

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recent evidence places more importance on chest compressions than ventilation in the resuscitation of victims with sudden cardiac arrest, even though both chest compressions and ventilation are mainstays of cardiopulmonary resuscitation (CPR) (123). Minimizing the interruption of chest compression, delivering high quality chest compressions, and increase in compression fraction are strongly associated with good resuscitation outcome (456). However, several determinants of chest compression to generate optimal hemodynamic effect, such as the optimal depth, rate, and hand placement position, remain unknown. Compression rate is a major determinant of cardiac output during CPR because only 1/3 of the stroke volume during spontaneous circulation is generated by each chest compression (7). Increasing compression rate can be an easy way to improve cardiac output during CPR. However, a very high compression rate might be associated with impaired coronary perfusion and/or decrease in cardiac output by reducing diastolic filling time (8).
During the recent 50 years of CPR history, the recommended chest compression rate has increased from 60 to 100 or at least 100 per minute (91011121314). The 2015 CPR guidelines recommend compression rate between 100 to 120 per minute during CPR without providing a specific compression rate (15). However, the effects of different chest compression rates during CPR on resuscitation outcome in humans have never been prospectively tested. Our primary objective of this study was to compare the efficacy of CPR with 120 compressions per minute (CPM) to CPR with 100 CPM in patients with non-traumatic out-of-hospital cardiac arrest.
MATERIALS AND METHODS
Study design and setting
This study was a multicenter, randomized, parallel-group, investigator-initiated, clinical trial to compare outcomes of cardiac arrest patients receiving CPR with 100 CPM or 120 CPM. A compression rate trial (COMPRATE trial) group was recruited to perform this study, and 12 university hospitals in Korea participated in the study.
Study population and randomization
Consecutive patients with non-traumatic out-of-hospital cardiac arrest admitted to the emergency department (ED) and who were aged 19 years or older were enrolled in the study. Exclusion criteria included cardiac arrest associated with exsanguination, terminal malignancy, aortic dissection, pulmonary thromboembolism, cardiac tamponade, congenital heart disease, or other chronic conditions such as bedridden status. We excluded patients after randomization based on information or patient status that existed before randomization but could not be determined before randomization because of the urgent need for treatment.
Patients were allocated to treatment groups according to the result from the opening of a sealed envelope by the attending emergency physician when the patient with cardiac arrest arrived at the ED. Patients were randomized to CPR with 100 CPM (CPR-100 group) or 120 CPM (CPR-120 group). Immediate caregivers were not blinded due to the nature of the study. However, physicians, neurologists, or healthcare professionals who provided continuous medical care after resuscitation or performed neurologic assessment were unaware of the intervention assignments.
Study protocol
To achieve adequate quality of chest compressions, certified BLS healthcare providers who participated in the study received a 2-hour training course using a manikin, a metronome, and a real-time CPR measurement feedback device (Q-CPR®, Phillips Healthcare, Seattle, WA, USA). CPR was performed according to AHA guidelines (13). The metronome was set at a rate of either 100 or 120 beats/min according to the randomization result. A defibrillator/monitor with a real-time CPR measurement feedback function (HeartStart MRx, Phillips Medical System) was used to maintain and analyze the quality of chest compressions. The optimal depth of chest compression was set to 5.5 cm. The compressor was also guided by a graphic display of compression depth, rate, and chest recoil determined from the monitor in order to maintain the quality of compressions. The compressor was rotated every two minutes.
After successful endotracheal intubation, an end-tidal carbon dioxide (ETCO2) monitoring probe (Microstream®, Phillips Medical System, Seattle, Washington, USA) was connected to the endotracheal tube. Ventilation was administered manually at a rate of 8−10 breaths/min with a volume of approximately one-third of a resuscitation bag (1.5 L) per breath. Defibrillation or administration of medication was performed by discretion of the attending emergency physician, if indicated. ETCO2 measurement was conducted five minutes after the beginning of resuscitation attempts. Peak and average values of ETCO2 were calculated from measurement of the first five consecutive ventilations.
Demographic data including pre-hospital and in-hospital variables were recorded in print and filed into the database. Data was sent twice a month from participating hospitals to the data monitoring committee. Two emergency physicians who were blinded to randomization assignments analyzed data acquired during CPR including the depth and rate of compression using a software package (Heartstart Event Review Pro® 4.1 Hospital Edition, Phillips Medical System, Seattle, Washington, USA).
