

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The radiologic and clinical findings of foreign bodies in the chest of children are well recognized. Foreign bodies are infrequently found in adults, however, and the radiologic findings of these unusual circumstances have rarely been described. The causes of foreign bodies in adults are much more frequently iatrogenic or traumatic than is the case in children, and where the location is thoracic, the various nonspecific or unusual imaging features occasionally encountered may cause diagnostic problems. A familiarity with the radiologic features of these unusual circumstances can thus be helpful in the early and correct diagnosis of intrathoracic foreign bodies and the judicious management of the patients concerned. In this pictorial essay, we classify various thoracic foreign bodies into three types according to their causes, and illustrate radiologic findings and consequences of thoracic foreign bodies in adults.
Type I: ASPIRATION or INGESTION
Airway Foreign Bodies
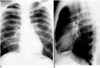
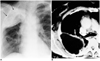
It is well known that foreign body aspiration is more common in children than in adults, its peak incidence occurring during the second year of life among children and during the sixth decade among adults (1-4). The many debilitating factors that predispose adults to foreign body aspiration include swallowing disorders and neuromuscular or neurologic disease (1-3). At presentation, the observed symptoms of aspirated foreign bodies do not differ according to the patient's age, though delay in diagnosis, the location of the body and radiographic images do differ between child and adult populations. The shorter time to diagnosis in children is almost certainly due in part to parental alertness but may also be related to the more central location of aspirated bodies in children. Indeed, aspirated foreign bodies lodged in the trachea are probably more prone to be symptomatic than those located in more peripheral airways (1). More than half of organic foreign bodies aspirated by children are peanuts, whereas a wide variety of aspirated foreign bodies, from bone fragments to metallic pins (Figs. 1, 2), are found in adults.
The most frequent symptom is the so-called "penetration syndrome," defined as the sudden onset of choking and intractable cough, with or without vomiting; other presenting symptoms that occur in isolation or in association are cough, fever, breathlessness and wheezing. Aspirated foreign bodies generally lodge in the right bronchial tree, especially the bronchus intermedius in adults, whereas in children a central location predominates (1, 2). Atelectasis is more common in adults, but air trapping is more common in children. In the acute setting the radiologic diagnosis of non-radiopaque foreign bodies in the lower airways relies on secondary findings such as air trapping or atelectasis. Bronchiectasis and bronchial stenoses are well-known late complications, so early diagnosis is mandatory.
In particular, since radiolucent foreign bodies show only secondary findings of airway obstruction such as air trapping or subsegmental atelectasis on chest radiographs, their presence must be strongly suspected if they are to be detected.
Esophageal Foreign Bodies
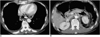
Adults, unlike children, rarely ingest foreign bodies, and most that are swallowed pass through the gastrointestinal tract without complication. Various foreign bodies such as food material can, however, lodge in the esophagus, and in such cases, chest radiography or CT can demonstrate the level of lodgement. The most common site of esophageal foreign bodies, and also the area from which foreign bodies are least likely to pass spontaneously, is the proximal esophagus at the thoracic inlet. Other common sites of lodgement include the level of the aortic arch or esophagogastric junction.
If diagnosis is delayed, foreign bodies lodged in the esophagus may cause perforation leading to serious complications such as mediastinitis. If esophageal perforation is suspected, CT can demonstrate pneumomediastinum, pneumothorax and pleural effusion, and can, in addition, identify mediastinal abscess and the site of rupture (Fig. 3).
Type II: TRAUMA or ACCIDENT
Thoracic Foreign Bodies due to Laceration
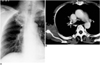
Foreign bodies may be observed anywhere in the chest as a result of accident or traumatic event. Penetrating wounds of the thorax caused by a knife, a fragment of glass (Fig. 4) or a bullet may induce pneumothorax (in 20% of such cases) or hemothorax (in 60-80%). Although there is usually evidence of penetrating thoracic trauma, significant internal injury may occur without obvious external thoracic injury. An injury that penetrates the lung may be associated with damage to other intrathoracic structures, which may be suggested by the clinical and imaging findings (1). Attention should thus be paid to the clinical history and mechanisms of injury, as well as to the radiologic findings. Interestingly, contrary to the general expectation that "nonleaded" glass is radiolucent, almost all types of glass are in fact radiopaque, and are frequently misinterpreted as metallic foreign bodies (Fig. 4B) (4). The presence of various kinds of foreign bodies has been reported in the radiologic literature, though to the best of our knowledge, the radiologic findings regarding wooden foreign bodies in the tracheobronchial tree have not been widely reported. Although metallic and other high-attenuation foreign bodies can easily be detected by CT, wooden foreign bodies usually appear as lesions of very low attenuation, seen on standard mediastinal window settings as similar in density to air. In order to differentiate wooden foreign bodies from air, a window width of up to 2000 HU is thus often necessary (Fig. 5).
