

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is one of the most common malignant tumors and a leading cause of cancer-related deaths worldwide. According to the latest statistics, 782500 new cases of HCC were diagnosed in 2012 and 745500 of them died with severe prognosis of a median overall survival time of less than a year after diagnosis and an overall survival of less than 5% (1). These data indicated that HCC is a serious health threat to human populations worldwide. Furthermore, < 30% of diagnosed HCC are suitable for curative therapies, such as surgical resection, liver transplantation, ethanol injection and radiofrequency ablation (RFA) (2). Because of the high recurrence rate and cancer mortality, the prognosis of HCC patients is even more discouraging.
Radiofrequency ablation has been widely accepted as an effective curative therapy for small HCC and is reportedly the most effective percutaneous ablation technique because of the higher survival rates (34). The complete response induced by RFA can provide a survival rate that is comparable to hepatic resection (5). Nevertheless, owing to the limited coagulative necrosis induced by RFA alone, the therapeutic effect of RFA in larger HCCs is unsatisfactory (67). To deal with this problem and obtain a larger therapeutic region, many complementary therapies have been used in combination with RFA. Transcatheter arterial chemoembolization (TACE) is also widely used for unresectable HCC such as AsHCC, a type of malignant tumor with hypervascularity, due to its superiority over other therapies such as good tolerability, repeatability and precise targeting, especially for the intermediate-stage HCC (89).
However, RFA and TACE have their own limitations. RFA is suitable for small tumors and it is difficult to achieve complete response in tumors > 5 cm. Furthermore, due to incomplete embolization or tumor angiogenesis, complete necrosis is barely induced by TACE alone. The combined use of TACE with RFA was previously reported and has shown a synergistic effect on ablation of HCC (10111213). Thus, the combination therapy reduces the local progression rate and leads to an improvement of both, the overall and the recurrence-free survival rate in HCC patients. Numerous studies have focused on whether TACE combined with RFA is more effective than RFA monotherapy, but the concluding evidence from these studies is difficult to apply in clinical practice due to conflicting outcomes and poor quality (14151617). On the other hand, combining data from suitable and eligible studies by meta-analysis has the advantage of reducing random error and obtaining precise estimates for clinical interventions. Hence, we performed this meta-analysis to compare the efficacy and safety of combined RFA and TACE with RFA alone for HCC.
MATERIALS AND METHODS
Literature Search
A comprehensive literature search was conducted in Pubmed, Embase, Cochrane Library, Chinese Biomedical Database (CBM), CNKI, and Google Scholar from their inception years to February 13, 2015 to identify relevant reports. The following combinations of search terms was used: ("hepatocellular carcinoma" or "hepatic cancer" or "hepatoma" or "liver cancer" or "liver tumor" or "cancer of liver" or "tumor of liver") and ("transcatheter arterial chemoembolization" or "TACE" or "hepatic artery chemoembolization" or "transarterial chemotherapy embolization" or "transhepatic arterial chemoembolization" or "transarterial chemoembolization") and ("radiofrequency ablation" or "RFA"). Besides, "randomized controlled trails" or "RCT" was used. References cited in the relevant systematic reviews or meta-analyses were also checked for any potential, eligible studies. No other limits were imposed on this search.
Inclusion and Exclusion Criteria
All randomized controlled trials (RCT) comparing combination therapy of TACE and RFA versus RFA monotherapy for HCC and reporting at least one of the main outcomes analyzed in this meta-analysis were included, irrespective of the etiology of liver disease, differences in viral hepatitis, or cirrhotic status. Duplicates, letters to the editor, as well as studies that mixed other effective interventions in either treatment group or control group were excluded. Additionally, studies with inappropriate random method such as randomized according to admission date, admission number, birth date or patient preference were also excluded.
Data Extraction and Quality Assessment
Two authors independently screened the titles, abstracts and full texts to determine whether they met the inclusion criteria; the data was extracted from the eligible studies and assessed for quality. Discrepancies were resolved by discussion or by another author. The extracted contents included general study information (such as title, publication year, authors and country), characteristics of participants and diseases, interventions (such as patients' age and sex, type of study, sample size, interventions, Child-Pugh stage, tumor size, tumor stage, length of follow-up) and outcomes (overall survival, recurrence-free survival, major complications).
The methodological quality of the included studies was evaluated using the risk of bias tool suggested by the Cochrane Handbook for Systematic Reviews of Interventions (18). In addition, to evaluate the quality of evidence from the pooled results, the Grading of Recommendations Assessment, Development, and Evaluation system (GRADE system) was employed (19).
