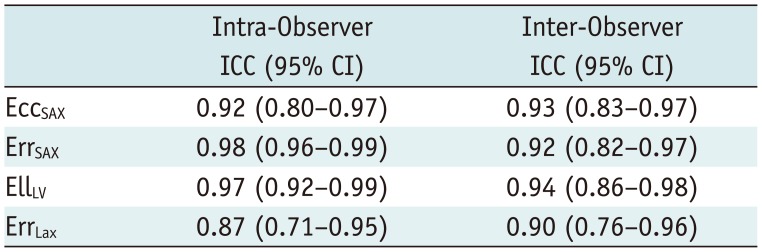
Cardiovascular magnetic resonance was performed within 11.6 ± 8.5 days (range: 0–31 days) of symptom onset in the myocarditis patients. The mean LVEF value was 45.8%, and the mean LVEDVI was 81.4 mL/m2 (Table 2). LGE, which was present in 23 of 37 patients (62.2%), was typically located in mid-wall (6/23, 26.1%) or subepicardial areas (17/23, 73.9%) of the LV wall. There were significant differences between patient and control groups in terms of LVESVI, LVMI, and LVEF. LVEDVI tended to be higher in patients with acute myocarditis. Furthermore, all myocardial strain parameters, including EccSAX, ErrSAX, EllLV, and ErrLax, were significantly lower in patients with myocarditis. Three subgroups showed no significant differences in age (p = 0.051), sex (p = 0.824), and body mass index (p = 0.463) (Table 3). All myocardial strain parameters of myocarditis patients with impaired LV function were significantly reduced compared to normal subjects. Also, EccSAX (−10.36 ± 3.76 vs. −14.76 ± 2.03, p = 0.001), EllLV (−11.48 ± 4.53 vs. −17.52 ± 4.45, p = 0.008), and ErrLax (19.60 ± 8.29 vs. 36.25 ± 15.15, p = 0.001) showed significant differences between patients with preserved EF and normal subjects. However, there were no significant differences in all strain parameters between myocarditis patients with impaired EF and patients with preserved EF. There was excellent intra-observer reproducibility between the first and second evaluations for all strain parameters (ICC = 0.87–0.98) (Table 4). There was also excellent inter-observer reproducibility between two observers for all strain parameters (ICC = 0.90–0.94). There was excellent intra-observer reproducibility (ICC = 0.84–0.97) for LVEDVI, LVESVI, LVMI, and LVEF measurements. Fair-to-good intra-observer reproducibility (ICC = 0.68) was determined for RVEF measurements.
Clinical Outcomes: MACE
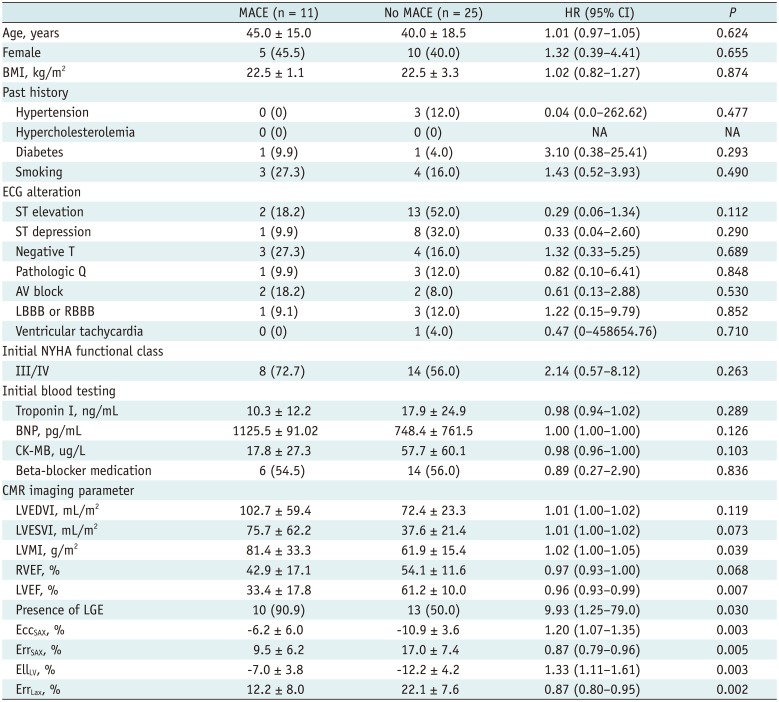
All 37 patients were available for clinical follow-up for at least one year. During an average follow-up of 41 ± 34 months (range: 0–112 months), 11 of 37 patients (29.7%) suffered a MACE, including cardiac death (n = 2), heart transplantation (n = 1), cardiac pacemaker (n = 1), rehospitalization due to cardiac events (n = 4), or embolic stroke (n = 3). All cardiac deaths occurred within 1 month of CMR acquisition.
