

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The outcomes of childhood cancer have improved in recent decades, and the number of long-term survivors of childhood cancer is expected to increase significantly in the future. Survivors of childhood cancer are at increased risk for the development of various late events, among which second malignant neoplasms (SMNs) are among the most serious. SMNs are the second most common cause of mortality among 5-year survivors of childhood cancer, behind only recurrence of the primary malignant neoplasm (PMN) (1).
Several large cohort studies have shown that the risk of developing an SMN increases 3- to 10-fold among childhood cancer survivors compared with the general population (2345). The Childhood Cancer Survivor Study (CCSS), the largest cohort study of childhood cancer survivors to date, reported a cumulative risk of developing SMN of 3.2% at 20 years and 9.3% at 30 years of follow-up (6). Racial and ethnic differences can affect the epidemiology and outcomes of both SMN and PMN. Indeed, large study groups, such as the CCSS, British Childhood Cancer Survivor Study Group (BCCSS), and Nordic cohort, have reported outcomes of childhood cancer survivors with SMNs from western countries (456). However, no well-organized, comprehensive cohort of childhood cancer survivors has been reported for populations in Asia. Additionally, data about SMNs in childhood cancer survivors are scarce in Korea. Although a previous retrospective study reported the outcomes of patients with SMNs from 6 institutions in Korea between 1981 and 1997, only a small number of patients with a limited spectrum of disease were enrolled for that analysis (7).
Our present study aimed to further extend that previous study by investigating the clinical characteristics and outcomes of SMNs in survivors of childhood cancer who were retrospectively surveyed from multiple institutions in Korea. Our findings are expected to provide baseline data for future cohort studies.
MATERIALS AND METHODS
Design and patients
A multicenter, retrospective questionnaire survey on SMNs was conducted after the treatment of childhood cancers. Questionnaires were sent to 26 member hospitals of the Korean Society of Pediatric Hematology-Oncology and responses were received from 14 hospitals (54%). Patients were registered if the PMN was diagnosed prior to the age of 21 years and if they had received chemotherapy with or without radiotherapy. SMN was defined as a new neoplasm that developed after the primary cancer, not including the recurrence of the PMN. A total of 102 patients from 11 hospitals who were diagnosed with a PMN between 1998 and 2011 were eligible for our present analyses.
The case report form recorded demographic characteristics (sex, age, and cancer predisposition syndrome), and data about the PMN (histological diagnosis and sites of primary and metastatic disease), treatments (chemotherapy, radiotherapy, surgical procedures, and hematopoietic stem cell transplantation [HSCT]), and about the SMN (date of diagnosis, histological type, site, extent of disease, therapy, and outcome).
Statistical analysis
The Student t-test was used to compare differences between parametric variables. The Mann–Whitney U test was used to compare non-parametric data. The Kaplan–Meier method was used to estimate survival probabilities. A threshold of P < 0.05 was set for statistical significance. All statistical analyses were performed using SPSS version 21.0 (Statistical Package for the Social Sciences; Chicago, IL, USA).
RESULTS
Demographic data
The median patient age at the diagnosis of SMN was 12.7 years (range, 2.5–29.4 years) and at the diagnosis of PMN was 6.6 years (range, 0–19.7 years). Fourteen patients (13.7%) were older than 20 years at the diagnosis of SMNs. The overall male-to-female ratio was 1.22:1. The median follow-up period was 8.6 years (range, 1.2–27.5 years). The study cohort included 6 patients (6%) with cancer predisposition syndrome, 4 patients with bilateral retinoblastoma (including those who subsequently developed osteosarcoma [2 cases], juvenile myelomonocytic leukemia [1 case], and mesenchymal sarcoma [1 case]), 1 patient with neurofibromatosis type 1 (who had a malignant peripheral nerve sheath tumor as the PMN and subsequently developed therapy-related acute myeloid leukemia [AML]), and 1 patient with Li-Fraumeni syndrome (who had rhabdomyosarcoma as the PMN and subsequently developed anaplastic astrocytoma).
Characteristics of the PMNs and SMNs
Table 1 presents the distribution of PMNs and SMNs. The most common PMNs were central nervous system (CNS) tumors (n = 17; 9 with medulloblastoma, 3 with germ cell tumors, 5 with others), followed by acute lymphoblastic leukemia (ALL; n = 16), non-Hodgkin lymphoma (NHL; n = 13), and osteosarcoma (n = 12). The most common SMNs were therapy-related myeloid neoplasms (t-MNs) (29 cases of AML and 12 cases of myelodysplastic syndrome [MDS]; 40.2%), followed by thyroid carcinoma (n = 15; 14.7%), CNS tumors (n = 10; 9.8%), and osteosarcoma (n = 8; 7.8%).
