

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Scrub typhus, also called tsutsugamushi disease, scrub fever, Japanese river fever and trombidiasis, is a disease that causes high fever, headache, and conjunctival hyperemia by proliferation of Orientia tsutsugamushi when larvae of Trombiculidae as a vector infected with O. tsutsugamushi bites in the skin of a person and eats the body fluid. It is an acute, febrile, exanthematous illness with a high fatality rate. Scrub typhus is wildly present in the triangle area connecting Japan, India, and Northern Australia (12). The vector of scrub typhus in Southeast Asia is Leptotrombidium delicense and, in the case of Japan, the vector contains L. akamushi, L. scutellare, and L. pallidumia (3). Vectors, such as L. pallidum and L. scutellare, are known in Korea (4). During World War II and the Vietnam War, tens of thousands of patients and a large number of deaths were reported. The infection is prevalent in Southeast Asian countries such as Taiwan, Malaysia, the Philippines and Australia (56)
The first cases in Korea were confirmed from six soldiers of the United Nations in 1951 (7). An army medical officer of the United States isolated and reported the pathogen from mites and wild rodents in 1957 (8). In patients, the bacterium was separated after proving serologically in 1986 (910). It has been reported that scrub typhus patients of acute febrile diseases during a fall season in Korea hold about 40%-50%. More than 90% of the disease occurrence happens from mid-October to early December (11).
More than twenty serotypes are known in the world. Three serotypes including Gilliam, Karp, and Kato have been used for serodiagnosis as major serotypes of O. tsutsugamushi (12). Until now, Gilliam, Karp, and Boryong serotype have been reported in Korea. However, Kato has not been reported. A number of novel strains have been isolated in Korea (1314).
An indirect immunofluorescence antibody assay (Immunofluorescence Assay, IFA) is a typical assay for tsutsugamushi disease. This assay has an advantage of accurate diagnosis compared with other methods (15). However, it has many disadvantages, for example, requiring expensive equipment, a fluorescence microscope, slides with all serotype specimens prevalent in each area, and consuming the time to process many specimens. The assay should be directly confirmed by a professional using an immunofluorescence microscope. There is subjective disagreement between the deciphers. Furthermore, it is impossible for accurate diagnosis when a new or unknown serotype is found (1617). The passive red blood cell agglutination method is designed to make it easier to diagnose scrub typhus in the clinic. This method is simple and widely used due to consuming less time and effort compared with IFA (18). However, it has disadvantages such as relatively low sensitivity and nondiscrimination of IgG and IgM.
In this study, the developed recombinant antigenic protein can be applied to patients all over the world to determine the presence of specific antibodies against the scrub typhus pathogen regardless of serotypes. The test kit, using the above antigen, can quickly and accurately discriminate IgM and IgG. Both domestic and international clinical institutions have evaluated the clinical performance of the test kit.
MATERIALS AND METHODS
Gene cloning and expression of recombinant proteins
Based on the fact that 56 kDa of surface antigenic protein of Orientia tsutsugamushi has antigenicity and diagnostic value, genes encoding the fragment of 56 kDa protein from the major serotypes, including Gilliam (tsg56, GenBank AY335819), Karp (tsa56, GenBank AY956315), and Kato (tst56, GenBank M63382), were amplified by polymerase chain reaction (PCR). The antigenic region was selected from the 56-kDa outer membrane protein gene which showed more than 30% amino-acid sequence homology with each other at 56-kDa outer membrane proteins of O. tsutsugamushi prototype Gilliam, Karp and Kato to make the chimeric 56-kDa protein. The amplified DNAs were connected in series and cloned into protein expression vector (pET-22b+). The cloned DNA was expressed in E. coli as a fusion protein. This fusion antigenic protein (cr56, 103 kDa) which is produced, isolated and purified in a single process at the same time can be used in diagnosing scrub typhus.
In addition to Gilliam, Karp, and Kato, the gene encoding 56 kDa protein (kr56, GenBank AF302990) from O. tsutsugamushi Kangwon strain and the gene encoding 21 kDa protein (r21, GenBank AM494475) from O. tsutsugamushi Boryong, were amplified by PCR and cloned into protein expression vector (pET-30a) to improve the sensitivity of the scrub typhus diagnosis. Each cloned DNA was expressed in E. coli and purified to use the scrub typhus diagnosis and each protein was added to cr56.