Foreign Bodies due to Injury by Gun or Explosion
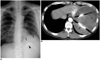
Penetrating wounds of the thorax caused by a gunshot or explosion are rare in Korea; most cases are related to injuries sustained during the Korean War. Complications associated with the presence of metallic foreign bodies in the thorax include atelectasis, obstructive pneumonitis (Fig. 6), and peumothorax or hemothorax. The delayed complication of calcific fibrothorax can occur as a result of previous hemothorax. A foreign body in the pleural cavity may cause chronic empyema, and malignant neoplasm associated with this condition and caused by a metallic foreign body has been reported in the literature (5).
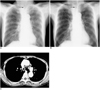
Intracardiac Foreign Bodies
Most reported intravascular or intracardiac foreign bodies are catheter fragments or broken guide wires, and may appear at any point along the course of venous return to the heart. The presence of most intravascular foreign bodies is connected to intravenous drug abuse, mental retardation or a suicide attempt, though iatrogenic insertion is also a possibility. An intracardiac metallic needle is rare, and is usually drug or suicide related (Fig. 7). To our knowledge, fewer than ten cases involving a needle in the heart have been reported in the recent medical literature, and the presence of a sewing needle in the right ventricle has not previously been reported in the radiology literature (6). We are unable to explain how it came to be present in this location. Retrieval using the snare and capture technique failed, and it was removed by open heart surgery.
Type III: IATROGENIC
Gauze Granuloma (Gossypiboma)
Gossypiboma, a term used to describe a mass within the body composed of a cotton matrix (usually a retained surgical sponge) is a very rare complication of thoracic surgery. The appearance of retained surgical sponges varies widely, and for their recognition, CT is very useful. Air trapped within a sponge gives rise to a characteristic -but unfortunately uncommon spongiform pattern. CT reveals a welldefined round mass with a thick wall and of heterogeneous internal density. The mass is usually wavy, striped and/or spotted, and mottled calcifications and gas bubbles may also occur within it (Figs. 8, 9). In these cases, the CT findings together with a history of previous surgery permit the correct preoperative diagnosis of retained surgical sponge (7). In any patient with an intrathoracic mass who has previously undergone thoracotomy, gossypiboma as well as hematoma, abscess formation and the recurrence of a primary tumor should be included in the differential diagnosis.
Complications related to Thoracic Plombage
The procedure involving the filling of the empty space remaining after lung resection is known as thoracic plombage, and prior to the early 1950s its use in the management of tuberculosis was common. Complications related to previous thoracic plombage are not uncommon. Various materials including paraffin wax, olive oil and polyethylene matrix were used as a filler for dead spaces and initial complications included pleural effusion and empyema related to local irritation caused by filling materials (Fig. 10). Delayed complications include recurrent local infection, bronchopleural fistula, and associated malignancy. Due to the high rate of early complications and assumed cancerogenicity, in a considerable number of cases the filling material was removed soon after its deployment. Subsequent treatment involved individualized management of the remaining space and muscle flap. Currently, thoracic plombage is rarely performed other than in cases of postpneumonectomy syndrome (8).
Gold Acupuncture Needle
Traditional Chinese acupuncture involves the insertion of multiple fine gold needles through the skin into the subcutaneous tissue (Fig. 11). The needle is cut off at the skin surface and left in the subcutaneous tissue for the life of the patient. Although this form of acupuncture is uncommon, it has been widely practiced in the Orient, and the multiple needles involved are usually discovered incidentally. Their appearance may mimic that of parasitic infections, but closer scrutiny reveals their uniform diameter and density, and thus that they are metallic (9). Although acupuncture is a generally simple and safe procedure, complications such as spinal cord injury, pneumothorax and cardiac tamponade may be associated.
Esophageal Speech Device
Tracheoesophageal voice has gradually evolved worldwide as a viable option for voice restoration following total laryngectomy (10). The standard procedural approach is seen to be the surgical creation of a tracheoesophageal fistula and the placement of an artificial voice device. Dysphonia can develop as a result of stenosis or loosening of the tracheoesophageal fistula, and on rare occasions the voice device may slip into the trachea. If this occurs, bronchoscopic removal is mandatory. Esophageal voice devices appear on chest radiographs as tubular radiopaque structures, and if follow-up radiography reveals a change in the location of a device, this suggests displacement into the esophagus or trachea (Fig. 12).
In summary, intrathoracic foreign bodies may occur in association with aspiration or penetrating trauma, or their origin may be iatrogenic. The causes of foreign bodies in adults are much more commonly iatrogenic or traumatic than in cases involving children. A familiarity with the radiologic features of these unusual circumstances can help achieve the early and correct diagnosis of intrathoracic foreign bodies and the judicious management of the patients concerned.






 XML Download
XML Download