Measures
The primary outcome measure was sustained restoration of spontaneous circulation (ROSC). Sustained ROSC was defined as a restored spontaneous circulation for longer than 20 consecutive minutes and persisting signs of circulation. The secondary outcome measures were survival and discharge from the hospital, one-month survival, and one-month survival with good functional status, categorized as a score of 2 or less on the cerebral performance category (CPC) (16).
Data analysis
Based on an average ROSC rate of 34% at the participating hospitals during the run-in period, a sample of 182 patients in each group was chosen to detect a 10% increase in the ROSC rate in the CPR-120 group compared to the CPR-100 group for providing a statistical power of 80% with a two-sided alpha value of 0.05, considering that, of all patients included in the study, 10% would be expected to have at least one of the exclusion criteria after enrollment in the study. Finally, a one-year study period was selected in consideration of annual visits of cardiac arrest patients to the participating hospitals. However, this planned sample size could not be obtained during the study period. The investigators decided to terminate the study without further extension of the study period in consideration of various situation of each participating institution.
The principal analyses of the trial were performed on the basis of a modified intention-to-treat basis with data from all randomly assigned patients except those who did not meet the inclusion criteria or those who were excluded. Differences in primary and secondary outcomes between the CPR-100 group and CPR-120 group were compared with χ2 test (Fisher's exact test). Continuous or categorical variables between the two groups were compared with a two-sample t-test or chi-square test (Fisher's exact test) as appropriate. Additional analyses were performed to compare the primary and secondary outcomes in subgroups of each group (Supplementary Tables). The relative predictions for primary outcome were quantified by odds ratio using binary logistic regression, which were presented as a forest plot. A P value less than 0.05 was considered statistically significant, and all statistical analyses were performed using SAS Ver. 9.2 (SAS Inc., NC, USA).
Ethic statement
The study protocol was approved by the institutional review board of Wonju Severance Christian Hospital (IRB No. CR311004) and each participating hospital. The institutional review board at 8 hospitals waived the requirement for written informed consent, while the institutional review board at the remaining 4 hospitals required written consent. At the hospitals where written consent was required, it was obtained after CPR from the next of kin. This trial was registered to Clinical Research Information Service, Korea (www.cris.nih.go.kr) (cris.nih.go.kr number: KCT0000231).
RESULTS
Enrollment and characteristic of the groups
Enrollment of the patients began in November 2011 and finished in December 2012. During the study period, 581 patients with out-of-hospital cardiac arrest presented to the ED of the participating hospitals. Among them, 111 patients (106 patients with traumatic cardiac arrests and 5 patients with death on arrival) were excluded before randomization. A total of 470 patients were randomized into two groups. Of these, 221 patients were assigned to the CPR-100 group, and 249 patients were assigned to the CPR-120 group. A total of 85 patients (38%) from the CPR-100 group and 93 patients (37%) from the CPR-120 group were excluded after randomization based on information or patient status that existed before randomization. Finally, a total of 136 patients (62%) in the CPR-100 group and 156 patients (63%) in the CPR-120 group were included in the analysis (Fig. 1).
Fig. 1
Patient inclusion and groups. DOA, death on arrival; CPR-100, CPR with 100 CPM (compression per minute); CPR-120, CPR with 120 CPM.

Baseline characteristics in terms of the events of cardiac arrest including age, sex, cause, witness of cardiac arrest, bystander CPR rate, initial ECG rhythm at ED, and time from collapse to ED arrival were not different between the two groups. In 81 (60%) patients of in the CPR-100 group and 113 (72%) patients in the CPR-120 group, full-time electronic data recorded during CPR were available for analysis. Compression depth was not different between the two groups (median, 55.7; interquartile range, 51.2–60.7 mm in the CPR-100 group; median, 57.8; interquartile range, 51.1–62.2 mm in the CPR-120 group, P = 0.647). The median compression rate was 101 CPM (interquartile range, 100–104 CPM) in the CPR-100 group and 118 CPM (interquartile range, 114–120 CPM) in the CPR-120 group (P < 0.001). The median chest compression fraction was 96.5% (interquartile range, 94.0%–98.2%) in the CPR-100 group and 95.5% (interquartile range, 93.2%–97.2%) in the CPR-120 group (P = 0.008). Mean ETCO2 was not different between the two groups (CPR-100 group, 25 ± 16 mmHg; CPR-120 group, 27 ± 15 mmHg, P = 0.370) (Table 1).