Table 1
Second malignant neoplasms in the study patients with the indicated primary malignant neoplasm
ACC, adrenocortical carcinoma; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; BAL, biphenotypic acute leukemia; CCSK, clear cell sarcoma of kidney; CNS, central nervous system; EFT, Ewing family tumors; GCT, germ cell tumors; HBL, hepatoblastoma; HL, Hodgkin lymphoma; LCH, Langerhans cell histiocytosis; NBL, neuroblastoma; NHL, Non-Hodgkin lymphoma; OSA, osteosarcoma; PPB, pleuropulmonary blastoma; RBL; retinoblastoma; RMS, rhabdomyosarcoma; STS, soft tissue sarcoma.
For the common types of SMN, the most frequent type of PMNs in patients with t-MNs (n = 41) were osteosarcoma (n = 10) and CNS tumors (n = 9). For patients with second thyroid carcinoma (n = 15), there was no preference for the preceding type of PMN. For patients with second CNS tumors (n = 10), the most common PMNs were ALL (n = 4) and other CNS tumors (n = 3). The most common combination was t-MNs after either osteosarcoma (n = 9) or CNS tumors (n = 9).
The median interval between diagnosis of the PMN and SMN was 4.9 years (range, 0.5–18.5 years). The interval was shortest for AML (median, 2.8 years; range, 0.5–13.4 years) and MDS (median, 2.7 years; range, 1.7–8.4 years) as the SMN, and was longer for solid tumors, such as osteosarcoma (median, 6.3 years; range, 3.6–14.8 years), thyroid cancer (median, 6.8 years; range, 4.1–18.5 years), and CNS tumors (median, 9.3 years; range, 1.9–12.6 years; Fig. 1). The mean interval was shorter for second hematologic malignancies (3.9 years) compared with second solid tumors (8.7 years; P = 0.020).
Fig. 1
The latency period between the diagnosis of primary and second malignant neoplasms.
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; CNS, central nervous system; MDS, myelodysplastic syndrome.

Among 41 patients with t-MNs, 23 patients had received a median cumulative etoposide dose of 2,377 mg/m2 (range, 334-4,837 mg/m2) for their PMNs, 21 patients a median doxorubicin-equivalent cumulative dose of 291 mg/m2 (range, 35-451 mg/m2), 16 patients a median cumulative cyclophosphamide dose of 9,040 mg/m2 (range, 689-26,727 mg/m2), 18 patients a median cumulative ifosfamide dose of 52,593 mg/m2 (range, 2,320-147,170), 17 patients a median cumulative cisplatin dose of 293 mg/m2 (range, 85-835 mg/m2), and 13 patients a median cumulative carboplatin dose of 4,125 mg/m2 (range, 1,252-10,411 mg/m2). In addition to chemotherapy, sixteen patients had received craniospinal (n = 7) or focal (n = 9) irradiation for their PMNs.
Cytogenetic abnormalities in t-MDS included combined chromosome 7 and 5 abnormalities (n = 3), chromosome 7 abnormalities (n = 3), complex karyotypes (n = 2), and other abnormalities (n = 4). For therapy-related AML (t-AML; n = 29), cytogenetic abnormalities included 11q23 translocations (n = 13), a normal karyotype (n = 5), complex karyotypes (n = 4), t(8;21) (n = 1), and t(15;17) (n = 1).
The most common histological subtypes of second thyroid carcinoma (n = 15) were papillary carcinoma (n = 9), followed by follicular (n = 4), poorly differentiated (n = 1), and undifferentiated (n = 1) carcinoma. The histological subtypes of second CNS tumors (n = 10) were as follows: 2 embryonal tumors (1 medulloblastoma and 1 supratentorial primitive neuroectodermal tumor [PNET]), 2 low-grade gliomas (1 oligodendroglioma and 1 pilocytic astrocytoma of the optic pathways), and 5 high-grade gliomas (3 glioblastoma, 1 anaplastic astrocytoma, and 1 anaplastic oligodendroglioma), and 1 brainstem glioma.
