

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recent technological advances have greatly increased the use of computed tomography (CT) for various clinical indications, including detection and staging of disease. CT has been increasingly used to aid medical decision making (1). Despite the enormous contributions of CT to modern healthcare, health problems due to the resulting radiation exposure have become an increasing concern (2, 3). Various techniques to decrease radiation exposure include automated tube current modulation (ATCM), X-ray beam collimation, filtration, and lower tube voltage (4, 5, 6). Of these, ATCM and lowered tube voltage based on clinical application have been proposed (7, 8, 9, 10).
Lowering tube voltage to reduce radiation exposure has been exploited for pediatric patients and CT angiography in recent years (11, 12). Since dose and radiation exposure vary with the square of the voltage given at a fixed tube current (13), lowering the voltage has a greater effect on patient dose than lowering the tube current. However, applying low tube voltage in adult patients with abdominal CT results in increased noise and artifacts. Several recent studies have recommended that tube voltage settings reflect the patient's body size, as well as the diagnostic purpose of the CT examination. Among them, a study by Yu et al. (10) demonstrated the feasibility of automatic tube voltage selection (ATVS) based on the patients' body habitus and the specific diagnostic task at hand. Commercially available software (CARE kV; Siemens Healthcare, Forchheim, Germany) that allows the simultaneous use of ATVS and ATCM has recently been developed.
Diagnostically unacceptable noise and artifacts are major concerns when lowering radiation dosage with conventional filtered back projection (FBP). Several approaches including noise reduction kernels, filters, image and projection-space de-noising, and iterative reconstruction (IR) algorithms have been explored to reduce image noise and artifact while maintaining image quality in low-dose CT. Sinogram-affirmed iterative reconstruction (SAFIRE) is one of the most recently developed raw data-based (sinogram data) IR algorithms with 5 presets (IR strength of 1-5). Unlike previous IR algorithms, which only work in image domain-based iterative processes, SAFIRE uses multiple comparisons between the reconstructed and measured data in the raw data domain to iteratively correct images (14). Recently, the feasibility of the combined used of CARE kV and SAFIRE in abdominal CT with emphasis on image noise measurement was explored (15). However, the lack of subjective image quality assessment was a limitation.
Therefore, the purpose of our study was to compare the radiation dose and image quality between standard-dose CT and a low-dose CT obtained with the combined use of CARE kV and SAFIRE for contrast-enhanced CT examination of the liver.
MATERIALS AND METHODS
This study was composed of 2 phases. In the first phase, we evaluated the appropriate level of SAFIRE in CARE kV-applied low-dose CT (protocol B) by qualitative and quantitative analysis. In the second phase, we directly compared a CARE kV-applied low-dose CT reconstructed with the appropriate level of SAFIRE to previously taken standard-dose CT scans (protocol A).
Patient Population
This retrospective study was approved by the Institutional Review Board of our hospital. Due to the retrospective nature of the current study, the requirement for written informed consent was waived. We identified 345 consecutive adult patients who underwent contrast-enhanced CT including the liver with a 128-slice multidetector-row CT (MDCT) (SOMATOM Definition AS+; Siemens Healthcare, Forchheim, Germany) by using both CARE kV and SAFIRE, between November 2012 to February 2013. The CT examinations were requested in regards to chronic liver disease or liver cirrhosis of the patients. We selected patients for evaluation (n = 67) who had been previously scanned on a 64-slice MDCT (SOMATOM Definition AS, Siemens Healthcare, Forchheim, Germany) to compare radiation dose and image quality (average time interval, 11.3 ± 7 months). The study population consisted of 48 men and 19 women, whose mean age was 62.4 ± 10.7 years (range, 27-84 years). The mean height was 163.8 ± 7.0 cm (range, 146-178 cm), the mean weight was 61.2 ± 8.6 kg (range, 44-85 kg), and the mean body mass index (BMI) was 22.8 ± 2.8 kg/m2 (range, 17.3-33.2 kg/m2). There was no significant difference in the BMI of the patients between the 2 CT scans (22.9 ± 2.7 kg/m2 for the initial scan and 22.8 ± 2.8 kg/m2 for the follow-up scan, p = 0.48 by the Wilcoxon signed rank test).
