

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Differentiation between malignant and benign pulmonary nodules is a common problem encountered by radiologists which has provided the impetus to explore alternative imaging techniques. Accurate diagnosis can reduce unnecessary thoracotomies in patients with benign diseases (1). Metabolic imaging with 2-(18F)-fluoro-2-deoxy-D-glucose positron emission tomography (PET) is being used more and more to differentiate benign from malignant focal lesions and it has been shown to be more efficacious than conventional chest CT (2). It has a unique ability to differentiate benign from malignant nodules, and it offers a different approach to the diagnosis of chest diseases because it exploits fundamental biochemical differences between benign and malignant cells (2).
However, fluorodeoxyglucose (FDG) is not a cancer-specific agent, and false positive findings in benign diseases have been reported in active inflammation or infection, causing false-positive results (1, 2). In addition, the malignant tumors with low metabolic activity (3) or tumors smaller than 1.0 cm in diameter (1) often show false negative results. Furthermore, the accuracy of FDG-PET scans in detecting pulmonary metastases in patients with cancer has not yet been established.
Awareness of the conditions and the mechanisms by which false positive and negative results occur will help radiologists interpret PET scans more accurately and also will help to determine the significance of the findings. In this review, potential sources of false-positive and false-negative findings are illustrated in a variety of lung diseases.
BASIC CONCEPT OF FDG-PET IMAGING
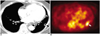
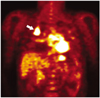
Fluorodeoxyglucose is an analog of glucose and is used as a tracer of glucose metabolism. There are several sites of normal physiologic accumulation of FDG (Fig. 1). It accumulates in various normal organs which use glucose for metabolism, including the brain, muscles, salivary glands, myocardium, gastrointestinal tract, urinary tract, thyroid gland, and gonadal tissues. In additional, increased FDG uptake in brown adipose tissue in the neck has been reported as a false positive result in 2.3-4% of patients. Brown adipose tissue is responsible for cold-induced and diet-induced thermogenesis. Mitochondria in brown adipose tissue exclusively express the thermogenic protein, and FDG uptake in hypermetabolic brown fat can occur, as glucose transporters have been observed in brown adipose tissue (Fig. 2) (2).
The mechanism by which FDG uptake in tumor cells and other pathologic conditions occurs is due to an increased number of glucose transporter proteins and increased intracellular hexokinase and phosphofructokinase levels, which promote glycolysis. In the normal glycolytic pathway, FDG behaves similarly to D-glucose in its transport through the cell membrane and phosphorylation by hexokinase. Once FDG is phosphorylated, structural changes made by a hexose-phosphate bond prevent FDG from being catabolized or transported back into the extracellular space in substantial amounts. This process is called "metabolic trapping," and it makes increased uptake and accumulation of FDG occur within abnormally metabolizing tumor cells (2).
Abnormal areas of FDG accumulation are detected by comparing the uptake with background activity. In the lungs, focal abnormalities that have a greater uptake than the mediastinal blood pool on attenuation corrected images are highly suggestive of malignancy. FDG PET also provides quantitative data in the form of the standardized uptake value (SUV) or standardized uptake ratio (SUR) (2). The SUV is obtained by putting the circular region of interest over the portion of the lesion with the greatest accumulation of FDG (3). The mean SUV is obtained by dividing the activity (µCi/mL) in the region of interest (ROI) by the injected dose in µCi divided by patient weight in grams (3).
SUV = (average ROI activity [µCi /mL]) / (injected dose [µCi] per body weight [g])
Increased body fat elevates the SUV, therefore, correction with lean body mass (SUVLBM) is required to avoid erroneous comparisons that can result from changes in pre- and post-therapy body weight in the same patient (2). The maximum SUV is obtained by using the maximum activity in the ROI instead of the mean activity (3). Notwithstanding the controversial views, SUVs of 2.5 or greater have been used as a cutoff value indicative of malignancy (3). Gupta et al. (4) reported that FDG-PET is superior to CT, when considering overall sensitivity, specificity, and accuracy of PET for staging mediastinal lymph nodes was 96, 93, and 94%, compared to 68, 65, and 66% with CT.
FALSE POSITIVE FINDINGS
Inflammatory cells such as neutrophil and activated macrophages at the site of inflammation or infection show increased FDG accumulation (5). Active granulomatous processes, other infectious conditions and active fibrotic lesions have also been reported to show increased FDG accumulation and cause false-positive PET scans for malignancy.
Tuberculoma and Tuberculous Lymphadenopathy
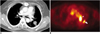
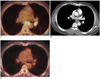
Tuberculoma is one of the most well-known diseases that show intense FDG uptake (Fig. 3A). Active granulomatous processes such as tuberculosis have been reported to accumulate FDG (1, 2). Tuberculoma typically appears as a fairly discrete nodule or mass (Fig. 3B) in which repeated extensions of infection have created a central caseous necrosis surrounded by a mantle of epithelioid cells and collagen with peripheral inflammatory cell infiltration (1).