SMNs after radiation therapy
Among 45 patients with a second solid tumor, 15 (33%) were reported to have developed this SMN in a previous radiation field (Table 2). The most frequent SMNs after radiation therapy were CNS tumors (n = 5) and thyroid carcinoma (n = 5), followed by osteosarcoma (n = 2), and others (n = 3). Indications of radiation treatment for PMN in second CNS tumors included prophylactic cranial radiation in 3 patients (1 case with NHL and 2 cases with ALL) and therapeutic craniospinal radiation in 2 cases with primary CNS tumors. For patients with second thyroid carcinoma, PMN was Hodgkin lymphoma in 2, ALL in 1, neuroblastoma in 1, and rhabdomyosarcoma in 1. Five of 10 subsequent CNS tumors (50%) developed after prior radiation therapy, 5 of 15 subsequent thyroid carcinomas (33%) and 2 of 8 subsequent osteosarcomas (25%). The median latency period of solid tumors after radiation therapy was 9.5 years (range, 5.3–14.0 years), while that of solid tumors not associated with radiation was 8.0 years (range, 1.1–18.5 years; P = 0.134). The median latency periods for CNS tumors and thyroid carcinoma after radiation therapy were 10.3 years (range, 8.6–12.6 years) and 9.5 years (range, 5.7–13.3 years), respectively, whereas those of CNS tumors and thyroid carcinoma that were not associated with radiation were 8.8 years (range, 1.9–9.6 years) and 6.5 years (range, 4.1–18.5 years), respectively (P = 0.095 and 0.371).
Table 2
Characteristics of radiation-associated second malignant neoplasms
SMNs after HSCT
A total of 20 patients among the patients with SMNs had been received HSCT before, including 17 patients after high-dose chemotherapy with autologous stem cell transplantation (HDCT/ASCT) and 3 patients after allogeneic HSCT. The most frequent SMN following HDCT/ASCT was AML (n = 7), followed by thyroid carcinoma (n = 4), non-thyroid carcinoma (n = 2), osteosarcoma (n = 1), rhabdomyosarcoma (n = 1), and other soft tissue sarcomas (n = 2). Among 4 patients with thyroid carcinoma, 1 patient had received total body irradiation as a component of preparative regimen for HDCT/ASCT. The SMNs following allogeneic HSCT included AML (n = 1), MDS (n = 1), and squamous cell carcinoma (n = 1).
Outcomes of SMNs
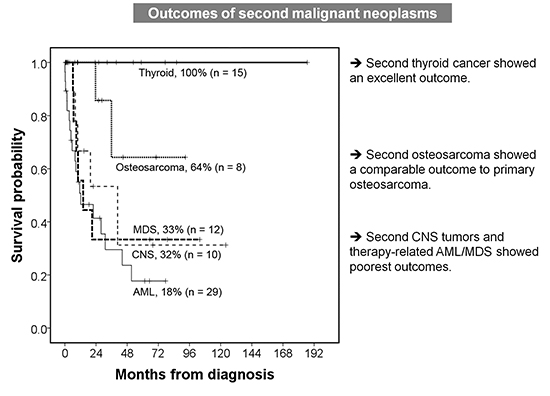
The 5-year overall survival (OS) rate of patients with an SMN was 45% (Fig. 2A) with a median follow-up time of 8.6 years. The 5-year OS rates of patients with common types of SMN, including AML, MDS, CNS tumors, osteosarcoma, and thyroid carcinoma, were 18%, 33%, 32%, 64%, and 100%, respectively (Fig. 2B).
Fig. 2
Survival outcomes of the patients with second malignant neoplasm. (A) The 5-year overall survival rates of patients with second malignant neoplasms. (B) The 5-year overall survival rates of patients with AML, MDS, CNS tumors, osteosarcoma, and thyroid carcinoma.
AML, acute myeloid leukemia; CNS, central nervous system; MDS, myelodysplastic syndrome.

For therapy-related MDS (t-MDS; n = 12), 5 patients had early MDS (refractory anemia in 2 cases, MDS associated with isolated del(5q) in 1 case, and unclassifiable in 2 cases) and 7 patients had advanced MDS (refractory anemia with excess blasts [RAEB]-1 in 1 case, RAEB-2 in 4 cases, and RAEB in transformation in 1 case). The 5-year OS rates of patients with early and advanced MDS were 50% and 20%, respectively. The 5-year OS rates for the patients who received allogeneic HSCT for t-AML (n = 14) and t-MDS (n = 6) were 35% and 40%, respectively, while those for the patients with t-AML (n = 15) and t-MDS (n = 6) who did not were 0% and 25%.
For second thyroid carcinomas (n = 15), all of the patients for whom treatment data was available (n = 13) were reported to have undergone thyroidectomy. No patient died of a second thyroid carcinoma.
