

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Several studies in developed countries have reported a decreasing trend in hip fracture incidence (1234). However, studies in Korea showed a 2-fold increase in the total number of hip fractures, and the incidence rate of hip fracture in women increased steeply during a 10-year study period (5). Hip fractures in elderly patients are very serious because of high mortality, loss of independence, lower quality of life, and high socioeconomic burden (67). Although most risk factors such as aging, gender, and medical comorbidities are inevitable, aging is the most important risk factor for hip fractures; thus, identifying modifiable risk factors is extremely important.
To prevent falls and related fragility fractures, the role of muscles has been emphasized for maintaining functional performance. The mass and strength of skeletal muscles naturally decrease with age, and this loss accelerates after age 65, with a risk of adverse outcomes such as physical disability, poor quality of life, and death (1). This condition is called sarcopenia, which is characterized by decreased muscle mass and impaired muscle function (234).
Sarcopenia and osteoporosis have become increasingly significant as the population of older people increases, and are clinically very important and common pathological states. In skeletal tissues, muscle and bone interact mechanically and functionally (4). Therefore, aging and various pathological states influence muscle and bone simultaneously. Sarcopenia is considered an indicator of the development of frailty (8) and loss of independence in the elderly. Furthermore, this condition is associated with increased physical disability, resulting in a risk of falls (6). However, the impact of sarcopenia on osteoporotic fractures has rarely been reported.
The purpose of this study was to 1) evaluate anthropometric characteristics related to hip fracture in Korean patients, 2) investigate sarcopenia prevalence in hip fracture (HF) and non-hip fracture (NF) groups, and 3) investigate the correlation between sarcopenia and osteoporosis.
MATERIALS AND METHODS
Patients
Between November 2011 and December 2014, fresh hip fracture patients (≥50 years) were eligible and assigned to the HF group. Exclusion criteria were inability to perform whole-body dual energy X-ray absorptiometry (DXA). Body composition and whole bone mineral density (BMD) were assessed using DXA (DPX-NT; GE Medical Systems Lunar, Madison, WI, USA).
During the study period, 424 hip fracture patients aged 50 years and older were admitted to the study institution. Of these, 34 (8.1%) were excluded because there was no time to perform DXA preoperatively due to the need for urgent surgical repair, and 31 (7.3%) were excluded because of lack of informed consent.
The final study population of 359 participants in the HF group (272 females, 78.3 ± 9.8 years; 87 males, 75.3 ± 8.6 years) did not differ significantly from nonparticipants with regard to age, sex, height, or body weight (Table 1).
Table 1
Characteristics of participants, body composition and skeletal muscle mass index in both females and males
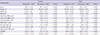
As a control, we used data from KNHANES IV-2008. Of a total 10,589 who participated in KNHANES IV-2008, 2,816 population were selected aged over 50 years and measured BMD by DXA (QDR 4500A, Hologic Inc., Waltham, MA, USA). Of these, 1,202 were excluded from the study because they received only lumbar or hip DXA and lacked data for whole-body DXA. Finally, 1,614 patients (950 females, 64.1 ± 9.1 years; 664 males, 63.3 ± 8.8 years) underwent whole-body DXA and were assigned to the NF group (Table 1).
Anthropometric measurements
Body composition was measured by whole-body DXA (DPX-NT; GE Medical Systems Lunar, Madison, WI, USA). Bone mineral content, fat mass, and lean soft tissue mass were measured separately for each part of the body, including the arms and legs. The lean soft tissue masses of the arms and legs were nearly equal to the skeletal muscle mass. As absolute muscle mass correlates with height, the skeletal muscle mass index (SMI) was calculated by the following formula: lean mass/height2(kg/m2), which is directly analogous to body mass index (BMI: weight/height2[kg/m2]). Arm SMI was defined as (arm lean mass/height2[kg/m2]). Leg SMI was defined as (leg lean mass/height2[kg/m2]). Appendicular SMI was defined as the sum of the arm and leg SMI.