Statistical Analysis
For the time-to-event endpoints (overall survival, recurrence-free survival), hazard ratio (HR) with its corresponding 95% confidence interval (CI) were combined as the effective value to assess the summary effects. The HRs and their 95% CIs were extracted explicitly from the included articles or calculated from the available numerical data using methods reported by Parmar et al. (20). A spreadsheet developed by Tierney et al. (21) was used to perform the calculations. In addition, for major complications, odds ratio (OR) with the 95% CI was calculated using the Mantel-Haenszel method. The chi-square (χ2) was first calculated to assess the heterogeneity of the included studies and the degree of statistical heterogeneity was measured using I-squared statistics. The fixed-effect model was used to pool the results when p > 0.05 and I2 < 50%, indicating no substantial heterogeneity; otherwise, the random-effect model was applied (22). Furthermore, Begg's funnel plot was used to assess publication bias and sensitivity analyses were performed to determine the stability of the pooled effects. We excluded individual studies sequentially to ensure that no single study would be solely responsible for the significance of any result. All p values were 2-tailed, and p values of < 0.05 were regarded as significant. Statistical analyses were performed using Review Manager Software (RevMan 5.2; Cochrane Collaboration, Oxford, UK).
RESULTS
Study Selection and Characteristics
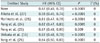
The search strategy initially resulted in a total of 563 studies. After screening the titles or abstracts, and retrieving for full texts when needed, 9 RCTs (161723242526272829) met the inclusion criteria. However, 3 of these studies were excluded, of which, 1 was retracted from JAMA (29) and the other 2 had inappropriate random method (1728). Finally, the remaining 6 RCTs (162324252627) published between 2005 and 2013 with 534 patients were analyzed in this meta-analysis. The key characteristics of the 6 RCTs were outlined in Table 1. The risks of bias in these included RCTs were shown in Figure 1. Notably, double-blind techniques were often impractical because of the nature of the treatments and their possible adverse effects.
Overall Survival
All 6 RCTs including 534 patients provided overall survival information (16, 23-27). The result of the heterogeneity test was p = 0.650/I2 = 0%, indicating no heterogeneity in overall survival between the studies. Therefore, the fixed-effect model was applied to pool the results. The cumulative overall survival in the TACE-RFA combined group was significantly longer than the RFA alone group (HR = 0.62, 95% CI: 0.49-0.78, p < 0.001) (Fig. 2). The specific information of overall survival in the first 5 years was summarized in Table 2.
Recurrence-Free Survival
Information on recurrence-free survival was available for 3 RCTs (162324) with a total of 417 patients. Of the 4 studies, there was no obvious heterogeneity between studies (p = 0.500/I2 = 0%), thus the random-effect model was applied to pool the results. The meta-analysis demonstrated that RFA plus TACE therapy was associated with a significantly higher recurrence-free survival than RFA monotherapy (HR = 0.55, 95% CI: 0.40-0.76, p < 0.001) (Fig. 3). The specific information of recurrence-free survival in the first 5 years was summarized in Table 2.
Major Complications
Five RCTs (1623242527) with 498 patients investigated major complications. The result of the heterogeneity test was p = 0.960/I2 = 0%, indicating no heterogeneity between the studies. Hence, the fixed-effect model was used. The meta-analysis indicated that the combination group had a higher incidence of major complications, as compared with the monotherapy group, but the difference between these 2 groups was not statistically significant (OR = 1.17, 95% CI: 0.39-3.55, p = 0.78) (Fig. 4). The relevant data on complications reported in the RCTs were shown in Table 3.
Evidence of the Critical Outcomes
The GRADE system was used to synthesize and rate the evidence for the outcomes, and the quality of evidence was summarized in Table 4. As a consequence of risk of bias, the overall quality of evidence for those outcomes was of moderate quality. Hence, further research is likely to have an important impact on the confidence in the estimate of effect and may change the current estimate.
Sensitivity Analysis and Publication Bias
Sensitivity analysis by sequential exclusion of individual studies did not alter the corresponding pooled results (Table 5). Hence, the results in this meta-analysis were validated as relatively stable and credible. The publication bias in this meta-analysis was assessed using funnel plot. All 6 eligible RCTs reported relative data on overall survival. The bilateral symmetry shaped funnel plot of overall survival indicated a lack of publication bias (Fig. 5).