CARE kV and SAFIRE
CARE kV is an automated attenuation-based tube voltage selection algorithm with tube current adaption. It was designed to automatically recommend an optimal combination of tube potential and tube current for each patient, based on the patient's topogram. CARE kV works in conjunction with ATCM (CARE Dose 4D; Siemens Medical Solutions) to maintain equivalent image quality, as described previously (1, 16, 17, 18). Briefly, the algorithm calculates the required tube current to reach an operator-selected contrast behavior (identification of scan type or tissue of interest, e.g., Scan type "Nonenhanced CT", "Angiography CT" or tissue of interest "Bone", "Liver") according to the patient's attenuation along the z-axis obtained from the CT topogram. Once optimal settings are determined, the tool checks the system to see if the optimal setting is possible (due to tube current limits, pitch settings, scan range, etc.) at a low tube potential, such as 80 kV. If the required tube current at any location of the CT topogram exceeds system limits, the software switches to the next higher tube potential (100, 120, or 140 kV) and the calculation is repeated.
Sinogram-affirmed iterative reconstruction is one of the most recently introduced iterative reconstruction processes. It differs from its predecessor (iterative reconstruction in image space or IRIS), by working both in the raw data domain and the image domain to reduce noise and maintain image sharpness. As in traditional IR, initial reconstruction using a weighted FBP is performed, followed by the introduction of 2 different correction loops in the reconstruction process. The first loop, where data is re-projected into the raw data space (sinogram data), is utilized to correct imperfections in the original reconstruction and remove artifacts. The detected deviations are again reconstructed using the weighted FBP, yielding an updated image. This loop is then repeated a number of times depending on the type of examination. The second correction loop occurs in the image space, where noise is removed from the image through a statistical optimization process. The corrected image is compared to the original and the process is repeated a number of times depending on the examination type. Five presets (strength of 1-5) are available with strength 1 (S1) being noisier and strength 5 (S5) being smoother in order to take the reader's preference and image quality requirements for different exam types into account. The strength is not related to the number of iteration loops and will not affect reconstruction time (19, 20, 21).
CT Protocol
Initial CT scans were performed on a 64-slice MDCT, and follow-up CT scans were performed on a 128-slice MDCT.A quadruple-phase CT consisting of precontrast, arterial phase, portal venous phase and delayed phase imaging was performed for all patients. All patients received 2 mL/kg total body weight of an intravenous (IV), non-ionic contrast medium containing an iodine concentration of 350 mg/mL (iomeprol, Iomeron 350; Bracco Imaging, Milan, Italy). Contrast medium was administered via a mechanical power injector (Stellant D CT, Medrad, Pittsburgh, PA, USA) at a rate of 3-5 mL/s through an 18-22-G IV catheter inserted into an arm vein, followed by a 40 mL saline flush administered at the same injection rate. Computer-assisted bolus-tracking software was used to determine the optimal scan delay for the arterial phase in each patient. Acquisition of the arterial phase started 12 seconds after the trigger threshold (100 Hounsfield units [HU]) was reached at the level of the descending thoracic aorta. The portal venous and delayed phases started 55 and 120 seconds after the trigger threshold, respectively.
The initial CT scan was performed with a fixed tube potential of 120 kV and an FBP algorithm (protocol A), whereas the follow-up CT scan was performed using CARE kV with the "Liver" contrast setting and the SAFIRE algorithm (protocol B). CARE Dose 4D was used for both protocols, with a quality reference tube current (reference mAs) of 210 mAs for protocol A and 179 mAs for protocol B (18). The other CT parameters were a beam collimation of 64 × 0.6 mm (protocol A) or 128 × 0.6 mm (protocol B), gantry rotation time of 0.5 seconds, section reconstruction thickness of 3.0 mm, and an image reconstruction interval of 3.0 mm. Images were reconstructed with B30f for protocol A (a medium-smooth soft tissue convolution kernel) and I30f for protocol B (a medium-smooth SAFIRE specific soft tissue kernel corresponding to the B30f FBP kernel). The scan range was from the dome of the diaphragm to the pelvic floor, for the portal venous phase and the dome of the diaphragm to the lower pole of the kidney for the precontrast, arterial and delayed phases.
