

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite the high prevalence of microscopic hematuria in adults, a consensus on the extent of evaluation remains controversial (123). Even more, the exact definition of microscopic hematuria is unclear (45). The scarcity of long-term data related to disease progression of isolated microscopic hematuria (IMH) is related to the equivocal consensus (6). In contrast to the lack of interest and data, an increasing number of people are receiving health screening and are diagnosed with incidental asymptomatic microscopic hematuria. IMH can be transient; however, our previous study focused on persistently existing microscopic hematuria (7).
Several studies have discussed IMH but most reports are either out of date or short-term retrospective studies, and pathological diagnostic data are extremely rare (5689), which is related to the controversy surrounding renal biopsy in patients with IMH. Renal biopsy is supported by some groups because the pathology can suggest a prognostic factor (110). However, some nephrologists do not recommend a biopsy because identifying prognostic factors will not change the course of management (1112).
These trends and debates lead us to design a study to present the long-term natural course of single-center patients with biopsy-proven isolated microscopic hematuria. The follow up focused on whether patients progressed to chronic kidney disease (estimated glomerular filtration rate [eGFR] < 60 mL/min/1.73 m2 for > 3 months) or significantly high proteinuria (> 300 mg/g urine protein to creatinine ratio [PCR]), as the presence of either marker suggests declining kidney function. Our study is unique because we focused only on patients with IMH. This was a 7-year retrospective, single-center study.
MATERIALS AND METHODS
Clinical definitions
The terms concerning microscopic hematuria need to be clarified. We defined IMH as the presence of two or more red cells per high-power field on a microscopic examination and absence of any other clinical symptom or signs. The absence of proteinuria was confirmed by a repeated negative dipstick test or < 300 mg/g in spot urine PCR. Trace proteinuria was neglected from the subjects.
Estimated glomerular filtration rate
The Modification of Diet in Renal Disease (MDRD) equation: 186.3 × [serum creatinine (sCr) (mg/dL)] – 1.154 × [age (years)] – 0.203 × (0.742 if female) was used to determine eGFR (13). Our laboratory does not use the isotope dilution mass spectrometry MDRD study equation due to global usage of the MDRD equation (14).
Subjects
A retrospective study was designed for subjects who had undergone renal biopsy from February 2002 to January 2011. Patients were meticulously evaluated for the presence of other secondary causes of hematuria, such as malignancy or urolithiasis. Any patient with such a secondary cause was excluded from biopsy. Renal biopsy for IMH was recommended by a single clinician to exclude any selection bias. The clinician recommended biopsy to every patient entering the clinic with IMH. Only those who agreed to the procedure received the biopsy. Also, patients were included in the study if they fulfilled the criteria listed below (Fig. 1).

Consecutive presence of > 2 red blood cells/high power microscopic field (test was repeated three times), sCr < 1.2 mg/dL, eGFR > 90 mL/min/1.73 m2, urine PCR < 300 mg/g (spot urine test was done only once), resting systolic blood pressure < 140 mmHg, resting diastolic blood pressure < 90 mmHg, sterile urinalysis except hematuria, absence of gross hematuria, and patients > 15 years old. All patients had undergone either ultrasonography or computed tomography to exclude any secondary causes. Patients with a chronic medical history or presence of a family history suggestive of Alport's syndrome were also excluded. Finally, 350 of the 1,508 patients (23%) were enrolled for the analysis.
Renal biopsy
Renal biopsy was done under ultrasonographic guidance. An 18G core needle and automated biopsy gun were used to target the inferior pole of the left kidney. All biopsy specimens were examined by light microscopy, immunofluorescence, and electron microscopy. Specimens of inadequate quality or quantity were excluded. The main focus of the biopsy results was the pathologic diagnosis and the presence of chronic histopathological features (tubular atrophy, interstitial fibrosis, and glomerulosclerosis).
Statistical analysis
All data are expressed as mean ± standard deviation. Student's t-test, the χ2 test, or Fisher's exact test were used to compare the data and detect differences. A two-sided P value < 0.05 was considered significant. All analyses were done using SPSS ver. 18.0 software (SPSS Inc., Chicago, IL, USA). A multivariate model (Cox proportional hazard model) was used to evaluate factors (age at biopsy, body mass index [BMI], initial blood pressure, initial proteinuria, baseline Cr, and presence of chronic histopathological changes in the biopsy leading to a progression to significant proteinuria).