Activated inflammatory cells have markedly increased glycolysis. The hexose monophosphate shunt is stimulated by phagocytosis, with increases of 20-30 times that of baseline values which is the cause of high FDG uptake (6). Tuberculous lymphadenopathy can be understood in the same manner as tuberculoma in the lung parenchyma (Fig. 4).
Elevated glucose levels can accelerate false positive results in inflammatory conditions. It has been suggested that inflammatory cells use more glucose under hyperglycemia than in euglycemia, and therefore, lesions containing such cells are more likely to be interpreted as malignant lesions under such conditions (5).
Sarcoidosis
Sarcoidosis is a chronic multisystem disorder. It can be characterized in affected organs by an accumulation of T lymphocytes and mononuclear phagocytes, noncaseating epithelioid granulomas, and derangements of the normal tissue architecture. The etiology is unknown, but it is thought to be caused by exaggerated cellular immune responses.
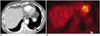
Pathologically, the first manifestation of the disease is an accumulation of mononuclear inflammatory cells, mainly CD4+ T helper 1 lymphocytes and mononuclear phagocytes, in the affected organ. This inflammatory process is followed by the formation of granulomas, aggregates of macrophages and their progeny, epithelioid cells, and multinucleated giant cells (7). Active granulomatous conditions with aggregation of inflammatory cells in sarcoidosis results in accumulation of FDG (1-3, 8), and it has been suggested that intensity of FDG uptake may reflect disease activity (9) (Fig. 5).
Cryptococcosis
Cryptococcosis is an infection caused by the yeast-like fungus Cryptococcus neoformans. This fungus reproduces by budding and forms round, yeast-like cells. Infection occurs by inhaling the fungus into the lungs. Pulmonary lesions are characterized by intense granulomatous inflammation (10). There are some reports which have showed high FDG uptake causing false positive results in cryptococcosis (8) (Fig. 6).
Paragonimiasis
Paragonimiasis is a food-borne parasitic disease common in south Asia, particularly in Japan, Korea and parts of China (11). Pulmonary paragonimiasis is a disease caused by a lung flake. Once ingested by humans, by eating infected crabs or crayfish, the larvae excyst in the small intestine, penetrate the intestinal wall, and enter the peritoneal cavity. They then penetrate the diaphragm and pleura and enter the lungs. The major target organs for the larvae are the lungs followed by the brain (12).
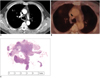
During the active phase of paragonimiasis, lung tissue surrounding the parasitic cysts may contain evidence of pneumonia, bronchitis, bronchiectasis, and fibrosis (12) (Fig. 7A). Watanabe et al. (11) reported one case of paragonimiasis mimicking lung cancer which showed high FDG uptake (SUV 4.7 at one hour post-injection, and elevation of SUV to 6.2 at two hours). Although the exact causes of FDG accumulation have not yet been proven, we can expect that inflammatory cells including eosinophlic infiltration, active inflammatory responses and viable worms cause high FDG uptake (Fig. 7B).
Other Infectious Conditions
In variable inflammatory conditions including abscesses (Fig. 8), glycolytic metabolism is elevated in the region of leukocytic infiltration associated with inflammatory processes, and consequently FDG uptake is elevated (2). Pneumocystis infections can also cause high FDG-uptake (Fig. 9). These conditions have not been well documented to date. However, in one report (13), patients with fever of unknown origin presented with high FDG uptake in PET imaging, finally proved to be infected by pneumocystis carinii pneumoniae. Inflammatory cells increase the expression of glucose transporters when they are activated, and multiple cytokines and growth factors can facilitate glucose transport without actually increasing the number of glucose transporters (5).
Radiation Fibrosis
Inflammatory processes in radiation fibrosis is caused by infiltration of leukocytes and macrophages and abnormal proliferation of type II pneumocytes, radiation-induced production of local cytokines such as platelet-derived growth factor, tumor necrosis factor, and transforming growth factor β in the radiation field are based on these inflammatory morphologic changes. Consequently, increased FDG uptake in the affected region would be expected (Fig. 10) (14).
Pneumoconiosis with Combined Massive Fibrosis
Pneumoconiosis is a tissue reaction to the presence of an accumulation of dust in the lungs. One clinicopathologic form of this reaction is fibrosis, while the other form consists of aggregates of particle-laden macrophages with minimal or no accompanying fibrosis, a reaction that is typically seen with inert dusts such as iron, tin, and barium (15) (Fig. 11). FDG-PET studies have revealed increased uptake in pneumoconiosis and progressive massive fibrosis. Some of this uptake is perhaps related to the presence of inflammatory cells such as macrophages, as well as fibroblasts (5).