For second CNS tumors (n = 10), 2 patients with embryonal tumors received surgery, radiotherapy and chemotherapy, and a patient with medulloblastoma survived, whereas a patient with PNET died of refractory disease. For high-grade gliomas, 2 patients (1 with glioblastoma and 1 with anaplastic oligodendroglioma) underwent surgery and then received chemotherapy, and other 3 patients received chemotherapy alone. Among them, only 1 patient with anaplastic oligodendroglioma survived, whereas other 4 patients died of refractory disease. A patient with brainstem glioma received radiotherapy and chemotherapy, but died of refractory disease. Two patients with low-grade glioma received radiotherapy and chemotherapy, and survived. The 5-year OS rate of all second CNS tumors was 35%. Notably, the outcome of patients with high-grade or brainstem glioma was very poor with a 5-year OS of just 17%.
DISCUSSION
Our current report presents the findings of a second retrospective survey of SMNs in childhood cancer survivors from multi-center in Korea. In the first survey, 24 patients with SMN treated from 1981–1997 had been enrolled from 6 institutions, including 7 cases of AML, 5 cases of osteosarcoma, and 5 cases of ALL (7). Our present study included a broader spectrum of SMN cases in which t-MNs were the most common SMN to be recorded during a median 8.6 years follow-up period, similar to the first report. Notably, t-MNs after CNS tumors or osteosarcoma were the most common combination of malignancies observed. However, in contrast to the first report, our present analyses indicated that thyroid carcinoma and CNS tumors represented other prevalent SMNs. The outcomes of patients with second t-MNs were poorer than those with de novo AML or MDS, whereas a second osteosarcoma showed a comparable outcome to a primary osteosarcoma, and patients with second thyroid carcinoma exhibited a 100% survival rate.
Previous studies have each reported a diverse spectrum of SMNs. The study of the CCSS cohort (median age, 34 years) reported non-melanoma skin cancer, breast cancer, thyroid cancer, and CNS tumors as the most common SMNs (6). A long-term follow-up study of the BCCSS cohort, with a median follow-up time of 24.3 years, reported the most frequently observed SMNs as CNS tumors and non-melanoma skin cancer, followed by digestive, genitourinary, and breast cancers (6). A population-based case-control study conducted in 5 Nordic countries with an average follow-up period of 7.5 years reported that CNS tumors, bone and soft tissue tumors, breast cancer, digestive tract cancer, and leukemia were the most common SMNs (8). A regional cohort study conducted in France reported over a median follow-up of 9.8 years that the most common SMNs were thyroid carcinomas, followed by bone tumors, leukemia, post-transplant lymphoproliferative disease, and CNS tumors (9). A single-center study from Hong Kong reported t-MNs and CNS tumors as the most frequent SMNs over a median follow-up of 5.3 years (10).
These significant discrepancies among studies on the incidence of different SMNs are a consequence of differences in the distribution of PMNs, the follow-up duration, and ethnicity of the patients analyzed. Long-term follow-up studies are more likely to include solid tumors because the latency period of a solid tumor is greater than that of a hematologic malignancy. In the present study, the latency period of t-AML and t-MDS was 2.8 and 2.7 years, respectively, which were comparable to previous studies (111213). Additionally, the rarity of Hodgkin lymphoma in Korea explains the low incidence of breast cancer, which has been associated with the radiation fields that are used to treat Hodgkin lymphoma. Because the median follow-up period of the BCCSS study was greater than 20 years and the median age of the CCSS cohort was 34 years, their reports included many adult-type cancers, such as digestive, genitourinary, and breast cancers. However, because our present questionnaire survey was limited to pediatricians and the median age of our study cohort was 12.7 years with a relatively short follow-up time, our cohort was less likely to include adult-type solid cancers and more likely to include t-MNs. Thus, longer follow-up would change the distribution of SMNs, resulting in the increase of solid tumors as SMNs. Therefore, our findings should be interpreted with caution, as the data were limited to childhood cancer survivors during adolescence and early adulthood. To overcome this limitation and obtain a more accurate estimate of SMNs in childhood cancer survivors in Korea, a comprehensive cohort follow-up study will be required.
In our present analyses, t-MNs were the most common SMN, perhaps because of the short latency periods of t-MNs, the short follow-up time of the study, and the limitation of our questionnaire survey to pediatric hemato-oncologists. It was difficult to definitely distinguish t-MNs as SMNs from relapse of PMNs with immunophenotypic changes, especially when latency periods between primary and second leukemia was short. To reduce the possibility of relapse of PMNs, we only included the patients who developed typical cytogenetic aberrations of t-MNs such as 11q23 translocations or chromosome 7 and 5 abnormalities, or distinguished cytogenetic aberrations from primary leukemia. The most common cytogenetic abnormalities were 11q23 translocations in t-AML and chromosome 7 and 5 abnormalities in t-MDS, a finding that is consistent with previous reports (1415). Previously, outcomes of t-MNs have been reported to be dismal (11121416). In our current study cohort, the outcomes for patients with t-MNs also appeared to be poorer than patients with de novo AML or MDS. Although the survival rate of the patients with t-MN who received allogeneic HSCT was better that of those patients who did not, our data do not suggest that allogeneic HSCT is beneficial in these patients, because those patients who did not achieve complete remission or died due to treatment toxicity could not proceed to HSCT. Thus, future studies of the role of allogeneic HSCT for t-MNs are needed.