Sarcopenia was defined according to the criteria for the Asia Working Group for Sarcopenia (AWGS) (SMI below 5.4 kg/m2 in women and below 7.0 kg/m2 in men) (7) and European Working Group on Sarcopenia in Older people (EWGSOP) (SMI below 5.5 kg/m2 in women and below 7.26 kg/m2 in men).
We simultaneously measured whole body BMD, including the lumbar spine, by DXA for all participants in the study. Osteoporosis was defined as a BMD 2.5 standard deviations (SD) below the peak bone mass of a young, healthy, gender- and race-matched reference population according to the World Health Organization (WHO) diagnostic classification.
Biochemical analyses
In the HF group, detailed information on the 25-hydroxyvitamin D (25(OH)D) assay was provided previously (9). Serum 25(OH)D levels were determined with a radioimmunoassay kit (DiaSorin, Stillwater, MN, USA).
In the NF (control) group, serum 25(OH)D and parathyroid hormone (PTH) levels were measured using a gamma counter (1470 Wizard; Perkin Elmer, Turku, Finland) and LIAISON (DiaSorin) with radioimmunoassay (25(OH)D 125I RIA Kit; DiaSorin) and chemiluminescence immunoassay (N-tact PTH Assay kit; DiaSorin), respectively.
Statistical analysis
We used Student’s t-test to compare characteristics in the study groups. To compare the prevalence of sarcopenia, we used the χ2 test. To find a significant relationship between appendicular SMI and BMD, Pearson’s correlation was carried out in each group. We evaluated the appendicular SMI value for continuous variables by using a general linear model for control, with covariates of age and sex. The general linear model is a generalization of a multiple linear regression model in the case of more than one dependent variable.
Prevalence of sarcopenia was calculated in 4 age groups (ages less than 70, 70 to 74, 75 to 80, and more than 80 years). The Mantel–Haenszel method was used for testing significance for age- and gender-adjusted prevalence of sarcopenia. To determine the presence of sarcopenia as an independent variable in predicting the occurrence of hip fracture selected as a dependent variable, we used the stepwise multiple logistic regression model. The regression model also included the patient characteristics of age, sex, whole body BMD, weight, and height, which are known to be key predictors of skeletal muscle mass.
The strength of association of the chosen variables and the occurrence of hip fracture were reported as the odds ratio (OR) and 95% confidence interval (CI) compared to a reference group. Statistical analyses were carried out using SPSS for Windows software (version 22.0; SPSS, Chicago, IL, USA). A P value of < 0.05 was considered significant.
Ethics statement
The study design and protocol were approved by the institutional review board of the Chung-Ang University Hospital, CAUH-IRB No. c2016048(1785). Written informed consent was waived all patients involved in this study. The use of Korea National Health and Nutrition Examination Survey (KNHANES) data was reviewed and approved by the ethics committee of the Korea Centers for Disease Control and Prevention (KCDC) (2011-02CON-21-C).
RESULTS
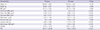
In the HF group, using the AWGS definition, the prevalence of sarcopenia in women and men was 44.3% and 68.2%, respectively; in the NF group, it was 7.1% and 16.1%, respectively. Sarcopenia prevalence was significantly higher in both men and women in the HF group than in the NF group (Table 2). When compared by age distribution, all age groups of women in the HF group had significantly higher prevalence of sarcopenia than the NF groups. The HF group of men aged less than 75 years had higher prevalence of sarcopenia than the NF group (P < 0.001). However, men aged more than 75 years did not have significantly different prevalence of sarcopenia in either group.
Table 2
Prevalence of sarcopenia in both women and men from each age group

In the HF group, using EWGSOP criteria, the prevalence of sarcopenia in women and men was 47.1% and 80.5%, respectively; in the NF group, it was 9.9% and 22.4%, respectively.