Sclerosing Hemangioma
Sclerosing hemangioma is widely believed to arise from type II pneumocyte and bronchial epithelial lining. It is a benign lesion with a good prognosis. However, in some cases it shows local invasion, multiplicity and lymph node metastasis. The CT findings of scelrosing hemangiomas are well defined, round or oval shaped, enhanced mass with or without punctuate calcification. There has been only one case report of FDG-PET findings of sclerosing hemangioma, and in this report it shows intermediate FDG uptake (SUV= 3.0) (16) (Fig. 12).
Granulation Tissue around Tumors
Even within tumors, FDG uptake is not completely confined to the tumor cells themselves. The newly formed granulation tissue around the tumor and the macrophages infiltrating the marginal areas surrounding the necrotic area of the tumor show a high uptake of FDG. Some authors have suggested that about 24% of the FDG concentration in a tumor mass is derived from non-tumor tissue (17).
FALSE NEGATIVE CONDITIONS
Tumors with low activity are well-known major causes of false negative findings. This can be easily understood considering the FDG PET is metabolic imaging using the activity of lesion.
Another major cause of false negative findings for malignancy is tumor size. It is likely a result of a loss in measured activity as the nodule size diminishes due to the roughly 1-cm resolution of the PET systems frequently used (partial volume effect) (2).
Bronchioloalveolar Carcinoma (BAC)
Bronchioloalveolar carcinomas appear as areas of ground-glass opacity, nodules, masses, or areas of ground-glass opacity plus consolidation, on high-resolution CT scans. On pathologic examination, bronchioloalveolar carcinomas are well differentiated, having moderate degrees of nuclear atypism, mild degrees of mitotic figure, desmoplasia, and necrosis. These mild degrees of atypism, mitosis, and desmoplasia may be the causes of lower peak SUVs than those of other lung carcinomas. Several reports (18) have revealed lower FDG uptake in BAC than adenocarcinomas in the lungs. Thus, bronchioloalveolar carcinomas can be potential causes of false negative findings of malignancy on FDG PET scans (Fig. 13). Furthermore, mucinous bronchioloalveolar cell carcinomas, which often contain abundant mucin, exhibit significantly lower peak SUVs compared with those of squamous cell carcinomas, adenocarcinomas, and other cell types. In such cases, not only histologic grade, but also the amount of mucin component in the tumor (Fig. 14) is closely related with FDG-uptake (18).
Small Size Lesion
When lesions are smaller than 1 cm, these lesions may not show high FDG uptake in the lungs or mediastinum. This is the result of the 1-cm resolution of PET systems frequently used (partial volume effect) (2). Spatial resolution limitations of FDG PET have been shown to be the causative factor of false negative PET scans (Fig. 15).
Metastatic Lung Nodule of Extrapulmonary Neoplasm
Metastasis of tumors with a mucinous component can result in low FDG uptake (18). The relative cellularity of tumors is important in the detection of disease using FDG PET. Consequently, low cellularity in these tumors caused by the presence of mucin results in lower FDG uptake (19). For example, lung metastasis of a mucinous carcinoma of the breast (Fig. 16) may not show high FDG uptake. Other metastatic tumors such as mucinous adenocarcinomas of gastrointestinal origin can also show false negative findings in PET scans. Also, a metastatic mass from a renal cell carcinoma (20) (Fig. 17), and some invasive ductal and lobular breast carcinomas (21) are well reported to result in false negative findings.
Chemotherapy Related Factor
In several previous reports, it has been well documented that FDG uptake usually decreases after chemotherapy, and this correlates with therapeutic response. Decreased FDG uptake after irradiation is mainly due to the reduced number of metabolically active tumor cells. However, a decrease of FDG PET does not always predict a good response because FDG can differentiate metabolically active cells from dead cells, but cannot differentiate biologically viable from metabolically active cells (22) (Fig. 18).
Carcinoid Tumor
Carcinoid tumors arise from the dispersed neuroendocrine system, and are classified as typical and atypical, depending on the degree of cellular atypia. In a previous report, the SUV in a carcinoid tumor was 1.0-2.3, which is the result of low metabolic activity. The reason for the low metabolic activity in the carcinoid tumor is unknown (23).
Hyperglycemia
The biodistribution of FDG can be affected by blood glucose levels. In situations of high blood glucose levels, circulating blood glucose uptake in pathologic lesions increase and this prevents FDG uptake because of the competitive reaction (5). Therefore, a large amount of glucose in the blood is taken up in the tumor tissue which interferes FDG uptake in the tumor, resulting in a false negative finding. Specifically, in type II diabetic patients insulin may be used to manipulate glucose levels. However, there is still no agreement as to adjusting glucose levels in diabetic patients (2).
CONCLUSION
Metabolic imaging with FDG-PET is beginning to play important role in the management of oncologic diseases. In addition, it plays a complementary role in accurate overall evaluation of malignant diseases. However, false positive FDG uptake or false negative PET scans are frequently encountered. Proper interpretation and accurate characterization of an abnormality can be accomplished only if one is aware of possible false positive and negative conditions.












 XML Download
XML Download