

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
According to the World Health Organization classification of newborn infants by weight, an infant with a birth weight < 1,500 g is classified as a very low birth weight infant (VLBWI), and among them, an infant with a birth weight < 1,000 g is classified as an extremely low birth weight infant (ELBWI). The reason for using this classification is that VLBWIs and ELBWIs are high-risk infants belonging to early preterm infants and are at high risks of death. Therefore, the survival rate (SR) of VLBWIs and ELBWIs is generally analyzed as a criterion for determining the prognosis of survival of preterm infants.
The SR of VLBWIs in Korea was 33.8% in the 1960s, 43.2% in the 1970s, and 49.2% in the 1980s, which was significantly low (1). In Korea, the neonatal intensive care unit (NICU) was first established in the 1980s. During this period, full-scale NICU management using mechanical ventilator, monitoring system, ultrasonography, computed tomography, and magnetic resonance imaging for newborns began. Artificial pulmonary surfactants have been used since the 1990s, contributing greatly to the survival of infants with neonatal respiratory distress syndrome, the most common cause of premature death. In addition, NICU facilities and scales expanded nationwide. In the 2000s, various institutional improvements were made, including the use of high-frequency ventilator and inhaled nitric oxide, induction of therapeutic hypothermia, administration of drug and surgical treatment for patent ductus arteriosus, treatment for apnea, and insurance criteria for neonatal care (2). As a result, the SR of VLBWIs increased from 62.6% in the 1990s to 85.7% in 2009, and that of ELBWIs increased from 56.1% in 2002 to 71.3% in 2009, which has been a great progress (1).
The Korean Society of Neonatology and the Korean Center for Diseases Control and Prevention (KCDC) collaborated in the ongoing process of this development in Korea, and the need for a database to register and manage the nationwide VLBWIs born in Korea emerged. As a result, the Korean Neonatal Network (KNN) database system has been launched in 2013 (3,4). In overseas countries, registration system managements for VLBWIs have already been established, which improved the SRs of VLBWIs. The Vermont Oxford Network (VON) in the US started in 1988, Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Neonatal Research Network in 1986, Neonatal Research Network of Japan (NRNJ) in 1999, Australian and New Zealand Neonatal Network (ANZNN) in 1994, Canadian Neonatal Network (CNN) in 1995, and European Neonatal Network (EuroNeoNet, 16 countries in Europe) in 2003 (3). In Korea, the establishment of the KNN system was late; however, such an establishment (4) made a big turning point in the nationwide management of VLBWIs in Korea. The activities and objectives of the KNN are explained separately below.
This review is based on the SR of VLBWIs in the 2000s combined with the reports in 2002 (5), 2007 (6), and 2009 (1,7), and the results of the KNN annual reports in 2013 (8), 2014 (9), and 2015 (10) were the targets in the 2010s. We compared the SRs of VLBWIs and ELBWIs according to their birth weight and gestational period between the 2000s and 2010s to investigate whether their SRs improved after the establishment of the KNN. We also compared the rates in Korea in the 2010s with the recently published reports of overseas countries. We also reviewed the improvements in facilities and capacities, such as NICU beds, basic equipment, laboratory and therapy equipment, manpower, and support systems in the entire country in 2011 and 2015.
AN OVERVIEW OF THE KNN
The KNN, which is organized by the Korean Society of Neonatology and coordinated by the KCDC, was established in 2013 (3), and 69 out of 90 NICUs in Korea participated in this project; as of March 2017, the registration of a total of 8,996 VLBWIs is in progress (4). This is equivalent to –74% of 2,871 VLBWIs born as reported in the National Statistical Office in 2014. Thus, the KNN's VLBWIs registration program provides the representative data of Korea based on the total population of the country, so that this research based on these data may represent domestic neonatal results and treatment results. The KNN has a distinctive system that differentiates itself from foreign neonatal networks, such as real-time data input via web-based data, web-based real-time comparison of aggregate data, and individual institutional data (11); it also has a data quality maintenance system through queries by a central data manager, monitoring committee, and neonatologist's data monitoring through institutional direct visits 2 times a year (12) and provides education to participants through web-based programs and symposium by researchers, annual publication of reports to the entire and individual participating institutions, and web-based operations of ongoing research proposal systems (3).