RESULTS
Baseline patient characteristics
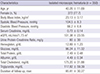
The baseline clinical characteristics of the 350 consecutive patients are listed in Table 1. Age ranged from 15 to 58 years and the mean was 40 ± 12 years. There were 78 males (22.3%) and 272 females (77.7%) included. The mean baseline urine PCR was 80 ± 30 mg/g with a mean follow up of 86 months. Mean body mass index was 23.1 ± 3.2 kg/m2. Mean systolic blood pressure was 104.5 ± 8.3 mmHg, and mean diastolic blood pressure was 66.2 ± 6.8 mmHg. Mean baseline sCr was 0.72 ± 0.14 mg/dL with a mean eGFR of 101.38 ± 23.55 mL/min/1.73 m2.
Table 1
Baseline clinical characteristics of isolated microscopic hematuria patients
Renal histology findings
The renal pathologic diagnoses of the 350 patients are shown in Table 2. The dominant pathologic diagnosis was IgA nephropathy (164/350, 46.9%), followed by idiopathic mesangial proliferative glomerulonephritis (151, 43.1%). Eleven (3.1%) patients had focal segmented glomerulosclerosis, six (1.7%) had minor glomerular changes, five (1.4%) had thin basement membrane nephropathy, four (1.1%) had membranous proliferative glomerulonephritis, four (1.1%) had IgM nephropathy, four (1.1%) had membranous glomerulonephritis, and two (0.6%) had normal biopsy results.
Table 2
Renal pathologic diagnosis of isolated microscopic hematuria patients
The number of patients who presented with a chronic histopathological feature at baseline is listed in Table 3. Nearly half (166, 47.4%) of the patients had chronic pathological changes. Segmental or global glomerulosclerosis was seen in 91 patients (26%). Tubular atrophy and interstitial fibrosis was shown in 130 (37.1%) and 124 (35.4%) patients, respectively.
Table 3
Baseline chronic histopathologic features of isolated microscopic hematuria patients

IgAN, IgA nephropathy; IMPGN, idiopathic mesangial proliferative glomerulonephritis; FSGS, focal segmental glomerulosclerosis; GMC, glomerular minor changes; TBMN, thin basement membrane nephropathy; IgMN, IgM nephropathy; MGN, membranous glomerulonephritis; No., number of subjects; G. sclerosis, glomerulosclerosis; T. atrophy, tubular atrophy; I. fibrosis, interstitial fibrosis.
Clinical outcomes
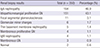
The clinical characteristics of the 350 patients and follow-up data are shown in Table 4. Follow-up duration was 12–148 months (mean, 85.81 ± 30.27 months). Systolic and diastolic blood pressure increased significantly (P < 0.001). However, mean blood pressure was within a normotensive level. sCr level increased significantly from a baseline of 0.72 ± 0.14 mg/dL to 0.76 ± 0.18 mg/dL at the end of follow up (P < 0.001). eGFR decreased from 101.4 ± 23.6 mL/min/1.73 m2 to 92.5 ± 18.2 mL/min/1.73 m2 (P < 0.001). The baseline urine PCR increased from a mean of 80 ± 30 mg/g to 100 ± 120 mg/g after a mean of 86 months (P = 0.003).
Table 4
Clinical characteristics in the isolated microscopic hematuria patients during the follow-up
Ten patients developed significant proteinuria (> 300 mg/g in urine PCR) at the end of follow-up (Table 5). All 10 had been diagnosed with IgA nephropathy using the initial biopsy. The urine PCR increased in other patients but was always < 0.3. Three patients progressed to chronic kidney disease (CKD) with an eGFR < 60 mL/min/1.73 m2. A 19-year-old male who was diagnosed with IgA nephropathy class II developed significant proteinuria after 17 months and his eGFR declined to < 60 mL/min/1.73 m2 after 63 months. The eGFR of a 43-year-old female diagnosed with idiopathic mesangial proliferative glomerulonephritis also declined to < 60 mL/min/1.73 m2 after 134 months. A 48-year-old woman with a minor glomerular lesion but chronic histopathological changes on biopsy progressed to an eGFR < 60 mL/min/1.73 m2 after 66 months.