Image Reconstruction of Protocol B
The images of protocol B were reconstructed for each patient using 3-mm section thickness and a 3-mm interval. Images were reconstructed using a standard FBP algorithm and a SAFIRE algorithm with a reconstruction strength of 1 to 5 during the portal venous phase. The 6 different reconstruction images, i.e., FBP (S0), and SAFIRE with strength 1 (S1) through 5 (S5), were generated from the same raw data for each patient and were then sent to and archived in our picture archiving and communications system (Maroview 5.4, Infinitt, Seoul, Korea).
Image Analysis
Qualitative Analysis: Protocol B
Qualitative analysis of protocol B images were done to determine the appropriate IR strength level of SAFIRE. Two radiologists, both with 5 years clinical experience in reading liver CT scans, independently assessed the SAFIRE images at a workstation (HP Z600, Hewlett-Packard Development Company, Palo Alto, CA, USA) that had a spatial resolution of 1536 × 2048 (PGL21, WIDE, Seoul, Korea), by using a picture archiving and communications system. Readers were blinded to the CT parameters and reconstruction methods, and the order of the 6 image sets was randomized to minimize recall bias. The criteria for image grading were established by consensus between the 2 radiologists before the start of image reading, to improve interobserver agreement. The parameters assessed by subjective CT image reading included image noise, visibility of small anatomic structures, pixelated image appearance and overall diagnostic confidence.
Subjective image noise was assessed using a 5-point scale (1 = unacceptable image noise, 2 = above average noise, 3 = average image noise, 4 = less than average noise, and 5 = minimal image noise). The visibility of small anatomic structures, such as intrahepatic small vasculature, was graded using a 5-point scale (1 = unacceptable visualization, 2 = suboptimal visibility, 3 = acceptable visibility, 4 = above average visibility, and 5 = excellent visualization). Pixelated image appearance was graded using a 3-point scale (1 = absent, 2 = present but not affecting interpretation, 3 = present and affecting image interpretation) and overall diagnostic confidence was assessed using a 5-point scale (1 = unacceptable diagnostic image quality, 2 = sub-diagnostic confidence, 3 = average confidence, 4 = better than average, and 5 = completely confident). The image quality attributes assessed in our study have been described in the European Guidelines on Quality Criteria for Computerized Tomography and have been used in numerous previous studies published in the radiology literature (22). The optimal IR strength was determined based on these grading results and the IR level, the main focus, showed the highest score in the visibility of small anatomic structures and overall diagnostic confidence.
Quantitative Analysis: Protocol A and B
Images from protocols A and B were evaluated together for quantitative analysis, since region of interest (ROI) measurements were not affected by each other. Quantitative measurements were performed at a commercially available workstation (Advantage Windows 4.2; GE Healthcare, Milwaukee, WI, USA) by an experienced radiology research personnel who was blinded to the image review results. The 7 image sets (i.e., 1 image set from protocol A and 6 image sets from protocol B, respectively) were displayed side by side with a preset soft-tissue window. The window width and level were 380 HU and 55 HU for protocol A and 410 HU and 65 HU for protocol B, respectively. We measured image noise and attenuation values of the liver, portal vein and paraspinal muscle, as described previously (9, 23). Objective image noise was measured for 469 image sets (7 image sets from each of 67 patients) as the standard deviation of the pixel values from a circular or ovoid ROI placed in a homogenous region of subcutaneous fat of the anterior abdominal wall. To ensure consistency, all measurements were performed twice at the level of the main portal vein and the mean was calculated.
Mean CT attenuation values (in HU) of the portal vein, liver parenchyma and paraspinal muscle were obtained on the portal phase of CT scanning. The attenuation of the portal vein was measured from a single ROI placed at the portal vein confluence level. The liver attenuation was recorded as the mean of the measurements of 4 ROIs in the medial and lateral segments of the left hepatic lobe and in the anterior and posterior segments of the right hepatic lobe (9). Areas of focal change in the liver parenchyma, visible blood vessels, bile ducts and prominent artifacts were carefully avoided during ROI selection. The attenuation of the paraspinal muscles was recorded as the mean attenuation of 2 ROIs that avoided macroscopic fat infiltration in the right and left paraspinal muscle at the level of the portal vein confluence. The size, shape, and position of all ROI measurements were kept constant by applying the copy-and-paste function at the workstation.