The purposes and unique systems of the KNN are as follows: the mission of the KNN is to establish nationwide web-based registries to provide population-based national key data for planning appropriate health care policies for high-risk newborns. The KNN provides data-driven interactive tools for improving the quality of participating NICUs and an infrastructure to facilitate collaborative multicenter clinical studies. The KNN is able to reduce the socio-economic burden of extremely low birth rates in Korea and increase the effective economic population by establishing effective evidence-based strategies to increase the survival of and reduce complications in high-risk newborns. The KNN established data quality management, management system, and feedback system using real-time data display system, query generation, site visit monitoring, and annual reports as well as organization structure and web-based electronic case report form (e-CRF) registry. The KNN consists of a well-organized system for education and training for registration and research and an online application of data use and research proposals (3).
DATA COLLECTION
Data of the VLBWIs and ELBWIs in Korea in the 2000s
In the 2000s, a Korean nationwide survey was reported 3 times. In the first report, Park et al. (5) studied the SR of neonates among 1,842 live births of VLBWIs and 592 live births of ELBWIs from 62 hospitals in 2002. The second study, reported by Hahn et al. (6), included 2,030 live births of VLBWIs and 711 live births of ELBWIs from 57 hospitals in 2007. The third was a report by Chang and the Committee on Statistics of the Korean Society of Neonatology (7). In this study, 2,587 VLBWIs and 910 ELBWIs from 82 hospitals in 2009 were included, and the SR of the neonates was defined as the rate of neonates who survived to the time of discharge from the NICUs. A summary of the results of this third report was included in Hahn et al.'s report (1). In this review, the summary of the three reports was used as the data for the neonatal SRs of the VLBWIs and ELBWIs in Korea in the 2000s (Table 1).
Table 1
Number and SR of VLBWIs and ELBWIs in Korea in the 2000s and 2010s
Values are presented as number (SR). VLBWI, birth weight < 1,500 g; ELBWI, birth weight < 1,000 g. Comparison of the SRs between the total rates in the 2000s and 2010s in the VLBWI group (P < 0.001) and ELBWI group (P < 0.001) using the statistical program “R” (version 3.3.2; R Foundation, Vienna, Austria) and the method Pearson's χ2 test with Yates' continuity correction.
SR = survival rate, VLBWIs = very low birth weight infants, ELBWIs = extremely low birth weight infants, NICUs = neonatal intensive care units, KNN = Korean Neonatal Network.
Data of the VLBWIs and ELBWIs in Korea in the 2010s
The KNN started in 2013 and annually publishes its report. In these annual reports, we collect the data of VLBWIs reported in the corresponding year from the registered NICUs in Korea and publish the report. The important items of the report include basic information on newborn and parents, information on pregnancy and childbirth, information related to diseases, information related to discharge, etc. VLBWI SR items are classified by birth weight and gestational period in the discharge-related information. The birth weight is divided into < 400 g to 1,499 g, and the gestational period is divided into 20 to 37 weeks. In this study, the summary of the KNN Annual Reports in 2013 (8), 2014 (9), and 2015 (10) was used for the neonatal SRs of the VLBWIs and ELBWIs in the 2010s (Table 1).
Data of international comparison
We used data from the International Network for Evaluating Outcomes of Neonates (iNeo), a multinational collaboration between 9 high-resource countries (13,14), including the ANZNN (15), CNN (16), Israel Neonatal Network (INN) (17), NRNJ (18), Spanish Neonatal Network (19), Swedish Neonatal Quality Register (SNQ) (20), Swiss Neonatal Network (SwissNeoNet) (21), and United Kingdom Neonatal Collaborative (UKNC) (22).