Table 1
Baseline characteristics of the patients included in the analysis

Comparison of primary and secondary outcomes
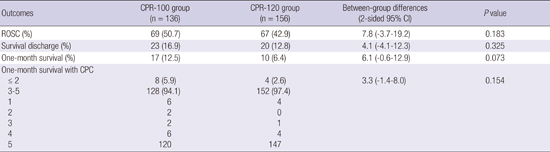
There were no statistical differences in primary and secondary outcomes between the two groups. In the comparison of primary outcome, 69 patients (50.7%) in the CPR-100 group and 67 patients (42.9%) in the CPR-120 group had ROSC (absolute difference, 7.8% points; 95% confidence interval [CI], -3.7 to 19.2%; P = 0.183). In the comparison of secondary outcomes, 23 patients (16.9%) in the CPR-100 group and 20 patients (12.8%) in the CPR-120 group were discharged alive from the hospital (absolute difference, 4.1% points; 95% CI, -4.1 to 12.3%, P = 0.325). A total of 17 patients (12.5%) in the CPR-100 group and 10 patients (6.4%) in the CPR-120 group had one-month survival (absolute difference, 6.1% points; 95% CI, -0.6 to 12.9%, P = 0.073). A total of eight patients (5.9%) in the CPR-100 group and four patients (2.6%) in the CPR-120 group had one-month survival with good neurological outcome, categorized as a score of 2 or less on the CPC (absolute difference, 3.3% points; 95% CI, -1.4 to 8.0%, P = 0.154) (Table 2).
Table 2
Primary and secondary outcomes of groups
CPR-100, CPR with 100 CPM (compression per minute); CPR-120, CPR with 120 CPM; ROSC, restoration of spontaneous circulation; CPC, cerebral performance category; CPC 1, good cerebral performance (conscious, alert, able to work, might have mild neurologic or psychological deficit); CPC 2, moderate cerebral disability (conscious, sufficient cerebral function for independent activities of daily life); CPC 3, severe cerebral disability (conscious, dependent on others for daily support because of impaired brain function); CPC 4, coma or vegetative state (any degree of coma without the presence of all brain death criteria, unawareness without interaction with environment, cerebral unresponsiveness); CPC 5, brain death.
Additional analyses
No strong evidence of subgroup differences was observed in primary outcome. However, we found a significant difference in the higher rate of ROSC with CPR-100 in male subgroup (OR, 0.54; 95% CI, 0.31-0.97) (Fig. 2)

DISCUSSION
This study is the first randomized clinical trial to test the efficacy of different compression rates in patients with out-of-hospital cardiac arrest. Our study demonstrates that, compared to CPR with 100 CPM, CPR with 120 CPM is not associated with improved resuscitation outcome as measured by the rate of sustained ROSC. We also found that there was no statistical difference between the two groups in secondary outcome measures including survival discharge, one-month survival, or one-month survival with favorable neurological outcome categorized by CPC 1 or 2. There was a statistically non-significant trend toward superiority of CPR with 100 CPM. This results suggest that CPR with 120 CPM has no additional beneficial effect over CPR with 100 CPM on resuscitation outcome measured.
It is unknown whether a specific compression rate during CPR is associated with improved resuscitation outcome in humans. Earlier investigations have suggested that a higher compression rate during CPR results in increased cardiac output. In an animal experiment, CPR with a faster compression rate up to 150 CPM produces a higher cardiac output than CPR with 60 or 100 CPM (17). However, coronary blood flow and cerebral blood flow were not different between CPR with a compression rate of 100 and with a rate of 150 CPM. The results of their study suggest that, with compression rates higher than 100 CPM, no additional increment in coronary or cerebral blood flow is expected, even though cardiac output increases. A small human study reported that, compared to CPR with 60 CPM, aortic pressure and coronary perfusion pressure increased significantly with CPR with 120 CPM (8). It has been demonstrated that compared with 60 CPM, CPR with 120 CPM produced significantly higher mean aortic pressure and coronary perfusion pressure, resulting in improved resuscitation outcome in dogs (18). On the other hand, an animal study reported that blood flow generated by manual chest compression is dependent upon the duration of compression, not the rate, when constant pressure is exerted on the sternum (19). Inconsistent findings from previous studies regarding the hemodynamic efficacy of different compression rates require further human studies in order to determine the optimal compression rate during CPR.