The contrast-to-noise ratio (CNR) values relative to paraspinal muscle for the organ of interest were calculated using the following equation (24): CNRo = (ROIo - ROIm) / SDn, where ROIo is the mean attenuation of the organ of interest, ROIm is the mean attenuation of the paraspinal muscle, and SDn is the mean image noise. SNRliver and SNRportal vein values were calculated by dividing the mean attenuation of the liver and portal vein by the mean image noise.
Image Analysis: Protocol A vs. Protocol B with Optimal IR Strength
After the appropriate IR strength of SAFIRE was determined, these images were compared with a standard-dose CT (protocol A) of the same patient. Previously measured data were used for quantitative measurement comparison. Qualitative analysis was done by the 2 radiologists, with 20 and 6 years of clinical experience, with the same parameters previously used, including the ability to choose 'preferred image' as either A or B. If the 2 images were considered almost the same, their choice was recorded as 'both'.
Radiation Dose Estimation
The volume CT dose index (CTDIvol) was obtained from the patient protocol that summarized the individual radiation exposure parameters of each CT scan. Radiation dose reduction (in percentages) was calculated based on the CTDIvol of protocol B divided by the CTDIvol of protocol A (25).
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD) or the median value and its range. Categorical variables were expressed as frequencies or percentages. For qualitative analysis of protocol B, the Friedman test was used. Additionally, when there was a statistically significant difference, a post-hoc analysis with pairwise comparison of variables according to Conover was performed (26). For quantitative analysis including both protocol A and B, we used the repeated analysis of variance test to compare statistically significant inter-group differences. When there was a statistically significant difference, a post-hoc analysis with Bonferroni correction was performed. After determining the appropriate IR strength level of protocol B, 2 image sets (protocol A and the 'appropriate level' image from protocol B) were compared using a Wilcoxon signed rank test for qualitative analysis. For items where 2 readers' data were present, the analyses used the average of the 2 readers' results and interobserver agreement between the 2 readers was additionally measured using the kappa. The scale for the k coefficients for interobserver agreement was as follows: less than 0.20, poor; 0.21-0.40, fair; 0.41-0.60, moderate; 0.61-0.80, substantial; and 0.81-1.00, almost perfect (27). Wilcoxon signed rank test was used to evaluate the statistical significance of radiologists' preference. All statistical analyses were performed using the MedCalc version 12.4.0.0 (MedCalc, Mariakerke, Belgium). A p value of < 0.05 was considered significant.
RESULTS
Qualitative Analysis: Protocol B
The image quality scores determined by the 2 radiologists and the level of interobserver agreement were shown in Table 1. The image noise decreased significantly as the SAFIRE level increased (p < 0.05). Visibility of small anatomic structures and overall diagnostic confidence were the highest with S2 (4.0 ± 0.4, 4.1 ± 0.5). The pixelated image appearance increased as the SAFIRE level increased (Fig. 1). Interobserver agreement was moderate to almost perfect.
Quantitative Analysis: Protocol A and B
Increased SAFIRE strength was associated with a linear noise reduction and a linear improvement in SNR and CNR. In direct comparison with FBP of protocol B (S0), the noise decreased significantly in all of the SAFIRE images (S1-S5, p < 0.05). The mean CT attenuation of the portal vein differed significantly between protocol A and protocol B (p < 0.05). There were no significant differences in the mean CT attenuation of the liver parenchyma and paraspinal muscles in the image sets including protocol A. There were no significant differences in the noise, signal-to-noise ratio (SNR) and CNR between protocol A and S2 images (Table 2).
Image Analysis: Protocol A vs. Protocol B (S2)
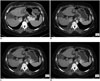
Objective image noise was lower in protocol B compared to protocol A, without statistical significance. There was no significant difference in the mean CT attenuation of liver and paraspinal muscles. The mean CT attenuation of the portal vein was significantly higher with protocol B (216.2 ± 40.8 vs. 233.1 ± 44.2, p = 0.005). There were no significant differences in SNRliver, SNRportal vein, and CNRportal vein (Table 2). Qualitative analysis results were shown in Table 3. Interobserver agreement was moderate to almost perfect. The radiologist with 20-year of clinical experience preferred both images in 53.7% (36/67), protocol A in 28.4% (19/67), and protocol B in 17.9% (12/67). The radiologist with 6-year clinical experience preferred both images in 59.7% (40/67), protocol A in 10.4% (7/67), protocol B in 29% (20/67) (p < 0.001) (Fig. 2).
