

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Benign biliary stricture (BBS) is a common and challenging clinical problem (1). Endoscopic placement of biliary stents, which is considered first-line therapy, provides the highest long-term biliary patency rate (2). However, endoscopic management of BBS remains challenging. The main drawback of endoscopic treatment is the need for multiple procedures over one-year treatment period, which increases costs and may decrease patient compliance (34). Therefore, there is a growing interest and need for the development of new devices that are able to mitigate the disadvantages of performing endoscopic treatment. Accordingly, there is a demand for a proper animal model to evaluate the efficacy of endoscopic devices.
As of now, there is no reliable BBS animal model. Previous studies of BBS models have mostly been used for surgical experiments with small animals, but the process of making a BBS model was cumbersome and laborious (567). In addition, small animal models tend not to be suitable for endoscopic experiments due to the minute size of the digestive tract. The lack of a proper large animal model can lead to errors in clinical application of new medical devices in humans. Therefore, it is necessary to develop a simple and reproducible method for making a BBS large animal model that is similar to actual clinical situations.
Radiofrequency ablation (RFA) therapy has been found to be safe and effective in several gastrointestinal disorders (89). RFA can deliver heat energy to tissue that results in necrosis around the RFA probe, and eventually stricture can be induced around tissue damaged by thermal energy (10). RFA has an extended range of indication in experiments because the procedure is not technically difficult to apply, and it is easy to control the degree of thermal energy emitted by an RFA device (9). Most recently, endobiliary application of RFA has been developed, and the efficacy of this usage was reported in a pilot clinical study (11). With this reference point, we decided to conduct a study using endoscopic RFA to develop a large animal model of BBS.
The aims of the current study were to develop a large animal model of BBS using endobiliary RFA and to investigate an effective and safe energy option for application in producing bile duct stricture.
MATERIALS AND METHODS
Animals
Fourteen-month-old female mini pigs (Sus scrofa), each weighing approximately 30 kg, were purchased from Medi Kinetics Co. Ltd. (Pyeongtaek, Korea) to be used for an in vivo experimental study. The animals were kept in specific pathogen-free animal facilities with complete substrate feeding, according to standard guidelines for laboratory animals. All animals were quarantined and acclimated in a vivarium for one week prior to the start of the experiments.
Equipment and instruments
An endobiliary RFA catheter (9 F, 230-cm working length; APRO Korea Inc., Gunpo, Korea) was used for the study. This catheter is a disposable, monopolar device suitable for endoluminal delivery of RFA into the biliary tree over a 0.035-inch guidewire. The distal end of the RFA catheter has a 10-mm leading tip, proximal to which there is a 10-mm steel electrode. Energy was delivered by an RFA generator (CoATherm RF-G200; APRO Korea Inc.) operating at 480 kHz and the range of the used power output was 60 to 100 W at 80°C for 60 seconds (Fig. 1).
Fig. 1
The endobiliary radiofrequency catheter (APRO Korea Inc., Gunpo, Korea) and power generator (CoATherm RF-G200; APRO Korea Inc.) used for endobiliary RFA. (A) An endobiliary RFA catheter. (B) The distal end of the RFA catheter has a 10-mm leading tip, proximal to which there is a 10-mm steel electrode. (C) An RFA generator.

Pre-procedure preparation
All animals fasted overnight and were given only water for 24 hours before the endoscopic procedure was conducted. Animals were pre-medicated with an intramuscular injection of atropine sulfate (0.04 mg/kg), xylazine (2 mg/kg), and tiletamine-zolazepam (5 mg/kg). After endotracheal intubation, 0.5% to 2.0% isoflurane was administered with 70% nitrous oxide, and 30% oxygen was given via a ventilator to maintain general anesthesia. The animals were placed in the left lateral decubitus position on a fluoroscopy table and allocated randomly to three groups (60, 80, and 100 W) according to the electrical power level.