Chest compression rate is known to be associated with resuscitation outcome of cardiac arrest patients. In a prospective, cross-over trial including 23 cardiac arrest patients, CPR with 120 CPM generated higher end-tidal carbon dioxide tension than CPR with 80 CPM (20). However, it is not likely that the difference of 2 mmHg in end-tidal carbon dioxide tension observed in that study would result in different resuscitation outcomes. A prospective, observational study to assess the quality of chest compression reported that mean compression rate was higher in the ROSC group than in the group with no ROSC (90 vs. 79 CPM) when overall chest compression rate was suboptimal (4). Interestingly, the rate of chest compression (98 vs. 107 CPM) was not different between patients with and without ROSC when compression rate was within the optimal range. A retrospective analysis of CPR data revealed that ROSC rates peaked at 125 CPM, and a delivered compression rate less than 75 CPM was associated with a low rate of ROSC (21). However, there was no difference in ROSC rate when compression rates were categorized at < 80, 80-140, and > 140 CPM. A recent systemic review provided separate estimates for the relationship between chest compression rate and outcome. The study result revealed that survivors were significantly more likely to receive chest compression rates closer to the range of 85 to 100 CPM than non-survivors (22). A secondary observational analysis of the data from large multicenter clinical trials reported that the likelihood of survival was greatest in the group who received chest compression rate of 110-119 CPM among five groups based on the compression rate of less than 80, 80-99, 100-119, 120-139, and greater than or equal to 140 CPM with controlling for CPR quality metrics including compression depth (23).
The inconsistency of results from retrospective studies and meta-analysis points to the need for a prospective study to test the effects of different compression rates on resuscitation outcomes. In our study, we compared the resuscitation outcome of two different compression rates with controlling for compression depth with CPR feedback; 100 CPM was chosen as a standard method recommended by various guidelines, and 120 CPM was chosen because it has been reported to produce higher hemodynamic effect in previous reports and is recommended as an upper limit of compression rate by recent European guidelines (14). Results from our study indicate that a compression rate of 120 per minute during CPR is not associated with improvement in resuscitation outcome. Faster compression rates above 120 CPM might cause an adverse effect on coronary perfusion by reducing diastolic perfusion time decreased linearly with compression rate, even though cardiac output and diastolic aortic pressure increase (24). A faster compression rate is associated with rescuer fatigue and low quality of CPR (25). In this context and in light of our study results, 100 CPM is favored as an optimal compression rate during CPR.
Our study has limitations. The current study was underpowered to provide a definitive answer about the difference of ROSC between the two groups. The study did not reach to the number of patients targeted by sample size calculation. Even though the difference in ROSC between the two groups was not found, our results suggest that CPR with 120 CPM is not superior to the current standard CPR with 100 CPM. A larger sample size may find statistically significant difference between the two groups. Randomization and intervention in this study were performed in the ED instead of at initiation of pre-hospital resuscitation. In our emergency medical setting, every patient with out-of-hospital cardiac arrest is transferred to the ED after few minutes of standard CPR with 100 CPM at the scene because pre-hospital termination of resuscitation is not allowed. CPR occurred in the out-of-hospital setting may confound the results related to compression rates. The lack of pre-hospital CPR data and a prolonged time to randomization may be factors that need to be considered when applying our study results to clinical practice. Another concern is that we could not analyze CPR data obtained from all patients enrolled in this study. Full-time recording of CPR data was not available for analysis in 40% of the CPR-100 group and 28% of the CPR-120 group. However, the quality of compressions should have been maintained because the compressor performed CPR with the guidance of a metronome and the graphic display of compression depth and rate from the monitor and the attending physician encouraged them to follow this guidance.
In conclusion, no differences in the resuscitation outcomes were found between those who received CPR with a compression rate of 100/min and those who received CPR with a compression rate of 120/min in patients with out-of-hospital cardiac arrest resuscitated in ED. A large trial is warranted, with adequate power to confirm a statistically non-significant trend toward superiority of CPR with 100 CPM.
 XML Download
XML Download