Radiation Dose Estimation
All of the patients (67/67, 100%) were scanned with a tube potential of 100 kV for protocol B. During the study period, there were 2 patients (BMI of 19.1 and 19.3 kg/m2) for whom 80 kV was recommended by CARE kV as the optimal tube potential. However, these patients were excluded from our study because there were no previous CT scans available. 120 kV and 140 kV were not recommended by CARE kV in any of the cases. The mean effective mAs (eff. mAs) was 120 ± 25.6 eff. mAs for protocol A (range, 87-249 eff. mAs) and 120 ± 22.6 eff. mAs for protocol B (range, 89-244 eff. mAs; p = 0.8). CTDIvol was significantly lower for protocol B (4.7 ± 0.9 mGy) compared to protocol A (8.8 ± 1.7 mGy; p < 0.001). The mean percentage dose reduction was 46.6%.
DISCUSSION
Our study demonstrated that by combining CARE kV and SAFIRE a significant radiation dose reduction was possible without altering subjective and objective image quality in evaluating the liver on the portal phase CT. Lowering the tube potential has the advantage of providing higher attenuation of iodinated contrast media, due to a greater photoelectric effect and decreased Compton scattering (10, 28). Even with the higher image noise in low kV images, CNR remained similar to those for 120 kV, as a result of increased contrast. CARE kV automatically selects the optimal tube potential with the lowest radiation dose estimated based on the patient's attenuation data obtained from the scout scan and the diagnostic purpose. A recent study has shown that combined use of ATVS and ATCM allowed reduction of the radiation dose while maintaining good image quality (1). In order to maintain image quality (e.g., 210 reference mAs at 120 kV, recommended by the vendor), however, tube current has to be increased. When only CARE is applied with kV with reference mAs of 210 mAs in 128-slice MDCT, the gross reduction in radiation dose is about 10-30% (1, 17, 18, 29). We hypothesized that the radiation exposure could be further decreased with the application of IR algorithm to CARE kV, as SAFIRE's denoising ability and artifact removal can compensate for the weak points of low-dose CT. We therefore attempted to lower the tube current (eff. mAs) by lowering the quality reference mAs to 179 mAs, which is controlled by ATCM (CARE Dose 4D). Additionally, since SAFIRE is provided with 5 levels of IR strength, the most appropriate level of SAFIRE was evaluated by quantitative and qualitative analysis. Our results are in good agreement with study by Kalra et al. (19), which found that lower iteration settings of S1 and S2 enabled a 50% dose reduction to 5.5 mGy for an abdominal CT examination. Although radiation dose was solely reduced by lowering quality reference mAs, they showed that these images have a pixelated, blotchy appearance, even though higher levels of SAFIRE enable remarkable noise reduction. We found that S2 was appropriate for CARE kV-applied low-dose CT, and the final image was of acceptable quality, without any blotchy, pixelated images. We also found that better SNR and CNR were obtained. Though the main goal behind CARE kV is to keep the CNR the same, the resulting CNR of our images from protocol B was better than that of protocol A. This is explained by the effect of SAFIRE, which reduces image noise without altering other image quality-related parameters. As a result, the overall image quality made by CARE kV with 179 reference mAs and SAFIRE reconstruction was almost the same as the previous standard dose CT with 120 kV and 210 reference mAs, but the effective radiation dose was almost the half of the standard-dose CT (effective dose, 3.5 mSv).
One of the recent studies by Shin et al. (15) proved that CT dose reduction up to 41.3% may be achieved without increasing image noise by applying CARE kV and SAFIRE. Based on the quantitative measurement of CT attenuation and image noise of 4 different organs/tissues, they suggested that IR strength of 3 or 4 in case of 30% mAs reduction could present similar image noise levels to the standard dose images. IR strength of 3 or 4 was suggested as a result of similar image noise between the prior standard dose CT and CARE kV applied with SAFIRE strengths of 3 and 4 in the aorta, liver and muscle. However, the image noise of subcutaneous fat was similar to SAFIRE strengths of 1 and 2. In their study, quantitative measurements were done with 1 circular ROI in each organ/tissue, and the reference mAs of standard dose CT and CARE kV applied CT was different from that used in our study (240 and 170 mAs vs. 210 and 179 mAs). They did not perform any subjective image quality assessment and did not evaluate the effect on diagnostic performance. IR strength of 2 determined by our study, in contrast, was based on both qualitative and quantitative analysis. However, due to differences in CT acquisition parameters, patient's body habitus and many other factors, IR strength could be suggested but should be selected according to each institution's protocol and reader's preference.