According to Shim et al. (23), there is another recent comparison between the KNN reports from 2013 to June 2014 and the reports of other countries, and they used the data of the KNN (June 2013–2014) and the data of the NRNJ (2012) (24), VON (2009) (25), CNN (2013) (26), ANZNN (2012) (27), and EuroNeoNet (2012) (28). The data used for Taiwan were adapted from Su et al. (29), who reported on the classified comparison of the 1997–2001, 2002–2006, and 2007–2011 reports in Taiwan.
Comparison of the equipment, manpower, and support system in the NICUs in Korea between 2011 and 2015
We obtained information on equipment, manpower, and support systems in the NICUs in Korea in 2011 and 2015 from the report of Kim published in 2016 (30). We also compared the number, beds, and grading of NICUs nationwide around the start of the KNN.
NEONATAL SRs OF THE VLBWIs AND ELBWIs IN KOREA IN THE 2000s AND 2010s
Improvement in the neonatal SRs of the VLBWIs and ELBWIs after the establishment of the KNN (Comparison of the SRs of the VLBWIs and ELBWIs in Korea between the 2000s and 2010s by birth weight and gestational period)
Table 1 shows the comparison of the SRs of the VLBWIs and ELBWIs in Korea between the 2000s and 2010s. There was a significant increase of 83.0% in the 2000s and 85.8% in the 2010s in the VLBWIs (P < 0.001). There was a significant increase of 66.1% in the 2000s and 70.7% in the 2010s in the ELBWIs (P < 0.001). In other words, when the KNN started in 2013, the SRs of both VLBWIs and ELBWIs remarkably improved in the 2010s compared with those in the 2000s.
Table 2 shows the comparison of the neonatal SRs of the VLBWIs and ELBWIs by gestational period in Korea between 2009 and 2015. There was an improvement in the SR in the gestational period of one week. The SRs in all gestational periods significantly improved compared with the data from 2009 after the KNN was implemented.
Table 2
Comparison of the neonatal SRs by GP in Korea in 2009 and 2015
Neonatal SRs of the VLBWIs and ELBWIs by birth weight in Korea in the 2000s and 2010s
Table 3 shows the number of births and SRs of the VLBWIs and ELBWIs in Korea in the 2000s and 2010s. In terms of SR, 20.5%, 68.0%, and 91.8% had birth weights of < 500 g, 500–999 g, and 1,000–1,499 g in the 2000s, respectively, and 31.7%, 73.3%, and 95.2% in the 2010s, respectively, demonstrating an improvement.
Table 3
Neonatal SRs of the VLBWIs and ELBWIs by BW in Korea in the 2000s and 2010s
INTERNATIONAL COMPARISON OF NEONATAL SRs OF VLBWIs AND ELBWIs
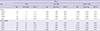
According to the recent reports by Shah et al. (13,14), an international database system of multinational collaboration called the iNeowas organized, which reported the VLBWI and ELBWI SRs in 9 countries in 2007–2010. Table 4 shows the data of the 9 high-resource countries: ANZNN (15), CNN (16), INN (17), NRNJ (18), Spanish Neonatal Network (19), SNQ (20), SwissNeoNet (21), and UKNC (22). The structure, design, and overall objectives of the iNeo have been reported elsewhere (13). Japan had a good SR of VLBWIs (95.0%), followed by Sweden (92.4%), Australia and New Zealand (91.5%), Canada (90.4%), Switzerland (89.8%), United Kingdom (England) (89.7%), Israel (86.1%), and Spain (83.1%). In Korea, the sum of the rates in 2013–2015 was 85.8%, and by 2015 alone, the rate was 86.4%, which was still in the level between England and Israel in comparison with this international group iNeo.
Table 4
International comparison of the neonatal outcomes of the VLBWIs by the iNeo
Data adapted from Shah et al. (14).
iNeo = International Network for Evaluating Outcomes of Neonates, VLBWIs = very low birth weight infants, SR = survival rate, ANZNN = Australian and New Zealand Neonatal Network, CNN = Canadian Neonatal Network, INN = Israel Neonatal Network, NRNJ = Neonatal Research Network of Japan, SEN1500 = Spanish Neonatal Network, SNQ = Swedish Neonatal Quality Register, SwissNeoNet = Swiss Neonatal Network, UKNC = United Kingdom Neonatal Collaborative.