The expressed 3 antigens were purified using His-bind Resin (Novagen, Cat No.69670-4) and dialyzed with potassium phosphate buffer. After formulating each antigen as 2 mg/mL, the mixed antigens were applied to the test line.
Collection of serum samples
Control serum specimens (n = 217) from a healthy person were obtained from the Department of Microbiology, College of Medicine, Hallym University and Korea Bank for Pathogenic Viruses. The serum specimens from a patient with scrub typhus (n = 141 for IgM, 136 for IgG), leptospirosis (n = 23), murine typhus (n = 48), hemorrhagic fever with renal syndrome (HFRS, n = 48), and rheumatoid factor (n = 3) were provided by the Department of Microbiology, College of Medicine, Hallym University and Korea Bank for Pathogenic Viruses. The serum specimens from patients with mycoplasma (n = 3), tularemia (n = 1), cytomegalovirus (CMV, n = 3), Epstein-Barr virus (EBV, n = 3), herpes simplex virus (HSV, n = 2), varicella zoster virus (VZV, n = 2), hepatitis A (n = 1), and hepatitis B (n = 3) were kindly provided from Biobank of Gyeongsang National University Hospital. The serum specimens from patients with toxoplasma (n = 2) and human immunodeficiency virus (HIV, n = 1) were obtained from Biobank of Keimyung University Dongsan Medical Center. The serum specimens from patients with rheumatoid factor (n = 3) and anti-nuclear antibody (ANA, n = 3) were provided by Biobank of Wonkwang University Hospital.
For the serum samples from India, blood samples were collected from clinically suspected scrub typhus cases (n = 87), which were IgM positive at InBios ELISA, during a sixteen months period from August, 2013 to November, 2014. IFA was performed blindly at Department of Microbiology & Immunology, School of Medicine, Hallym University.
In the case of serum samples (n = 89 for cases, 76 for control) from Sri Lanka, IFA was performed blindly at the Rickettsial Disease Diagnostic and Research Laboratory, Faculty of Medicine, University of Kelaniya for rickettsial antibody testing against O tsutsugamushi antigens.
Indirect immunofluorescent antibody assay (IFA)
Serological diagnosis of scrub typhus was performed by the IFA as described by Kim et al. (14). Briefly, O. tsutsugamushi strains Gilliam, Karp, and Kangwon 87-61 were cultured on monolayered mouse L929 cells in a humidified 5% CO2 atmosphere at 37°C containing 2% fetal bovine serum (Gibco BRL, Grand Island, NY, USA). When the cytopathic effect approached 50%-70% of the cells, the cells were harvested and then dotted on Teflon-coated spot slides, following fixation with acetone for 10 minutes. The slides can be stored in a freezer at -70°C without exposure to air from outside until used. After applying patient serum diluted two-fold serially (1:10 to 1:1,280 in phosphate buffered saline [PBS]) to the antigen-coated spot of the slide for 30 minutes, fluorescein isothiocyanate (FITC)-conjugated antibody, antihuman IgM or IgG (Cappel Laboratories, Cochranville, PA, USA) was applied to determine the positive signal. Endpoint titer against individual serum was represented as the reciprocal of the highest serum dilution at which rickettsiae exhibited clear positive fluorescence at any one of the three strains. From diagnostic study in Korea, cutoff values of titer at IgM and IgG IFA were ≥ 1:10 and ≥ 1:40 (14).
InBios ELISA for diagnosing scrub typhus
An ELISA plate was coated with O. tsutsugamushi derived recombinant antigens. ELISA, IgM/IgG targets antibodies to the 56-kDa antigenic protein. The procedure followed with the manufacturer's protocol. The initial serum dilution was 1:100. After incubation and washing of plates, optical density (OD) was read at 450 nm in iMark Microplate Reader (Bio-Rad, Japan). Twenty samples were collected from healthy volunteers and used in the calculation of the cut-off value in both IgM & IgG ELISA tests. Cut-off values were calculated as follows: Cut-off value = Average of the normal human serum samples (NHS) + three times of standard deviation (SD) from of NHS.
The samples with OD values above the cut-off were considered positive and those below the cut-off were taken as negative. Borderline samples were retested in triplicate.