Table 5 displays the results of the univariate Cox regression analysis used to evaluate the predictors of MACE. The analysis revealed that LVMI, LVEF, the presence of LGE, and EccSAX, ErrSAX, EllLV, and ErrLax, values were significant unadjusted predictors of MACE. Multivariable Cox proportional hazard regression analysis, which included LVMI, LVEF, the presence of LGE and EccSAX, ErrSAX, EllLV, and ErrLax values, indicated that the presence of LGE (hazard ratio, 42.88; 95% confidence interval [CI]: 2.15–855.0, p = 0.014) and ErrLax (hazard ratio, 0.77 per 1%; 95% CI: 0.64–0.92, p = 0.004) were significant predictors of MACE.
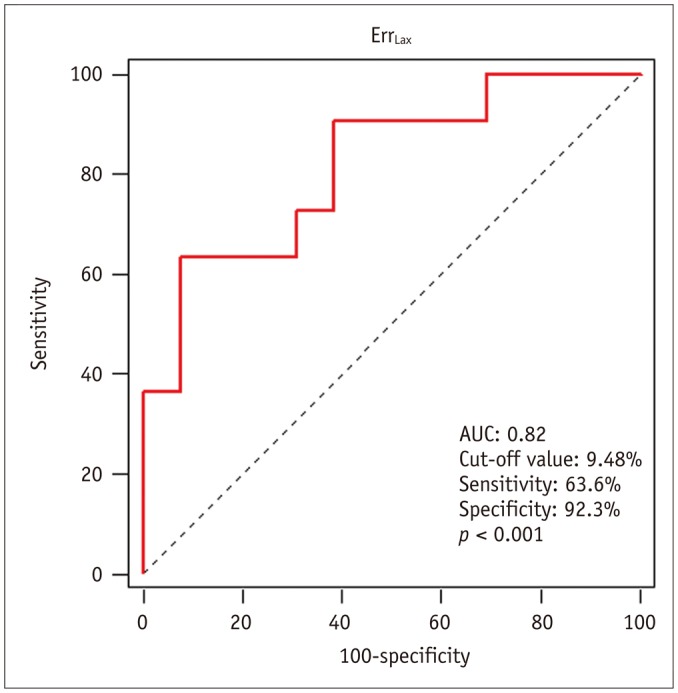
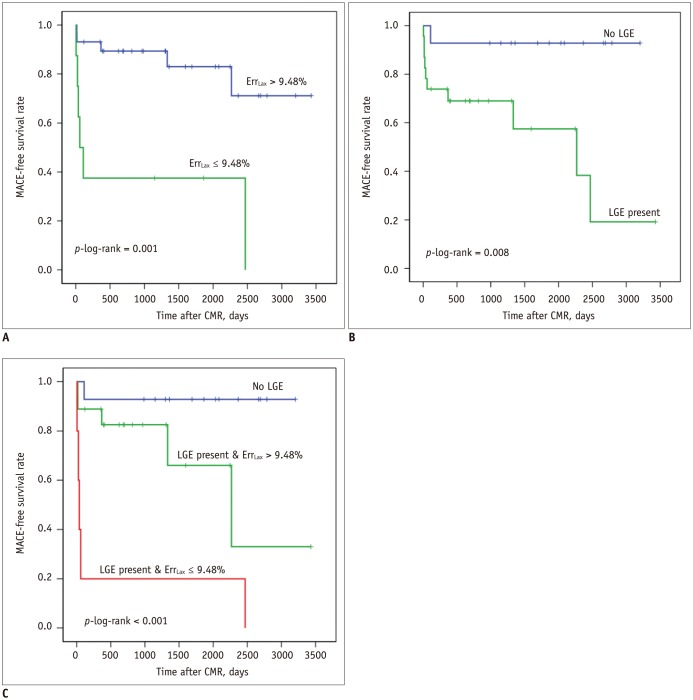
Receiver-operating characteristic curves for ErrLax to obtain optimal cut-off values for predicting MACE during follow-up showed an area under the curve (AUC) of 0.82 (95% CI: 0.657–0.925). The cut-off value with the best combination of sensitivity and specificity for ErrLax was ≤ 9.48% (sensitivity, 63.6%; specificity, 92.3%) (Fig. 2). Kaplan-Meier survival curves for MACE are displayed in Figure 3. Kaplan-Meier analysis demonstrated that the worst outcomes occurred in patients with LGE and an ErrLax value ≤ 9.48%. Only 1 of 14 patients without LGE (7.1%) experienced MACE, whereas 10 of 23 patients with LGE (43.5%) experienced MACE. Figure 3C shows that outcomes in patients with LGE and an ErrLax value ≤ 9.48% were significantly worse than in patients with LGE and an ErrLax > 9.48%. All patients with LGE and an ErrLax value ≤ 9.48% experienced MACE.
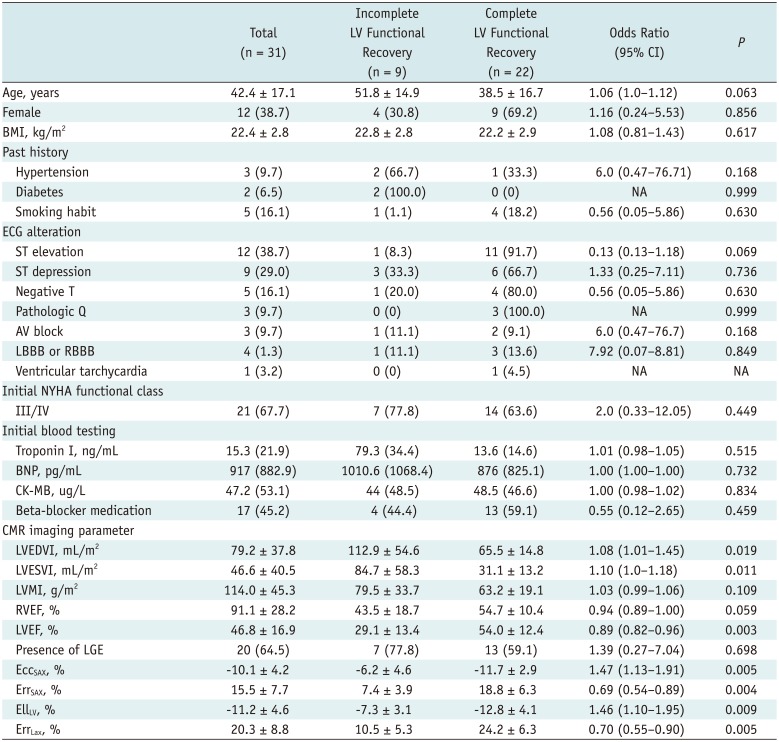