Table 5
Occurrence of significant proteinuria or chronic kidney disease at the end of the follow-up
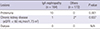
| Lesions | IgA nephropathy (n = 164) | Others (n = 172) | P value |
|---|---|---|---|
| Proteinuria | 10 | 0 | 0.001 |
|
Chronic kidney disease (eGFR < 60 mL/min/1.73 m2) |
1 | 2* | 0.637 |
| Dialysis | 0 | 0 | N/A |
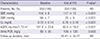
Ten of 164 patients (6.1%) in the IgA group presented with significant proteinuria at the end of the follow up. A chi-square analysis of these patients showed IgA nephropathy compared to that in the other group (P = 0.001). A multivariate Cox proportional hazard model analysis was performed to evaluate independent risk factors for the proteinuria and CKD, including age, sex, BMI, blood pressure, Cr level, urine protein-Cr ratio, biopsy results, and the presence of chronic changes on the biopsy. However, no significant risk factors leading to such events were detected.
DISCUSSION
This study is unique and the results are significant for clinicians. First, we evaluated patients with IMH who had histopathological reports. Second, long-term data after renal biopsy are rare in patients with IMH. Our data include a maximum 12 years follow up with a mean follow up of 86 months (78915). In addition, this was a large retrospective dataset of 350 patients with IMH from a single center. The single center and single physician decreases the possibility of selection bias.
The pathological diagnoses were diverse among patients with IMH. IgA nephropathy was the most common followed by idiopathic mesangial proliferative glomerulonephritis, with prevalence rates of 46.9% and 43.1%, respectively. The result that IgA nephropathy was the most common pathology is compatible with previous reports (78915). However, our data suggest a low prevalence (1.4%) of thin basement membrane disease in contrast to other reports. These contrasting reports may be related to different prevalence rates of thin basement membrane disease (TBMN) among geographic areas (16). TBMN is generally thought to be a benign renal disease. It has a very low risk of progressing to renal failure, whereas other chronic glomerulonephritis diseases, such as IgA nephropathy, generally result in decreased renal function during a long-term follow up. Such possibility supports the need for renal biopsy, which may lead to early aggressive management. Nevertheless, the necessity and risks of renal biopsy for these patients remain controversial.
The Oxford classification is a pathologic classification of IgA nephropathy with prognostic variables (17). The main six pathological variables are mesangial cellularity score, segmental sclerosis, endocapillary hypercellularity, cellular/fibrocellular crescents, percentage of fibrosis/tubular atrophy, and the arteriosclerosis score. Among these variables, chronic lesions, such as tubular atrophy, interstitial fibrosis, and glomerulosclerosis, have been reported to be the most meaningful histological predictors (1819). In our study, 45.7% (75/164) subjects with IgA nephropathy presented with one or more of these chronic lesions. However, we were unable to find an association between the chronic changes and declining renal function. The same result occurred with those who eventually progressed to significant proteinuria. These negative outcomes are thought to be related to the follow-up duration. Our study included patients who were evaluated for > 12 years; however, the mean duration was 86 months, which is slightly more than 7 years. Previous reports using the Oxford classification generally included > 10 years of cohort data from patients with IgA nephropathy (111217). We also evaluated whether such chronic changes was associated in patients with IMH rather than IgA, but no association was found.
Proteinuria at the initial diagnosis was a poor prognostic factor in several studies (79). None of our patients with IMH had significant proteinuria at the initial evaluation. However, significant proteinuria became evident in 10 patients with IgA nephropathy during the clinical course. Chow et al. (7) reported that each 0.1 g/day increase in baseline proteinuria is related to a two-fold relative risk of developing adverse renal events. We only had one patient who developed proteinuria in 18 months and progressed to CKD with an eGFR < 60 mL/min/1.73 m2 at the 63 month-follow-up. We expect that longer duration observations would show a negative association between proteinuria and renal function. In addition, all of the patients who developed proteinuria had IgA nephropathy. Renal function decreased to an eGFR < 60 mL/min/1.73 m2 in three patients with IMH during the follow up, which is < 1% of all patients with IMH, and may be related to the relatively short duration of observations.
Several limitations in our study should be mentioned. The retrospective design lead to selection bias. To overcome this bias, we recruited subjects from a single physician at a single center. Another limitation was the lack of baseline data related to microalbuminuria. However, we provided spot urine protein-Cr ratio and repeated urinalysis data before the biopsy to minimize the risk of pre-existing proteinuria.
In summary, we described the natural course and necessity for intervention to determine the pathology of patients with IMH. Our results show that the prevalence of proteinuria increased during the 7 year follow up but none of the cases progressed to advanced CKD (eGFR < 30 mL/min/1.73 m2). Therefore, we conclude that IMH has a generally benign course despite the increased rate of proteinuria. Yet, IgA nephropathy should be observed when a rapid progression to proteinuria is detected.
 XML Download
XML Download