

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Disease can be classified into communicable disease, non-communicable disease, or injury, which has specific characteristics (1). Injury can occur via various mechanisms, such as, a transport-related accident, fall, drowning, fire, poisoning, or as a result of mechanical force (1), and injuries have different types of sequelae, such as, fracture, sprain, hemorrhage, burn, or laceration (2). Furthermore, injury is an important public health problem because it is the leading cause of death and is also related to severe disability (34). Globally, deaths from injuries were estimated at 4.092 million in 1990 and 5.073 million (a 30% increase) in 2010 (1). Besides, injury is preventable, and if this were achieved, premature deaths from unintentional injuries could be reduced by 39% and about 37,000 lives could be prolonged (5), which suggests injuries are better addressed as a separate problem.
The global burden of disease (GBD) study represented the foundation stone of assessing the burdens from diseases and injuries (67), and attempted to calculate comprehensive and comparable health losses associated with diseases. Burden of disease was estimated from years of life lost (YLLs) and years lived with disability (YLDs), and these were summed up to produce disability-adjusted life years (DALYs) (6). GBD data is useful for understanding health state, set priorities, and the evaluate effects of public health programs (89). It covers a wide range of diseases and regions, that is, up to 291 diseases and 21 regions. Furthermore, the GBD study has been used to evaluate national and sub-national burdens in some areas for policy makers and researchers (1011). However, the reliability of GBD study has been debated because of limited data and disability weight. Therefore, other researchers have been trying to obtain more reliable, elaborate findings using other data sources and methods (121314).
The purpose of this study was to estimate the national burden of injuries in Korea by injuries mechanism using more reliable data and disability weightings. We also explored the characteristics of its burden with respect to gender and age.
MATERIALS AND METHODS
Study design
This cross-sectional study involved an analysis of morbidity and mortality data related to injuries in South Korea in 2010. The incidences of injury-related deaths and hospital admissions were estimated for 2010 because data on hospital admissions for 2010 was the most recent available. Life expectancies were also calculated using mortality data for 2010 and YLLs were evaluated using age of injury-related death and life expectancy data. Burden of injuries was estimated for 2010 in units of DALY.
Participants
The study population was the people who admitted in hospital or died from external cause in 2010. The mortality and hospital admission data included diagnostic codes of the 5th Korean Classification of Diseases (KCD-5) based on the 10th revision of the International Classification of Disease (ICD-10). The study participants were defined and categorized according the mechanism of injuries, which was adopted from the classification of the GBD 2010 study (Supplementary Table 1).
No data was available for date of injury occurrence in death certificates. Therefore, some mortalities resulting from injuries suffered during 2009 may have been included, but on the other hand some injuries sustained in 2010 could have resulted in deaths in 2011. In the present study, we assumed that such gains and losses balanced each other. Regarding morbidity data, the Korean National Hospital Discharge Survey included date of injury and admission date. Date of injury was used to discriminate between the prevalence and incidence rates of injuries. An injury was considered an incident when dates of injury occurrence and hospital admission fell in 2010, whereas a case was considered as prevalent when injury occurred during the preceding year. Incident cases for 2010 were enrolled in this study, because the GBD 2010 study adopted an incident-based approach. In addition, we excluded in-hospital injuries that occurred during hospital stays.
Data source and measurement
We used morbidity data from the 7th Korean National Hospital Discharge Survey conducted by the Korean Center for Disease Control and Prevention (15). This survey sampled clusters of hospitals stratified by geographic location and number of beds in the first step. Hospitals with less than 100 beds and long-term care/rehabilitation hospitals were excluded. The number of the acute-care hospital sampled was 170. In the second step, approximately 9% of discharged patients were randomly sampled in hospitals with an electronic medical record system, whereas in hospitals with manual systems, 300–450 cases were retrieved according to bed numbers. Moreover, extraction rates depended on gender and age group. This representative data contained de-identified clinical information accessible to the public. The detailed sampling design used for the survey has been previous described (16). Weighting for the complex sample survey was considered when incidences of injured were estimated for YLD calculations.