Clinical Outcomes: Functional Improvement
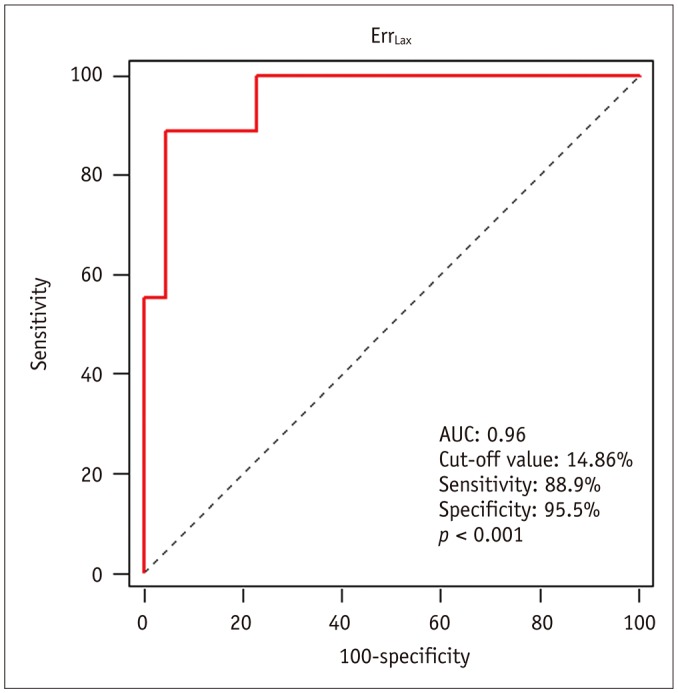
A total of 31 of 37 patients (83.8%) underwent follow-up echocardiography after 1 year. Six patients were excluded because of death during the follow-up period (2/31, 6.5%) or absence of follow-up echocardiography (4/31, 12.9%). Of the 31 patients, 71% (22/31) had normal LVEF on follow-up echocardiography, and 16% (5/31) had normal LVEF on initial echocardiography. Table 6 lists the results of univariate analysis by logistic regression. A multivariable backward stepwise regression analysis, that included LVEDVI, LVESVI, LVEF, EccSAX, ErrSAX, EllLV, and ErrLax values, demonstrated that ErrLax was the only significant predictor of incomplete LV functional recovery (hazard ratio, 0.54 per 1%; 95% CI: 0.29–0.976; p = 0.042). ROC curves for ErrLax to obtain optimal cut-off values for the prediction of incomplete LV functional recovery during follow-up showed an AUC value of 0.96 (95% CI: 0.82–1.0) (Fig. 4). The cut-off value with the best combination of sensitivity and specificity for ErrLax was 14.9% (sensitivity, 88.9%; specificity, 95.5%).
DISCUSSION
This retrospective study presented the following results: 1) all myocardial strain parameters were significantly impaired in patients with acute myocarditis, 2) even patients with a preserved EF showed significantly reduced EccSAX, EllLV, and ErrLax, 3) ErrLax measured on CMR independently predicted MACE or normalized LVEF values in patients with acute myocarditis, 4) all patients with LGE and low ErrLax values experienced MACE.