Endoscopic procedure
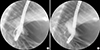
An expert biliary endoscopist (S. J.) performed endoscopic retrograde cholangiography (ERC) on 12 swine using a standard side-viewing duodenoscope (TJF-240; Olympus Optical Co. Ltd., Tokyo, Japan). After duodenal intubation of the scope, a diagnostic cannula (ERCP catheter, bottle-shaped metal tip; MTW-Endoskopie, Wesel, Germany) was inserted into the bile duct using the wire-guided cannulation technique with a 0.035-inch hydrophilic-tipped guidewire (Boston Scientific Corporation, Natick, MA, USA) to obtain the cholangiogram. The endobiliary RFA catheter advanced into the distal common bile duct (CBD) over the guidewire under fluoroscopic guidance (Fig. 2). Endoscopic biliary sphincterotomy was not required for insertion of the RFA catheter because, unlike humans, swine do not have sphincter of Oddi in major duodenal papilla, and the papillary orifice is patulous and wide. RFA applications were performed with power settings of 60, 80, and 100 W for 60 seconds.
Post-procedure follow-up and pathology assessment
During the four weeks following the procedure, the animals were fed their usual diet. Clinical signs and parameters including weight loss, daily food intake, and demeanor score were monitored daily. Biochemical tests of liver function were assessed at baseline and two weeks after the procedure. ERC was repeated two and four weeks after the endobiliary RFA to identify the bile duct stricture and procedure-related adverse events. Bile duct stricture was defined if the luminal diameter decreased by more than 50% of the baseline. When the bile duct perforation was identified in a follow-up cholangiogram, the animal was sacrificed by potassium chloride overdose immediately, and the bile duct was achieved to evaluate pathologic findings. With the exception of cases of bile duct perforation, animals were sacrificed six weeks after the procedure. Laparotomy was performed to evaluate presence of bile duct stricture. The CBD was identified and removed, and the effects of RFA on the distal CBD were assessed macroscopically during necropsy. Histological examination of the CBD was subsequently performed for all animals.
RESULTS
Endobiliary RFA and clinical follow-up
Endobiliary RFA of the CBD was successfully performed on all 12 swine. No technical difficulties or adverse events were encountered during the procedures. No clinical signs of acute cholangitis (e.g., fever, weight loss, decreased daily food intake) were noted in any animal two weeks after the procedure was completed. However, a large amount of pus was gushing out of the major duodenal papilla during follow-up ERC in all animals, so that the occurrence of acute cholangitis was suspected. Laboratory tests also indicated cholestasis. Median values of the liver profiles were as follows: total bilirubin, 4.4 mg/dL (range, 0.2–7.9); alkaline phosphatase, 360 IU/L (188–1078); gamma-glutamyl transpeptidase, 92 IU/L (56–150); asparatate aminotransferase, 162 IU/L (20–840); alanin aminotransperase, 31 IU/L (20–70). On the follow-up ERC two weeks after the procedure, a segmental bile duct stricture was observed in all animals (Fig. 3A) (Table 1). Before the main experiment, pilot study using energy dosages of 80 W and 100 W for each mini-pig was performed to evaluate the effect and adverse event of RFA. Bile duct perforation was observed in pig that received the 100 W dosage of RFA, but those of 80 W did not occurred bile duct perforation on ERC 2 weeks after RFA. As the results of pilot study, further experimental procedures using 100 W were discontinued because of an ethical problem. We decided to modify the study that the pigs initially allocated to 100 W group were reclassified to 80 W group (Supplementary Fig. 1).
Fig. 3
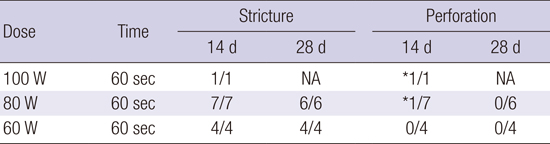
Endoscopic retrograde cholangiograms after endobiliary RFA. (A) Cholangiogram at two weeks after endobiliary RFA showing stricture at site of procedure. (B) Cholangiogram at four weeks after endobiliary RFA. The silhouette of the stricture proximal margin is more apparent and proximal duct dilatation has progressed.