Mortality data were obtained from the mortality records of the Korean National Statistical Office (17) from January 1 to December 31, 2010. Morbidity and mortality data were analyzed to estimate YLLs and YLDs, respectively, which were summed to obtain DALYs.
Variables
To calculate disease burden, incidences and mortalities of injury by mechanism were required for an incidence-based approach. There were up to two KCD-5 codes for mechanism of injury in hospital discharge survey data and one for mortality data. Numbers of injured were enumerated by injury mechanism and the classification of injury mechanisms was mutually exclusive. Most of the admitted patients had one mechanism code for injuries; only 0.99% of had two. Moreover, mortality data had only one diagnostic code for mechanism. Therefore, the incidence of injuries was essentially based on patient number, not on number of injuries, for the incidence-based approach. It is possible because the hospital survey was conducted using de-identified data that frequency included re-admissions.
Age and gender specific incidences of injury were estimated and corresponding mortalities were calculated. The weighted incidences of injuries were estimated for the whole population in Korea and for subpopulations based on gender (male and female) and age deciles (0-9, 10-11, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, ≥ 80), and the combination of gender and age groups. Duration of injuries and age at injury onset were estimated using Dismod II (18).
Statistical analysis
Using unique disability weightings, YLDs were estimated from injury incidences and durations and ages at injury onset. YLL was estimated using the formula for mortality and onset-age used in the GBD 2010 study and suggested in the overview of the Korean Burden of Disease Study 2012. After summing, burdens of injuries were calculated as DALYs per 1,000 in the registered population. The statistical analysis was performed using SAS version 9.3 (SAS Inc., Cary, NC, USA) and Dismod II version 1.04 (World Health Organization).
RESULTS
Table 1 shows the demographic findings of the study subjects. In morbidity and mortality data, total numbers of newly injured and those that succumbed to injury were 27,398 and 22,831, respectively, in 2010. The weighted frequency of newly injured was 831,240. Men were more likely to be involved in injuries than women, and those that died of injuries tended to be older. After weighting, around one third of the patients admitted to an acute-care hospital, claimed automobile insurance. The beneficiary of medical aid consisted of 5.2%. The most common locations of injuries were roads followed by homes. Of those that succumbed to injury 35.2% and 7.5% died hospital or on the way to hospital, respectively.
Table 1
Demographic characteristics of injured according to Korean morbidity and mortality data

Total injury burden in Korea was estimated at 1,581,072 DALYs in 2010, which corresponded to 3,170 per 100,000 (Table 2). This consisted of 604,361 YLLs and 976,712 YLDs. Males had nearly twice the burden (1,008,632) of females (572,440). From neonates to those in their twenties, injury burden increased from 992 to 4,070 per 100,000, and then stayed at over 3,000 through the 4th to 8th deciles and decreased to 2,639 for those over 80 years old.
Table 2
Estimated burdens of injuries in Korea by gender and age
Table 3 presents injury burden by mechanism which was categorized into 3 levels (higher, middle and lower level). All injuries were classified into higher-level (broad) classifications as: 1) transport injuries, 2) unintentional injuries other than transport injuries, 3) self harm and interpersonal violence, and 4) forces of nature, war, and legal intervention. These classes accounted for 35.5%, 39.8%, 24.3%, and 0.4%, respectively, of the total injury burden. These classes were further categorized into middle-level (detailed) classification which was further categorized into lower-level (most detailed) classification again. For instance, transport injuries were categorized into transport injuries by agricultural injuries and road injuries which were further categorized into pedestrian injury, pedal cycle injury, 2-wheeled motorized vehicle injury and etc. Among middle-level classification, the five highest ranking were road injuries (DALY: 546,477), falls (376,697), self harm (299,422), exposure to mechanical forces (91,406), and unclassified unintentional injuries (85,778). The road injuries involving a 3/4-wheeled motorized vehicle (347,832), a pedestrian (100,367), a 2-wheeled motorized vehicle (73,888) accounted for almost all (95.5%) road injuries in the lower-level classification.