In contrast to previous studies (521), we included CMR-derived myocardial strain as a possible predictor of MACE or incomplete LV functional recovery in acute myocarditis. Few previous studies have evaluated LV strain in echocardiography of patients with acute myocarditis, or its prognostic values (10). Hsiao et al. (10) reported that longitudinal and circumferential strain measured with echocardiography were significant predictors of major clinical events in 45 acute myocarditis patients. However, their study employed a relatively short follow-up period (mean = 19.8 months), and did not adjust for potential confounding factors through the use of multivariate analysis. Furthermore, echocardiography is inherently limited in patients with poor echogenic windows, and echocardiographic strain parameters may depend on insonation angle (22).
Cardiovascular magnetic resonance-derived feature tracking using steady-statefree precession CMR images is analogous to echocardiographic speckle tracking, but uses a higher spatial resolution and reproducible wall motion tracking (23). One recent study reported that CMR-derived myocardial strain measured with the feature tracking method can predict preserved residual EF in ST elevation myocardial infarction (22). CMR-derived myocardial strain can predict acute myocarditis with high sensitivity and specificity, and significantly reduced cardiac strain is shown even in patients with a preserved EF (91424). However, there are no prior studies on the predictive value of CMR-derived myocardial strain measurements in acute myocarditis patients.