Rapid diagnostic Test (RDT)
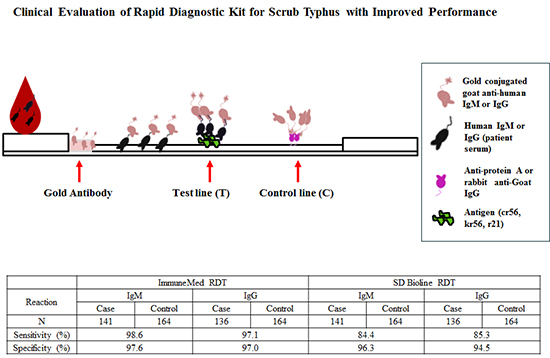
A mixture of cr56, r21 and kr56 of O. tsutsugamushi as antigen (0.8 ± 0.08 μg/strip) was applied to RDT membrane (RDT kit manufactured by Immunemed) (19). The test procedure was briefly as follows: 300 μL diluent buffer including 3 μL serum was applied to the sample port of the test kit and then a complex of antigen-serum antibody-gold conjugated anti-IgM or IgG was run on each IgM or IgG test strip. The result was read at 15-20 minutes. The red color appearing concurrently on control line (C) and test line (T) was regarded as positive. The test was considered as negative when only the control line appeared and it was invalid if there was no detection of control line.
Data analysis
Variables indicate the number of true positives (TP), true negatives (TN), false positives (FP), and false negatives (FN). Accuracy and reliability were calculated by (TP+TN)/number of all tests and ([TPxTN]-[FPxFN])/([TP+FN][TN+FP]) respectively. Positive predictive value (PPV) indicates the value of TP/(TP+FP) and negative predictive value (NPV) is TN/(TN+FN).
RESULTS
Sensitivity and Specificity of the ImmuneMed RDT of Each IgM and IgG
Positive or negative was determined by subjective visual interpretation (Fig. 1). Control line (C) represents the validation of test results. Red colorization of test line (T) indicates the presence of human antibody against O. tsutsugamushi.
Fig. 1
Representative pictures for RDT indicating negative and positive results. Red colorization of the test line (T) indicates the presence of human antibody against O. tsutsugamushi and the red control line (C) represents the valid test result. Demonstration is negative (kit 1), both positive in IgM and IgG (kit 2), IgM positive (kit 3), and IgG positive (kit 4) in RDT results.

Table 1 shows the sensitivity and specificity of RDT of each IgM and IgG at the base of IFA performed in Korea. Of the 141 positive serum samples by IFA IgM from Korea, 139 were positive in RDT assay with 98.6% sensitivity for IgM. Out of 136 positive scrub typhus cases evaluated by IFA IgG, 132 cases were identified as positive in RDT assay with 97.1% sensitivity for IgG. For IgM, four of the 217 controls were found false positive in Korea. Thus, specificity of RDT for IgM was 98.2%. For IgG among 217 control specimens, only five controls were considered as false positive in Korea. Thus, specificity of RDT for IgG was 97.7%.
Table 1
Sensitivity and specificity of the ImmuneMed scrub typhus RDT at the base of each IgM and IgG IFA in Korean patients
Examination of cross-reactivity of ImmuneMed RDT to different diseases
To evaluate the cross-reactivity of ImmuneMed RDT to different diseases, serum samples were collected from Korea Bank for Pathogenic Viruses, and Biobank of several different hospitals. Each blood sample was applied to ImmuneMed RDT as serum, plasma, and whole blood to evaluate the performance depending on the state of the sample. Serum samples for murine typhus (n = 48), leptospirosis (n = 23), and hemorrhagic fever with renal syndrome (HFRS, n = 48) were collectively called as acute febrile illness due to the similarity of clinical symptoms and epidemic patterns.
ImmuneMed RDT did not react with any other disease, including HFRS (n = 48), leptospirosis (n = 23), murine typhus (n = 48), mycoplasma (n = 3), tularemia (n = 1), CMV (n = 3), EBV (n = 3), HSV (n=2), VZV (n = 2), hepatitis A (n = 1), hepatitis b (n = 3), malaria (n = 3), rheumatoid factor (n = 6), ANA (n = 3), toxoplasma (n = 2), and HIV (n = 1).