Table 1
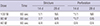
Results of endobiliary radiofrequency ablation in a swine model*
| Dose | Time | Stricture | Perforation | ||
|---|---|---|---|---|---|
| 14 d | 28 d | 14 d | 28 d | ||
| 100 W | 60 sec | 1/1 | NA | *1/1 | NA |
| 80 W | 60 sec | 7/7 | 6/6 | *1/7 | 0/6 |
| 60 W | 60 sec | 4/4 | 4/4 | 0/4 | 0/4 |
Finally, bile duct perforations were observed in two animals (1/1 [100%] for 100 W; 1/7 [14.3%] for 80 W) on ERC two weeks after the procedure; these animals were sacrificed immediately to investigate pathologic progression. Bile duct perforation was not observed in the 60 W group (n = 4, 0%).
Biliary irrigation with normal saline and pus aspiration were performed for treatment of acute cholangitis in the remaining pigs, and follow-up ERC was performed four weeks after the initial procedure. On ERC review, the silhouette of a stricture of proximal margin was more apparent and proximal duct dilatation had progressed (Fig. 3B). Bile duct perforation was no longer apparent.
Macroscopic and microscopic assessment
On the macroscopic examination of extracted CBD, the CBD had filled with yellowish sludge. In addition, there was a fibrous band at the level of stricture (distal CBD) and diffuse reddish mucosal inflammation on the proximal part of the CBD. No signs of other damage to the surrounding CBD were found. In the animals that experienced perforation, bile duct perforation with abscess formation was noted at the level of stricture.
Microscopic findings of CBD specimens in all animals, including perforation cases, demonstrated severe periductal fibrosis and luminal obliteration with transmural inflammation. These microscopic findings did not show significant difference according to the dose of thermal energy. The CBD, which was proximal to the stricture segment, maintained normal mucosa and muscular structure, but the lumen was markedly dilated (Fig. 4).
Fig. 4
Photomicrographs of a histologic section of bile duct with endobiliary RFA at a 60 W setting. (A) The distal part of the CBD, which is embedded in the duodenal muscle layer, reveals mild mucosal inflammation without ulcer or stricture in representative pathologic findings from the swine bile duct (H&E; original magnification 40 ×). (B) The muscle layer of distal CBD is well preserved (MT; original magnification 40 ×). (C) The RFA area of the CBD shows luminal obliteration with mucosal ulcer and transmural inflammation (H&E; original magnification 40 ×). (D) The RFA area shows destruction of muscle layer with transmural inflammation and severe fibrosis (MT; original magnification 40 ×). (E) The lumen of the proximal part of the CBD is markedly dilated. Mucosa is intact without ulcer (H&E; original magnification 12.5 ×). (F) The proximal CBD shows attenuated muscle layer (MT; original magnification 12.5 ×).

DISCUSSION
The current study demonstrated that the thermal energy induced by RFA was effective in producing bile duct stricture. A significant stricture was seen in the CBD of all animals, supporting the efficacy of endobiliary RFA for creating stricture. The results of our experiments are in agreement with previously published data. Thermal energy generated by a heat probe or a multipolar electro-cautery probe was evaluated by Rumalla et al. (12) in an animal study with nine swine that was designed to develop a BBS model of the CBD. In their study, 6 of 7 heat probe treatments and 1 of 6 multipolar probe treatments resulted in stricture. This led the authors to report that the application of intraluminal thermal injury can result in a reproducible animal model of BBS; the application of a heat probe at 15 J produced bile duct stenosis in all animals. In addition, the investigators found that strictures tend to develop more effectively as the dose of thermal energy increases (> 10 J).