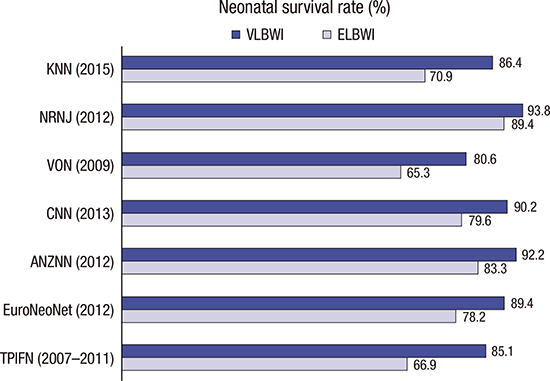
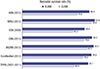
Shim et al. (23) reported Korea's SRs of VLBWIs and ELBWIs and compared the results of Korea in 2015, Japan in 2012 (24), the US in 2009 (25), Canada in 2013 (26), Australia and New Zealand in 2012 (27), and EuroNeoNet in 2012 (28). Fig. 1 shows the summary of the data from the KNN (10) in 2015 and Taiwan in 2007–2011 (29). Taiwan's national data were added here, and the SRs of the VLBWIs were 76.4%, 81.5%, and 85.1% in divisions of 1997–2001 (4,647), 2002–2006 (4,005), and 2007–2011 (4,507), respectively (29). As shown in Fig. 1, Japan had the highest SR of VLBWIs (93.8%), followed by Australia and New Zealand (92.2%), Canada (90.2%), Europe (89.4%), Korea (86.4%), Taiwan (85.1%), and the US (80.6%). Japan also had the highest SRs of ELBWIs (89.4%), followed by Australia and New Zealand (83.3%), Canada (79.6%), Europe (78.2%), Korea (70.9), Taiwan (66.9%), and the US (65.3%). In other words, the rates of both VLBWIs and ELBWIs in Korea were in between those in Europe and Taiwan. Such a finding shows that Korea should further develop their programs to reach the level of Japan, Australia and New Zealand, Canada, and Europe in the future.
Fig. 1
Comparison of the neonatal SRs of VLBWIs and ELBWIs between Korea, Japan, US, Canada, Europe, Australia and New Zealand, and Taiwan. Data adapted from Shim et al. (23).
SR = survival rate, VLBWIs = very low birth weight infants, ELBWIs = extremely low birth weight infants, KNN = Korean Neonatal Network (10), NRNJ = Neonatal Research Network of Japan (24), VON = Vermont Oxford Network (US; 25); CNN = Canadian Neonatal Network (26), ANZNN = Australian and New Zealand Neonatal Network (27), EuroNeoNet = European Neonatal Network (28), TPIFN = Taiwan Premature Infant Follow-up Network.
The reasons why Japan has the best results internationally are as follows. In Japan, neonatology was established as a specialty earlier than in Korea. Special medical care for premature infants started in 1958 and was supported by the government. The national action of supporting medical instruments for perinatal care and the regionalization of perinatal medicine was introduced in 1979. Starting in 1984, the national support for maternal-fetal intensive care units started, and additional supports for the medical expenses needed for perinatal medicine were achieved in 1986. These national projects continued to develop and included the organization of the Tertiary Central Perinatal Care Centers and Secondary Regional Perinatal Care Centers in 1996. This system regionalized perinatal and neonatal care and built an effective management system for the care of high-risk pregnancies and neonates. The highest SRs of VLBWIs and ELBWIs worldwide could be achieved using this perinatal care system. In addition, the patient information network is an important feature. The Japanese nationwide “Neonatal Research Network” was introduced in 1999. Another network called the “Perinatal Care Center Network” started in 2003. These 2 networks include all NICUs in Japan, which have excellent functions (1). The high level of Australia and New Zealand, Canada, and Europe is also the result of the efforts of the ANZNN, CNN, and EuroNeoNet, respectively. What is unusual is that the US has the lowest rates among these countries because of the presence of variable races and problems in the health care system.