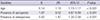
After adjusting for differences in age and the ratio of females in the HF and NF groups, general linear model analysis was used to compare the characteristics, body composition, and SMI of patients in both study groups (Table 3). No significant differences were observed for height, weight, and BMI after controlling for age and gender. Whole-body lean mass, BMD, and PTH were significantly lower in the HF group than in the NF group (P < 0.001). However, 25(OH)D was not significantly different between the HF and NF groups (P = 0.238).
Table 3
Comparison of characteristics of patients between two groups after adjusting age and gender
A stepwise logistic regression analysis was carried out to identify predictive factors for the occurrence of a hip fracture. We found that older age, sarcopenia, and osteoporosis were significant factors for the occurrence of a hip fracture (OR = 1.15, OR = 6.52, OR = 1.87; P < 0.001, P < 0.001 and P < 0.001, respectively) (Table 4). There was no significant correlation between appendicular SMI and whole-body BMD in the HF (P = 0.194, P = 0.323, P = 0.585, respectively). However, there was a positive correlation between appendicular SMI and whole-body BMD in the NF group (R = 0.13, P < 0.001; R = 0.12, P < 0.001; R = 0.12, P < 0.001, respectively) (Fig. 1A-F).
Table 4
Stepwise logistic regression analysis for hip fracture
| Variables | B | OR | 95% CI | P value |
|---|---|---|---|---|
| Age | 0.14 | 1.15 | 1.13-1.17 | < 0.001 |
| Presence of sarcopenia | 1.87 | 6.52 | 4.67-9.09 | < 0.001 |
| Presence of osteoporosis | 0.62 | 1.87 | 1.35-2.58 | < 0.001 |
Fig. 1
Correlation of appendicular skeletal muscle mass index (SMI) and femur bone mineral density (BMD). (A) The hip fracture (HF) group. (B) The non-fracture (NF) group.
Correlation of appendicular SMI and femur neck BMD in (C) the HF group and (D) the NF group. Correlation of appendicular SMI and spine BMD in (E) the HF group and (F) the NF group.

DISCUSSION
Sarcopenia and osteoporosis have similar pathophysiology and are important risk factors for fragility fractures (410). Hip fracture is especially significant in disability and frailty, and is known to be related to high mortality, decreased activities of daily living, and increased socioeconomic burden in elderly patients (1112). The present study evaluated the prevalence of sarcopenia in patients with hip fractures diagnosed by DXA after hip fracture occurrence, and was defined using AWGS criteria. This case-control study showed that the prevalence of sarcopenia and osteoporosis in patients with hip fracture was 6.5 and 1.8 times, respectively, more common than in controls. However, in the HF group, there was no significant correlation between appendicular SMI and whole-body BMD (P = 0.194, P = 0.323, P = 0.585, respectively).
This study showed that the prevalence of sarcopenia in women and men in the HF group was 44.3% and 68.2%, respectively. Hida et al. (13) reported that the prevalence of sarcopenia in hip fracture patients based on Japanese criteria (appendicular SMI < 5.46 kg/m2 in women, < 6.87 kg/m2 in men) was 44.7% in women and 81.1% in men. Di Monaco et al. (14) reported that the prevalence of sarcopenia in patients with hip fracture based on the New Mexico Elder Health Survey (height adjusted appendicular SMI < 2 SD in a young reference group) was 64% in women and 95% in men. These findings did not correspond with another study, in which Gonzalez et al. (15) evaluated the prevalence of sarcopenia in 479 patients with hip fracture. They reported that the prevalence of sarcopenia was 17.1% (12.4% in men, 18.3% in women) using the EWGSOP definition. This prevalence of sarcopenia in the Gonzalez study is lower than in other studies by 3 to 4 times. The reason for these differences in prevalence is mainly due to use of different criteria. Nevertheless, despite these different definitions, the prevalence of sarcopenia in men is higher than in women (Table 5).