On the basis of these results, we planned to begin our endoscopic experiment with a higher level of energy power to improve the success rate of creating a BBS model. However, higher electrical power is accompanied by a high risk of bile duct perforation. Our results showed that the occurrence of CBD perforation strongly correlated with the amount of thermal energy exposure. The safest thermal energy option to develop a BBS model was 60 W for 60 seconds; the risk of bile duct perforation increases when energy beyond this level is applied. The current study used a monopolar RFA electrode, which is commonly used in the treatment of hepatocellular carcinoma (HCC) and different from the contact thermal devices used in previous relevant studies. Thermal energy options for the management of HCC range from 6 to 120 W for 6 to 12 minutes (13). Therefore, we applied electrical power of 100 W for 60 seconds to the first animal to adjust the risk of bile duct perforation and determine the threshold to create biliary stricture at the beginning of this study. The biliary stricture in this animal was formed properly, but perforation was detected two weeks after the procedure. Subsequently, the doses of electrical power were decreased sequentially down to 60 W in the other animals. All animals that received 60 W for 60 seconds survived at the end of study without bile duct perforation. In terms of the ability to create biliary stricture, this thermal energy option yielded satisfactory results. On the serial cholangiograms two and four weeks after the procedure, a tight biliary stricture with dilated proximal bile duct was confirmed in all four animals that treated with this thermal energy option. Moreover, severe fibrosis was observed at the site of injury and luminal obliteration was found on microscopic examination of CBD specimens. Therefore, we estimated that the optimal thermal energy option for creating a BBS model using RFA would be 60 W for 60 seconds. This finding will be of great benefit for future studies in that it should reduce unnecessary failure and improve the yield rate in making a BBS model.
The basic mechanism for creating BBS in this study was thermal injury. The RF waves passing through the electrode agitated tissue ions around the electrode, thus increasing the temperature by frictional heat and resulting in destruction of the normal bile duct wall located close to the electrode (14). Thereafter, biliary stricture gradually developed during the healing process. Although the mechanism for induction of biliary stricture in the current study differs from those associated with other causes of BBS (15), the histologic features of this BBS model are similar to cases of BBS in patients with concentric periductal fibrosis and luminal obliteration. The histologic features we encountered are typical end-result findings detected in BBS (16). Therefore, we estimated that our stricture model is a proper animal model that can substitute for BBS in humans, and hopefully be helpful in the development of new device, technology, or treatment strategies. However, this BBS model would not be applicable to investigate adverse events resulting from biliary endoscopy procedures. The biliary system of swine has relatively few differences from that of humans. One difference is that the biliary system of swine is not combined with the pancreatic duct. It enters the wall of the duodenal bulb right below the pylorus, and is separated from the main pancreatic duct. Thus, adverse events related to the procedure, such as post-procedure pancreatitis, cannot occur in this BBS model. To cope with this factor, another BBS model using other species will be required.
The current animal model has several advantages compared with previous BBS models. Most importantly, the high thermal energy of endobiliary RFA used in the current study is easily reproducible, stable, and has a high success rate with little injury to the animal subjects. To this date, surgical approaches such as ligation, clamping, or electro-thermal injury of the CBD have been mainly used to create a BBS animal model (1718). Although these surgical approaches yielded satisfactory results in creating strictures, they require complicated preparation and postoperative care and sometimes lead to mortality of the animal, whereas establishment of a model using endobiliary RFA is straightforward and safe. All endoscopic procedures can be performed without technical difficulty within 20 minutes, and all animal subjects that underwent 60 W-RFA survived without serious adverse events until the end of the experiment. Furthermore, strictures of the CBD in all animals were found and the degree of stricture was satisfactory upon pathological examination. The second advantage of the current animal model is that the condition of the stricture in large animals is similar to the clinical manifestations seen in human patients with BBS, thus allowing surgeons to practice endoscopic therapeutic techniques or conduct preclinical experiments prior to working with humans.
The primary limitation of this study was the short observation time. Although RFA- induced bile duct strictures were maintained for four weeks in the current study, it is uncertain whether this model could be used for long-term observation experiments of therapeutic devices. These strictures have to be preserved without spontaneous improvement for a long time in order to investigate the therapeutic effect of various devices. However, the aim of our study was to establish a simple and reproducible method for making an animal model of BBS. A further long-term follow-up study will be needed to determine the long-term durability of stricture.
In conclusion, we developed a swine model of bile duct stricture using endobiliary RFA. The endobiliary RFA with proper energy settings appears to be a feasible and safe method to create a BBS model.
 XML Download
XML Download