IMPROVEMENT IN THE FACILITIES AND CAPACITIES IN NICUs AFTER THE ESTABLISHMENT OF THE KNN IN KOREA
Facilities and capacities in the NICUs in Korea in 2011 and 2015 with regard to the comparison of the equipment, manpower, support system such as parenteral nutritional support, dedicated neonatal pharmacist, neonatal sonography/echocardiography, extracorporeal membrane oxygenation, pediatric surgeon, etc. are shown in Table 5 (30). The number of NICUs nationwide was 89 in 2009 before the start of the KNN and the same in 2015. However, the number of beds increased from 1,299 to 1,716. The numbers of basic equipment, incubators, radiant warmers, ventilators, etc. have all increased. The increase in the number of high-frequency ventilator was especially remarkable. The use of nitric oxide, hypothermia, ultrasound, automated auditory brainstem response, and amplitude electroencephalography diagnostic equipment, which are important as the latest methods for inspection and treatment, also remarkably increased. There have also been some improvements in the support systems. As the most important developmental content, there is an increase in the number of manpower, including neonatology specialists, residents, nurses, and nurse specialists, corresponding to the increased number of beds. Currently, the NICUs in Korea are divided into NICU grading according to the number of patients and nurses. As of 2015, there were 61 grade 1 NICUs, 22 grade 2 NICUs, and 3 grade 3 NICUs in Korea. However, the number of beds in the NICUs in Korea is still insufficient compared to the number of births, which is especially concentrated in specific regions, and effective measures are needed for further improvements, according to Kim (30).
Table 5
Comparison of the facilities and capacities in the NICUs in Korea between 2011 and 2015

Data adapted from Kim (30). Nursing grade was determined by the ratio of number of bed to nurse in NICU (grade 1 < 1.0; grade 2 < 1.5; grade 3 < 2.0; grade 4 ≥ 2.0).
NICU = neonatal intensive care unit, ND = no data.
SUGGESTION AND CONCLUSION
Chang et al.'s study (3) emphasizes the following as the future of neonatology in Korea: continuous improvement in low birth rates and neonatal mortalities, regionalization and organization of the medical system in the perinatal area, establishment of data collection and development direction through the KNN nationwide, NICU quality improvement, evidence-based development in neonatology, treatment of premature infants near survival limits, development of new therapies for newborn and premature infant diseases, expansion of promising research fields, strengthening of database collection direction and simulation-based education in the neonatal area, neonatal development and family-centered nursing and treatment, establishment of follow-up care after discharge, etc.
To achieve this, the actions of the KNN are described as follows. If the collection and activities of domestic multi-purpose data through the KNN are continuously maintained and developed, improvement in the international quality of treatment and promotion of international clinical research through collaboration with the international networks of newborn infants in the future with NICU quality improvement activities and activation of clinical studies of multicenter newborns are expected. Based on the KNN, establishing the basis of internationalization through information exchanges with Japan and Taiwan that established a neonatal network in the Asian region sooner than Korea, complementing our system, and participating in the database of the iNeo (13,14) will be a good opportunity to improve the quality internationally.
As limitations of the present study, it is important to note that it was only possible to compare international SRs using official data that was shown in papers. Important factors such as quality of prenatal care and treatment protocol were not considered, and neither was variable national periviability, the limit of viability of the preterm infants. With active intervention, most infants born at 26 weeks and above have a high likelihood of survival, and virtually none below 22 weeks will survive, and SRs reported in a number studies demonstrated the rise of SR as gestational age increased from 22 to 25 weeks (32-34). Thus, SR, especially that of very preterm infants born below 26 weeks may vary due to different periviability by country and region.
The SRs of the VLBWIs and ELBWIs improved in the 2010s compared with those in the 2000s. The KNN's role established in 2013 contributed to this improvement. However, looking at Korea's SRs of VLBWIs and ELBWIs in 2015, they are still low compared with those of Japan, Australia and New Zealand, Canada, and Europe. To achieve better outcomes in Korea, it is necessary to establish and develop the abovementioned tasks.
 XML Download
XML Download