Table 3
Estimated burdens of injuries by its mechanisms in Korea
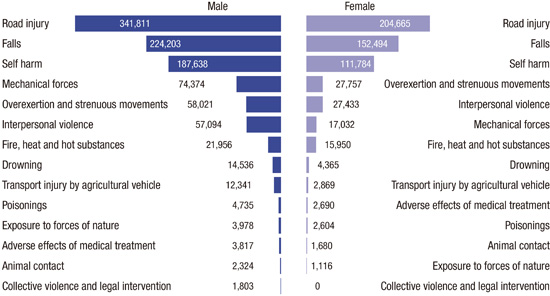
Differences between male and female injury burdens are shown in Fig. 1. Road injuries, falls, and self harm had the greatest disease burdens for males and females, and the 2nd and 3rd ranking were injuries from falls and self-harm. However, a difference between male and female rankings occurred from the 4th ranked item. Injuries from mechanical forces (4th rank) were more influential than the injuries from overexertion and strenuous movements (5th rank) and interpersonal violence (6th rank) in males. In contrast, the injuries from overexertion and strenuous movements (4th rank) were more influential than interpersonal violence (5th rank) and mechanical forces (6th rank) in females.

Contributions to injury burden by mechanism are presented in Fig. 2. Fig. 2A shows the total burden of injuries by age group, whereas Fig. 2B provides the estimates of injury burden per person based on numbers in the population in specific age groups. Fig. 2A shows an inverse V shape in injury burden which peaked in the forties. On the other hand, when analyzed by age group, those in their twenties had the heaviest burden per person and this burden declined slowly with age (Fig. 2B). In particular, road injuries decreased gradually from age 20. On the contrary, fall related injury in terms of injury burden per person increased rapidly from early adulthood.
Fig. 2
Disability-adjusted life years (DALYs) for injuries by age in Korea. (A) Shows the total injury burden by age group and (B) shows the injury burden per person after adjusting for the age-matched number in the general population.

Injury burden per person is visualized in gender and age groups (Fig. 3). Road-related injuries are ranked as 1st in the most of age groups. Fall and self-harm is the 2nd and 3nd ranking, respectively in males and females, although the exact ranking depends on the age group. Mechanical forces were not a common cause of injury burden in females, while it ranked 4th in males during physically and economically active period. Total DALYs among the age groups in males and females were suggested in Supplementary Tables 2 and 3.

DISCUSSION
This study presents incidence-based burden of injuries in Korea using nation-specific data and disability weightings. Korea had 1,581,072 DALYs from injuries (3,170 per 100,000). Males had almost twice the burden from injuries than females. In both genders, road-related injuries, falls, and self-harm ranked as 1st, 2nd, and 3rd with respect to burden of injury. Injury burden reached an obvious peak in the forties in the study population, while burden per person declined gradually from early adulthood.
Injuries have unique problems as compared with communicable and non-communicable diseases. Unlike diseases, injuries can be under-estimated when national health insurance data is used, because a substantial portion of transport and work-related injuries are covered by private or occupational insurance (1920). Furthermore, the mechanisms of injuries can be complex and multiple injury types can result from a single accident (21). Therefore, a reliable database for injuries is essential to estimate injury burdens and to understand how injuries occur (22). A high quality database containing data on diagnoses and mechanisms of injuries would provide a basis for such estimations.