Table 5
Summaries of studies of sarcopenia in patients with hip fracture

| Authors (reference) | Study design | Regions | Population | Mean age (yr) | Definition | Cut-off of muscle mass (appendicular muscle kg/ht2) by DXA | Prevalence (%) |
|---|---|---|---|---|---|---|---|
| Hida, 2013 (13) | Case-control | Japan | 357:2511 | 82.7(F), 80.3(M) | Japanese criteria | 6.87(M), 5.46(F) | 81.1(M), 44.7(F) |
| Di Monaco, 2012 (14) | Case series | Italy | 591 | 79.7 | New Mexico Elder Health Survey | < 2 SD in a young reference group | 95(M), 64(F) |
| Gonzalez, 2015 (15) | Case series | Spain | 479 | 78.3(F), 75.3(M) | EWGOSP | < 2 SD in a young reference group | 12.4(M), 18.3(F) |
| Present study, 2016 | Case-control | Korea | 359:1614 | 78.3(F), 75.3(M) | AWGS | 7.0(M), 5.4(F) | 68.2(M), 44.3(F) |
| EWGOSP | < 2 SD in a young reference group | 80.5(M), 47.1(F) |
Patients with hip fractures had lower serum 25(OH)D levels in this study. However, we could not identify a relationship between sarcopenia and serum 25(OH)D levels. Gumieiro et al. (16) evaluated the association between serum levels of 25(OH)D3 with mid-upper arm muscle circumference, handgrip strength, and length of hospital stay in 102 patients with hip fracture. They reported that serum levels of 25(OH)D3 were related to muscle strength rather than mass. In longitudinal observational studies, lower serum levels of vitamin D were associated with significantly decreased skeletal muscle mass during follow-up. Liu et al. (17) performed a community-based study on vitamin D levels and skeletal muscle mass in 568 patients. They measured 25(OH)D3 and appendicular SMI at baseline and 6 years later, and reported that appendicular SMI was significantly decreased in the group with lower 25(OH)D3. However, we did not measure muscle strength and it was impossible to confirm a correlation with serum 25(OH)D3. Therefore, a prospective follow-up study is necessary to evaluate the effect of vitamin D on sarcopenia.
As a causal factor of the occurrence of hip fracture in multivariate analysis in this study, the OR of sarcopenia was 3.5-fold higher than that of osteoporosis in patients with hip fracture. This finding demonstrates that sarcopenia is a greater risk factor in patients with hip fracture. This corresponds to another study, in which Hida et al. (13) reported that the presence of sarcopenia (P = 0.02), older age (P < 0.001), and lower whole-body BMD (P < 0.001) were significant risk factors for hip fracture in elderly patients. However, in evaluating the relationship between sarcopenia and osteoporosis in the HF group, there was no significant correlation between appendicular SMI and whole-body BMD. Hida et al. (13) reported the same results. They found no significant correlation in the HF group (P = 0.257) between appendicular SMI and whole-body BMD.
There were several limitations. First, this study was cross-sectional and retrospective. Therefore, selection bias might be inevitable. To overcome this, we designed a case-control study and found significant differences between the HF and NF groups. Second, there could be errors in measured values because the whole-body DXA machines used for the patient group were different from those used for the control group. Hologic conversion formula is adjusting with Lunar data only for BMD data of spine and hip in two different devices (18). However, lean body mass and other site were not established conversion formula between two devices. Therefore, direct conversion is impossible and further studies are necessary to develop conversion formula for whole body DXA data between two devices. Finally, comparison with other studies is very limited due to different definitions of sarcopenia. However, the AWGS recently suggested guidelines for Asian populations. It is possible to compare results with other studies in Asians. However, no standardization has been made of body composition for Korean patients.
In conclusion, the present study showed a higher prevalence of sarcopenia and osteoporosis in patients with hip fractures compared with normal populations, and that sarcopenia prevalence is higher in men. Further study is needed to confirm the association with sarcopenia in patients with hip fracture.
 XML Download
XML Download