

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A pneumocele of the frontal sinus is a rare disorder that can accompany a facial deformity. A pneumocele is characterized by the pathological expansion of the aerated sinus lined by normal mucosa. Pneumoceles most commonly affect the frontal sinus, followed in frequency by the sphenoid, ethmoid and maxillary sinuses (1). The etiology of a pneumocele is still unclear, but it might occur after head trauma, nasal polyposis, sinus surgery, chronic sinusitis and the formation of a tumor. We report a case of pneumocele of the frontal sinus and suggest that the pneumocele occurred after trauma to the head in a patient.
CASE REPORT
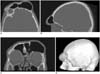
A 46-year-old man was admitted to our hospital with a 4-week history of headache and a growing mass on the left forehead. The patient had a history of severe head trauma due to a traffic accident that occurred 21 years prior. Over the intervening years, the patient had noticed a slowly growing mass on the left forehead. A physical examination demonstrated the presence of a hard mass, about 6×6 cm in size, on the left forehead. There were no abnormal findings after both a neurological and ophthalmological examination. Cranial multi-detector computed tomography (MDCT) was performed using a 64-MDCT unit (Aquilion 64; Toshiba, Tokyo, Japan) with a 0.5-mm- section width, a rotation time of 500 ms, tube voltage of 120 kV and tube current of 180 mA. The reconstructed images were processed, and multiplanar reformatted and three-dimensional (3D) volume-rendering (VR) images were processed on a separate workstation (Vitrea 2; Vital Images, Plymouth, MN). These images showed an abnormally expanded left frontal sinus with concurrent thinning of the bony wall (Figs. 1A-C). There was no sign of frontal bone fracture, despite the previous cranial trauma. Coronal reformatted MDCT images showed that the left frontal recess was obliterated with a soft tissue density. The other sinuses were normal. The 3D CT VR image showed an abnormal protrusion of the forehead due to a pneumocele of the frontal sinus (Fig. 1D). Surgical treatment was offered as an option for correcting the deformity but was refused by the patient.
DISCUSSION
A pneumocele is an uncommon condition that shows an abnormal enlargement of the paranasal sinuses. It is characterized by the focal or generalized thinning of the bony walls of the nasal sinuses as a result of pressure necrosis (2). Most pneumoceles are asymptomatic. In symptomatic cases, the common complaints are headache, a dull pain in the affected area, slowly progressing swelling and the presence of a facial deformity. Surgical nasoantral windowing can be carried out to decompress the sinus in symptomatic cases (2, 3). The clinical differential diagnosis of pneumocele includes mucoceles and both benign and malignant neoplasms of the paranasal sinuses. However, pneumoceles can be easily diagnosed with the use of CT that might show partial or total expansion of the sinus with concurrent thinning or erosion of the bony sinus wall. There are usually no signs of inflammation (4).
The word pneumocele is synonymously used with pneumosinus dilatans, pneumatocele, hyperpneumatization, sinus ectasia, sinus hypertrophy and aerocele. The abnormal enlargement of the sinuses can be classified into the following three types: a hyperpneumatized sinus, a pneumocele and pneumosinus dilatans (5). A hyperpneumatized sinus is characterized by the enlargement of a sinus without sign of either bony sinus-wall changes or extension of the sinus beyond its normal anatomic boundaries. Pneumocele refers to an abnormally enlarged sinus with thinning or erosion of the sinus walls. In this case, extension of the sinus beyond the normal boundaries is observed. The absence of thinning or destruction of the bony sinus walls distinguishes pneumosinus dilatans from a pneumocele.
A pneumocele lacks an established cause; nevertheless, several etiologies have been proposed. Infection by a gas-forming organism, spontaneous drainage of a mucocele, hormonal abnormalities and congenital factors have been proposed as possible factors that might have important roles in the pathogenesis of pneumoceles. Although the pathogenesis of pneumoceles is not completely understood, it has been proposed that increased sinus pressure caused by a one-way-valve obstruction of the nasofrontal duct could cause this condition. The one-way-valve, which can occur because of a possible physiologic block at the sinus ostium, allows air to enter into the sinus but prevents its return. Thus, persistent air entrapment elevates the pressure in the affected sinus. Other studies have described increased sinus pressure (4, 6). Urken et al. (5) have discussed the one-way-valve mechanism. At the same time, these investigators have been unable to formulate a possible etiology and pathogenesis for a pneumocele despite examining a large number of asymptomatic patients and six reported cases of pneumosinus dilatans. Our patient had no history of infection or neoplasm. The patient presented with a headache and progressive left frontal bossing after head trauma and soft tissue density had been observed at the left frontal recess on the coronal reformatted CT images. We believe that the left frontal pneumocele of our case was secondary to the previous head trauma, although the relationship between head trauma and the soft tissue of the frontal recess is not clear.
 XML Download
XML Download