Previous studies on low kV CT have raised concerns that images become noisier and that artifacts or pixelated images are created as the tube potential decreases or the iterative reconstruction strength increases. Therefore, our major objective was to maintain the 'look-and-feel' appearance of low-dose CT when combined with IR algorithm. To prove that image quality was not altered by CARE kV and SAFIRE, a previous standard-dose CT was evaluated for image analysis and radiation dose estimation intraindividually. This scan was performed at a different CT scanner (64-slice MDCT vs. 128-slice MDCT). A previous study by Eller et al. (16) compared standard 120-kV CT performed with a 128- or 64-slice CT scanner to an ATVS CT performed with a 128-slice CT scanner for evaluation of subjective image quality. The radiation dose was compared by using the estimated CTDIvol by switching off the CARE kV in the scanner console, without actually performing the scan. Due to the retrospective design of our study, however, we could not have estimated CTDIvol with CARE kV switched off. Therefore, we used previous CT scans for comparison, and attempted to select similar scanning parameters by selecting patients who had a previous CT scan performed with Definition AS. The radiation exposure in protocol A was lower than many other studies using 64- or 128-slice MDCT with standard-dose abdominal CT protocol (1, 16, 30).
The comparison of the standard-dose CT (protocol A) with low-dose CT (S2 of protocol B) had no severe artificial appearance in the 2 image sets as evaluated by both readers. Although there are many IR algorithms in the literature, some radiologists, especially those with relatively longer clinical experience, are unfamiliar with iteratively reconstructed images. While it is possible that radiologists with more clinical experience may need to adapt to newer imaging technologies, their preference must be considered when designing scan protocols. Therefore, we attempted to improve image quality by comparing standard-dose CT as a reference.
Interestingly, all of the CT scans with CARE kV in our study were performed at a tube potential of 100 kV. This might be explained by the fact that in CARE kV, the algorithm for selection of tube potential, has a physics-based parameterization in maintaining equal CNR, which may result in unusual behavior. Previous reports on CARE kV indicated a significant correlation between the automatically selected tube potential and body habitus, including BMI and abdominal body diameter. However, there was considerable overlap in these parameters and the various selected tube potentials (1, 16, 17, 18). Since some low tube potentials might require tube currents exceeding the maximum possible tube current of the CT scanner, they are discarded by the algorithm and the next higher tube potential is proposed. We assume that since quality reference mAs of our study was low, scanning overweight or obese patients (BMI, 23 kg/m2 or greater) with tube potential of 100 kV was possible (i.e., did not exceed the maximum possible tube current of the CT scanner) (Fig. 3).
There are several limitations to our study. This study was a retrospective study with a non-randomized, small number of patients seen at a single institution. Multicenter, prospective clinical trials will be needed in order to validate our study results. CT scans were performed with 100 kV, so the impact of applying CARE kV was subtle. As there was only 1 patient with a BMI > 30 kg/m2 (33.2 kg/m2) and none with a BMI < 18.5 kg/m2, it was inevitable that the most of the scans would be performed with a tube potential of 100 kV. Also, there was a limitation in generalization of our results as this study was performed with scanners from a single vendor and used vendor-specific software. Optimal IR strength selected in our study (S2) is another limitation since it was also study specific. As the body sizes of Asians are smaller than those of North Americans and Europeans, the applicability of our findings to heavier patients is uncertain. Additional studies to validate our study results in heavier patients would be required. Additionally, 2 protocols were performed at 2 distinct time points with different CT scanners. However, we found no difference in the patient's body habitus between the 2 protocols. We did not evaluate the diagnostic performance for hyper- or hypovascular hepatic lesions. Considering the higher CNR and SNR of our study results, further study including the hepatic tumors is warranted.
In conclusion, our results showed the potential of combining CARE kV and SAFIRE in contrast-enhanced liver CT. Through automated tube potential selection and iterative reconstruction with IR strength of level 2, radiation dose was reduced by a mean of 47% while maintaining image quality.





 XML Download
XML Download