Comparison test of the ImmuneMed RDT and SD Bioline RDT to scrub typhus
To compare with the performance of other scrub typhus RDT, SD Bioline RDT against scrub typhus was used. Table 2 shows the sensitivity and specificity of ImmuneMed RDT and SD Bioline RDT for each IgM and IgG to O. tsutsugamushi at the base of IFA in Korean patients. 141 positive serum samples by IFA IgM were used for evaluating sensitivity for IgM. 136 positive serum samples by IFA IgG were evaluated for examining sensitivity for IgG. Specificity was measured using 164 control specimens for IgM and 164 controls for IgG.
Table 2
Comparison test of the ImmuneMed RDT and SD Bioline RDT for each IgM and IgG to O. tsutsugamushi at the base of IFA in Korean patients
For IgM, the sensitivity and specificity of ImmuneMed RDT was 98.6% and 97.6%, but those of SD bioline RDT was 84.4% and 96.3% respectively. For IgG, those of ImmuneMed RDT were 97.1% and 97.0%, but those of SD Bioline RDT were 85.3% and 94.5%. This result indicates that the ImmuneMed RDT shows excellent performance of sensitivity and specificity to diagnose scrub typhus compared with SD Biolines.
Sensitivity and Specificity of the ImmuneMed RDT in Sri Lanka
Table 3 shows the sensitivity and specificity to scrub typhus at retrospective diagnosis based on IFA in Sri Lanka. Of the 89 (44 with eschars) serum samples from Sri Lanka, 82 were positive in RDT with 92.1% sensitivity. Out of 76 controls evaluated, only 3 cases were identified as false positive in RDT with 96.1% specificity. This result indicates that the ImmuneMed RDT can be used in the epidemic region of several serotypes to discriminate O. tsutsugamushi from other diseases.
Table 3
Sensitivity and specificity of the ImmuneMed RDT for retrospective diagnosis at the base of IFA in Sri Lanka
Comparison of ImmuneMed RDT and InBios ELISA for diagnosing scrub typhus in South India
To compare the performance of ImmuneMed RDT with ELISA test, the serum specimens diagnosed with InBios ELISA kit was used. ELISA from InBios was currently used for diagnosing scrub typhus in South India. As shown in Table 4, there is a 94.0% concordance rate between ImmuneMed RDT and InBios ELISA to diagnose scrub typhus. This result suggests that ImmuneMed RDT can replace ELISA test for diagnosing scrub typhus with high sensitivity.
Table 4
Comparison test of ImmuneMed RDT and InBios ELISA diagnosing scrub typhus in South India patient serum samples
| Reaction | ImmuneMed RDT | InBios ELISA | ||
|---|---|---|---|---|
| IgM | IgG | IgM | IgG | |
| Case* | 50 | 50 | 50 | 50 |
| Positive | 43 | 46 | 50 | 43 |
| Negative | 7 | 4 | 0 | 7 |
| Sensitivity, % (95% CI) | 86.0 (85-86) | 92.0 (91-92) | 100 (99-100) | 86.0 (85-86) |
DISCUSSION
Scrub typhus is prevalent in rural areas of Asia (20). However, this disease is difficult to diagnose for reasons of the non-specific signs and symptoms, and the difficulty of conventional IFA availability. Although IFA is a gold standard with high sensitivity and specificity, it does not represent perfect sensitivity. Because all epidemic serotypes of O. tsutsugamushi should be provided for IFA diagnosis in each region, accessibility of IFA is difficult in most regions. O. tsutsugamushi is an obligate intracellular pathogen. It is difficult to culture due to a relatively high cost and it requires biosafety level (BSL) 3. For these reasons, clinicians in underdeveloped countries may choose and use the non-specific and insensitive Well-Felix reaction (18).
In our previous study, we showed the diagnostic sensitivity of scrub typhus using a mixture of recombinant antigens derived from O. tsutusgamushi serotypes (21). In this study, we further improve the sensitivity and specificity of the ImmuneMed RDT and apply it in Korea and Sri Lank to confirm the performance of RDT. Performance of the ImmuneMed RDT was also compared with that of SD Bioline RDT. Furthermore, the ImmuneMed RDT was compared with ELISA test for confirming the performance of the RDT using serum samples in South India.