Primary thyroid carcinoma during childhood is uncommon. A single-center study has reported that 17 of 25 patients with thyroid carcinoma presented with an SMN, and that 12 of these cases (71%) with second thyroid carcinoma had received radiation to the thyroid gland during therapy for their primary cancer; most of those primary cases were Hodgkin lymphoma (17). Another study showed that 68% of the second thyroid cancers developed within the field of radiation (18). In our present cohort, only 5 of 15 patients (33%) developed with previous radiation field. Relatively low incidence of radiation-associated thyroid cancers can be attributed to low incidence of Hodgkin lymphoma in Korea. Treatments for patients with second thyroid carcinomas have yielded excellent outcomes and therapeutic approaches for such lesions can therefore be similar to those used for primary thyroid carcinoma.
The most important risk factor for the development of second CNS tumors is cranial radiation, and meningioma and glioma have been reported to be common therapy-related brain tumors (1920). In our present cohort, only 5 of 10 (50%) second CNS tumor cases were associated with radiation, and most of these patients had glioma and seemed to require a longer latency period than patients who did not receive cranial radiation. Typically, meningioma associated with radiation requires a long latency period (> 10 years) (192021), so it was not included in our present study series. In addition, our present study surveyed the patients who received chemotherapy and did not include those who received radiotherapy alone for primary CNS tumors. The outcomes for patients with second CNS tumors were very poor in our present study, especially for high-grade glioma cases. However, this finding is consistent with the survival rates of de novo high-grade glioma, so the outcomes of subsequent CNS tumors remain to be investigated.
Thyroid cancers, brain tumors, and breast cancers has been well known to be associated with previous therapeutic radiation. Besides, bone and soft tissue sarcomas, genitourinary, or gastrointestinal cancers have been reported to develop in previous radiation filed (22). Previous epidemiologic studies have reported the dose-response relationship for SMNs after therapeutic radiation, with the exception of thyroid cancers, for which there was a linearly increased risk up to 20 Gy, and then a decrease in risk for doses > 20 Gy (23).
In the present study, the latency periods for SMNs after radiation therapy seemed slightly longer than those not associated with previous radiation, but without statistical significance. One explanation for this tendency is that SMNs after radiation therapy require more than 5 years of latency period, because at least a 5-year lag has been shown between radiation exposure and second cancer development (22).
Our present study had several limitations of note. First, we could not collect epidemiological data because our analyses were based on a retrospective medical review rather than on information from a registry. Our data could not show a cumulative risk of SMNs among childhood cancer survivors or the incidence of SMNs in the selected patients who had risk factors such as cranial radiation or cancer predisposition syndromes. Also, the estimation of frequencies of SMN was likely to be hampered by a selection bias. Thus, our study does not represent the epidemiological aspects of SMNs after childhood cancer in Korea, but provides the clinical features and outcomes of a retrospective, selected case series. Second, our present questionnaire survey was limited to pediatric hemato-oncologists. For this reason, we could not collect data on adult-type, very late cancers because of our short follow-up period and difficulties in monitoring childhood cancer survivors into adulthood. Thus, our results should be interpreted cautiously, limiting to an early follow-up period in a pediatric hemato-oncology clinic.
In conclusion, the most common types of SMNs in childhood cancer survivors, which were encountered in a pediatric hemato-oncology clinic during the early follow-up period, were t-MNs, thyroid carcinoma, CNS tumors, and osteosarcoma. The outcomes of patients with second t-MNs and CNS tumors were especially poor, whereas patients with second osteosarcomas showed comparable outcomes to cases with its primary counterpart. Additionally, second thyroid carcinomas had no significant impact on long-term survival. Our current study did not evaluate the relative risks of SMNs based on epidemiological data and a nationwide childhood cancer survivor registry should therefore be established in Korea to evaluate the incidence and outcomes of SMNs. The findings in our current study can provide baseline data for future multi-center trials of childhood SMNs. Further therapeutic efforts will be required to improve the survival outcomes in patients with SMNs, especially in cases with t-MNs and CNS tumors.
 XML Download
XML Download