In this study, all strain parameters, including EccSAX, ErrSAX, EllLV, and ErrLax values, were characterized by excellent intra- and inter-observer reproducibility. This result agrees with those of previous studies of CMR feature tracking methods in which considerable intra-observer reproducibility in global myocardial strain measurements was demonstrated (25). In the present study, intra-observer reproducibility was lower for EccSAX than for ErrSAX and EllLV in contrast to previous reports in which EccSAX was the most reproducible strain parameter (2526). This discrepancy may be due to differences in the software used to obtain myocardial strain measurements. Schuster et al. (27), compared the reproducibility of CMR feature-tracking softwares, and found that Circle had better reproducibility for ErrSAX than TomTec (Diogenes or 2D Cardiac Performance Analysis-MR, TomTec GmbH, Unterschleissheim, Germany). In that study, ErrSAX was more reproducible than EccSAX using Circle, which is similar to the result of the present study. Therefore, further studies are required to assess intra- and inter-observer reproducibility of EllLV and ErrLax with respect to the type of feature tracking software used.
Myocardial LGE is a marker of irreversible myocardial injury, e.g., necrosis and fibrosis (16). The presence of LGE is reportedly an independent predictor of a poor outcome, defined as heart transplantation, the requirement for extracorporeal membrane oxygenation or a ventricular assist device, and/or death (521), is in agreement with the present results. Moreover, a recent study of the long-term outcome of patients after acute myocarditis found that NYHA functional class > II and larger LGE mass were independent predictors for the occurrence of long-term MACE (24). LGE was detected in 62.2% of patients in this study, which is a relatively high proportion compared with the 53.2% detected in a previous report (53.2%) (5). This discrepancy may be due to differences in the interval between clinical onset of the disease and CMR examination (mean duration = 11.6 days vs. < 5 days), as well as the characteristics of the study populations. CMR studies conducted during the first day of myocarditis may be less sensitive than those conducted after 7 days because of the focal nature of the early stages of the disease (16). The prominence of LGE may vary accordingly.
The present analysis of the subgroup of patients who underwent follow-up echocardiography revealed that ErrLax values ≤ 14.9% independently predicted incomplete functional recovery (p = 0.042). Although a similar result was obtained previously for myocardial infarction (22), this study assessed, for the first time, the relationship between ErrLax values and myocardial strain. This relationship was based on an analysis of cine images using a feature tracking method during incomplete LV functional recovery in myocarditis. Unexpectedly, LGE did not appear to play a prominent role in this subgroup, contrary to data from a previous myocarditis study (4). This discrepancy may have been due to death during follow-up or absence of follow-up echocardiography in a subgroup of patients. Either of these might introduce a selection bias that could affect the reliability of the data and result in an underestimation of the role of LGE.
This study had several limitations. Its retrospective design and relatively small sample size could be improved in the future by the use of prospective designs and larger cohorts. It included clinically validated suspected acute myocarditis patients only. EMB was not used as a reference standard because of its limited sensitivity (28), and it is not routinely performed in clinical practice. Several previous studies (102930) also relied on a combination of clinical, laboratory, ECG and angiographic findings to identify myocarditis. Furthermore, we could not use Lake Louise Criteria for diagnosis of acute myocarditis, because a T2-weighted sequence or an early gadolinium enhancement sequence was not performed in most cases. Therefore, we included patients with clinically suspected myocarditis according to a combination of clinical, laboratory, ECG and angiographic findings. CMR scanners with different field strengths (i.e., 1.5T and 3T scanners) were used in the present study, which may have affected the imaging analyses. However, previous studies indicated no significant differences in global strain parameters, volumes or EF were found with different field strengths (25).
In conclusion, CMR-derived LV radial strain (ErrLax) values can predict MACE or normalized LVEF in patients with acute myocarditis. The presence of scars, indicated by LGE, is also a good independent predictor of MACE. These results indicate that large, longitudinal follow-up studies are required to further establish LGE and CMR-derived myocardial strain as independent predictors of MACE in acute myocarditis.
 XML Download
XML Download