In this study, the RDT, using recombinant proteins derived from O. tsutsugamushi serotype Gilliam, Karp, Kato, Kangwon, and Boryong, was successfully applied to the different regions including Korea, Sri Lanka and South India. The performance of the ImmuneMed RDT for scrub typhus using Korea serum samples shows 98.6% and 97.1% sensitivity and 98.2% and 97.7% specificity for IgM and IgG, respectively (Table 1). Two patients for IgM and four patients for IgG from Korea showed false negative in sensitivity. IFA titer for IgM false negative was 1:40 at samples number 98-1221 and 1:10 at 00-253, and IgG false negative was 1:1280 at sample number 90-110, 1:160 at 99-279 and DK 32, and 1:640 at 00-253. These titer values are low in the IFA positive criterion and do not indicate enough antibody to react with the recombinant proteins in these patients` serum samples. Therefore, the RDT may not be reacting with patients' serum.
False positive in specificity was rarely detected in healthy controls and other disease controls. Although this false positive may not be non-specific reaction, we cannot rule out the factor that patients have residual antibody reacting with antigens from a past infection, an unapparent infection, or an infection with another serovar which is not used at IFA, especially in case of Sri Lanka.
Furthermore, a comparison test was performed between ImmuneMed RDT and SD Bioline RDT. The specificity of each RDT was similar at healthy controls and other diseases. However, at sensitivity, the ImmuneMed RDT is superior to that of SD Bioline RDT. This result indicates that the recombinant proteins (antigens) made from the ImmuneMed RDT have good properties to detect the antibody against O. tsutsugamushi compared with SD Bioline RDT (Table 2). ImmuneMed scrub typhus RDT used antigens from five serotypes of O. tsutsugamushi including Gilliam, Karp, Kato, Kangwon, and Boryong. However, SD Biolines tsutsugamushi test utilized antigens from three serotypes of O. tsutsugamushi including Gilliam, Karp, and Kato. Another difference is that ImmuneMed used anti-human IgG as secondary antibody to enhance the affinity compared with protein A for SD biolines. These two factors make differences for sensitivity and specificity for diagnosing scrub typhus.
In Sri Lanka, the performance of the ImmuneMed RDT shows 92.1% of sensitivity and 96.1% of specificity. Although the number of serum samples looks small, the accuracy and reliability of the test is sufficient. Seven false negatives may be due to unknown infection except O. tsutsugamushi in Sri Lanka. Three false positives from healthy controls from Sri Lanka reacted with antigens from a past infection, an inapparent infection, or an infection with an unknown serovar. In addition, as a patient infected with a rare or new serovar has not been diagnosed as scrub typhus even though to use IFA, RDT may be a real positive but it might be interpreted as a false positive.
To compare with other detection methods, ELISA test was chosen to evaluate the performance of the ImmuneMed RDT. Even though only IgM positive at ELISA as sample was selected, there is a 94.0% similarity between ImmuneMed RDT and InBios ELISA at retrospective diagnosis from patients of O. tsutsugamushi (Table 4). This means that the selected antigens from five different serotypes and other technical improvement represent to similar or better performance with InBios tsutsugamushi ELISA. This indicates that the ImmuneMed RDT can replace ELISA test to diagnose scrub typhus as an easy and time saving diagnostic tool with high sensitivity and specificity.
ImmuneMed Scrub Typhus RDT can detect IgM and IgG to speculate not only a current infection but also the progress of the disease simultaneously. Especially in Sri Lanka and South India, it can be positive interpretation based on an inapparent infection, past infection, or infection of another serovar which is not used in IFA even though IFA titer is not positive.
In this study, the clinical evaluations reveal that ImmuneMed Scrub Typhus RDT is very consistent with IFA in Korea and Sri Lanka. Additionally, the use of ImmuneMed Scrub Typhus RDT as a primary diagnosis for O. tsutsugamushi infection would assure easy diagnosis of the disease. Since scrub typhus can be treated with doxycycline, accurate and rapid diagnosis will provide effective management of this disease (35). We believe that ImmuneMed Scrub Typhus RDT should be in place not only at hospitals but also other health centers owing to its accuracy, rapidity, simplicity, and low necessity for skill. Furthermore, it may improve the rapid detection of scrub typhus and be applicable for global diagnosis after further development.
 XML Download
XML Download