Injury burden was estimated to be larger in the KBD than in the GBD country profile of 2010 (23). In the GBD 2010 country profile, the total burden was 1,286,733 DALYs, that is, 893,825 for males and 392,908 for females, and the total burden was 18.6% less than that found in the KBD study. Moreover, some differences were evident in the rankings of injury burdens determined by these two studies. Road injury, fall, self-harm, mechanical force, overexertion and strenuous movements, interpersonal violence, and fire were the top 7 ranked causes of injury burden in descending order in the present study. However, in the GBD 2010 study the order was self-harm, road injury, fall, mechanical force, drowning, interpersonal violence, and transport injury by agricultural vehicle.
There could be some explanation in the difference between this study and GBD 2010 study (1321). Difference was not suspected to come from classifications of types and sequelae because the classification of our study was the same as that of the GBD study to allow comparisons. However, in the GBD study, a prevalence-based approach was used and raw data, except for mortality data, was obtained from the South Korea Patient Survey (24). In this survey, de-identified inpatient and outpatient data, which contained one main diagnosis and one sub-diagnosis, was collected for one month (25). The study included an oriental clinic and convalescent hospital and was conducted to understand medical use in Korea. On contrast, the KBD study was performed using an incidence-based approach using the Korea National Hospital Discharge Survey data, which contained one main diagnosis, up to 20 sub-diagnoses and date of injury over a period of one year at acute-care hospitals. Therefore, the Korea National Hospital Discharge Survey was deemed to provide more reliable information on the incidence of injury, while the South Korea Patient Survey was considered to provide a good estimate of the prevalence of medical disease.
Different disability weights could also explain observed differences in injury burdens (1326). Disability weights were calculated using an online survey of Korean medical professionals, which allowed nation-specific disabilities to be produced and used to calculate injury burden. It has been suggested disability weights could be the main reason for different estimates of injury burden (26). As was found in the present study, other studies have reported that estimations of injury burden at the national level are considerably higher than the results of the GBD study (1326). In the UK, when disability weights and home-based cohort data were used, the national burden of injuries was calculated to be 2.6 fold higher (13). The authors suggested that the many assumptions made and data limitations could have been responsible for this discrepancy.
In one study, injury burden was compared among developed countries in the western pacific region (23). Regarding gross domestic product (GDP) per capita, Australia, Singapore and Japan reported higher GDPs ($67,473, $55,980 and $38,634, respectively) and China lower GDP ($6,992) than Korea ($25,998) (27). According to GBD 2013 study, total injury burdens reported were; Singapore 1,234 (1,080-1,415), Australia 1,780 (1,612-1,977), Japan 2,143 (1,875-2,430), Korea 2,577 (2,097-2,865), and China 2,603 (2,353-2,915) (28), which followed the GDP pattern. However, Korea had a much higher burden from self-harm (1,010) than Australia (475), Singapore (377), Japan (763), or China (313).
The implication of this KBD study was that we could estimate the national injury burden as more reliable value. Moreover, our study could provide to a more precise understanding of injury burden and enable the establishment of proper priorities for public health strategies and interventions. The strength of this study is that it provides a means of estimating more reliably the burdens of injuries in Korea. In this study, findings could be compared with the GBD study because it used the same classification and framework. Furthermore, reliable data and disability weights were used in the present study, which suggests results are dependable. However, it has a number of limitations. In particular, the burdens of minor injuries on outpatients and inpatients treated by hospitals with fewer than 100 beds were excluded, which suggests the possible under-estimation of injury burden (14). According to the Korean National Health and Nutrition Examination Survey, the numbers of patients treated at an outpatient clinic or admitted to hospital were 1,572 and 1,086 million, respectively, in 2010 (29). There is the other possibility of under-estimation of injury burden. The hospital survey was based on the discharge date and therefore the patient who got injured in 2010 and still admitted to 2011 was not included in the 2010 data. Furthermore, re-admissions were not discernible due to de-identification of the database, which indicates a possible over-estimation of injury burden, although this is not likely to be substantial because long-term care and rehabilitation hospitals were excluded. Finally, injury burden was estimated using 2010 data because this was the most recent Korean National Hospital Discharge Survey data available.
 XML Download
XML Download