DISCUSSION
Comparative effectiveness of RFA combined with TACE vs. RFA alone for HCC has been addressed by numerous investigations but remains a controversial problem. However, most of the evidence from these studies is weak due to research methodology, small sample size or lack of concordance (141516183031). We performed a meta-analysis that included published RCTs to date, in order to obtain more precise estimates and define the effect of clinical interventions more precisely. The meta-analysis showed that the combination of TACE and RFA tends to be associated with significantly higher overall survival and recurrence-free survival than RFA monotherapy in the treatment of HCC. However, there appears to be no significant differences between the combination of TACE and RFA and the RFA monotherapy, in terms of major complication. Despite the moderate overall quality of evidence for the outcomes due to risk of bias, it is notable that double-blind techniques were often impractical because of the nature of the treatments and their possible adverse effects.
Complete necrosis is reportedly achieved in more than 90% of small HCC nodules after RFA (32). Unfortunately, the effect of RFA is not optimistic for medium and large tumors, and local tumor progression frequently occurs in some HCC nodules in which RFA treatment is considered complete and technically successful. RFA and TACE in combination show synergistic effects; furthermore, TACE prior to RFA is beneficial for several reasons. Firstly, TACE can improve the effect of RFA thermal coagulation through reducing the cooling effect of hepatic blood flow. Secondly, TACE can lead to ischemic edema, which may enlarge the area of tumor necrosis induced by RFA. Thirdly, TACE can reduce the portal venous flow by filling the peripheral portal vein around the tumor, and prevent HCC patients from the portal vein invasion (333435). Consequently, RFA can provide a better prognosis for HCC patients with the coordinated effects of TACE.
Of the RCTs included in our meta-analysis, Shibata et al. (16) showed that combined RFA and TACE have overall survival rates and recurrence-free survival rates that are equivalent to RFA alone in patients with HCCs ≤ 3 cm. They concluded that the addition of TACE to RFA for HCCs ≤ 3 cm might not be necessary. Aikata et al. (27) also reported no significant difference in overall survival between the 2 groups in patients with HCCs < 3 cm. Morimoto et al. (25) showed identical overall survival in the combination treatment group among patients with intermediate-sized (3.1-5.0 cm) HCCs. At the same time, Peng et al. (2324) reported a positive result in overall survival and recurrence-free survival among patients with HCCs < 5 cm or 7 cm. These different conclusions may be derived from different tumor size, etiologies of liver disease, multiple tumor lesions, liver function or some other reasons. None of these studies prompted significant difference in major complications between the combination of TACE and RFA and the RFA monotherapy.
Several previous meta-analyses showed the efficacy of TACE combined with RFA, as compared with RFA alone in patients with HCC (3336373839404142). Unfortunately, HRs were under-used in these meta-analyses when assessing time-to-event outcome such as overall survival and recurrence-free survival. Furthermore, the previous meta-analyses failed to consider that time-to-event outcomes have the following 2 important aspects i.e., event occurrence and the time at which the event occurs. ORs measure only the number of events but take no account of time of occurrence. Therefore, they are less appropriate for analyzing time-to-event outcomes, and can pose additional problems in a meta-analysis of time-to-event outcomes (21). We conducted the meta-analysis using HRs, which are considered to be the most appropriate method. The HRs summarizes the difference between 2 Kaplan-Meier curves and represents the overall reduction in the risk of death on treatment, as compared to control over the follow-up period (2043). Specifically, the HR is the odds that the time of survival is longer in patients treated with combined RFA and TACE, as compared to patients treated with RFA only. This implies that the time to the endpoint was increased by the addition of TACE. Furthermore, the GRADE system was applied to assess the quality of evidence summarized in our article and grade strength of recommendations for clinical scientists, which also failed to be used widely and properly in previous studies. Another difference from previous meta-analyses, was the inclusion of RCTs alone, in our article. Thus, the conclusions of the current meta-analysis were valid.
Our meta-analysis had some limitations. Firstly, the heterogeneity of the included studies caused by the inclusion criteria, the etiological factors of HCC, or other reasons might influence the consistency of effects and cause between-study heterogeneity, despite the lack of statistical evidence. Secondly, the safety of the combination of RFA and TACE was not fully assessed due to insufficient data obtained from the included studies, hence, only major complications were analyzed. Thirdly, we included studies that were available only in the abstract form (27), and the reported data may not be as accurate and complete as those reported in the corresponding full text publication.
In conclusion, this meta-analysis suggested that the combination of TACE and RFA is associated with significantly higher overall survival and recurrence-free survival than RFA monotherapy in the patients with HCC without significant difference in major complication between them. These results need to be validated in RCTs with better quality and larger sample sizes.









 XML Download
XML Download