

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Emergency department (ED) crowding is a serious problem in most tertiary hospitals in Korea. According to the 2009 data of the National Emergency Department Information System (NEDIS), the mean ED length of stay (LOS) of inpatients in 121 emergency medical centers in Korea was 4.2 hours, and the ratio of stay > 6 hours among ED patients was 15.5% (1), which are longer and higher than that in the United States (3.3 hours [9.7%]) (2). Crowding in EDs has negative effects such as increased dissatisfaction due to long waiting times, increased pain-exposure time for patients, increased potential for violence against medical personnel, increased ambulance diversion and burnout of medical personnel (3), and increased mortality of patients in the ED (45).
The causes of ED crowding are multifactorial; the input-throughput-output conceptual model classifies the causes according to the factors contributing to ED crowding and is a representative model that explains ED crowding (6). Of these 3 components, the output component, which pertains to the ED stay of acute patients requiring hospitalization due to the lack of inpatient hospital beds, was highlighted as the main factor (78910). There have been several efforts to improve ED output through measures such as hallway admissions (1112); however, considering that ED crowding in regional hospitals is not a single-hospital problem but a community-level problem, the solution requires an approach from the regional level, as the existing measures have inevitable limitations. Therefore, we established the community-based Regional Transfer Network System (RTNS) and investigated whether the new regional intervention model could resolve ED crowding of a regional emergency medical center.
MATERIALS AND METHODS
Study design
This study was designed as a “before and after study” for adult patients who visited Kyungpook National University Hospital ED from November 2011 to October 2013. The after study period was defined as a year after implementation of the new transfer-system intervention in November 1, 2012 and the before study period was defined as a year before the intervention began.
Study setting and population
There are four tertiary hospitals and 115 secondary hospitals in the Daegu metropolitan area. Especially, four of 18 overly crowded EDs in Korea were located in Daegu, which was the city that had the most crowded EDs except Seoul (1). According to NEDIS data, about 33,000 patients a year visited to the ED through inter-hospital transfer in Daegu (13). Kyungpook National University Hospital is the only regional emergency medical center at the center of Daegu City, wherein approximately 50,000 patients are admitted to the ED annually. One tertiary hospital and 32 secondary hospitals located in Daegu were included in this study.
Before the start of this study, participating secondary hospitals provided information regarding the number of hospital beds and clinical departments available to the tertiary hospital, ahead of intervention. In the tertiary and secondary hospitals, transfer coordinator and counterpart coordinators were designated for the transfer task and care-information input, and they worked between 08:00 and 24:00 hours.
Study protocol
Indication
Patients fulfilling the following inclusion criteria for transfer to secondary hospitals among adult patients (age > 15 years) were included: 1) patients who stayed in the ED for > 6 hours in a stable condition but for whom emergency or general ward admission was delayed or those who could not use the general ward even 5 days after emergency ward admission or 3 days after emergency intensive care unit (ICU) admission; or 2) patients who required additional progress monitoring, even if the symptoms improved after acute-phase treatment or needed only conservative treatment because it was difficult to improve their status further; or 3) patients who were hospitalized in the general ward for an extended period of time and whose transfer to another hospital was deemed necessary by the attending professor. The emergency ward is a temporary ward for patients if the beds in the general ward are unavailable and exists mostly in the regional emergency medical centers in Korea.
Transfer process and web-based patient follow-up system
If a tertiary hospital patient fulfilling the transfer criteria of this study consented to transfer to a community hospital, the attending physician submitted a transfer request to the transfer coordinator in the referring hospital. The coordinator provided the patient or guardian with information on a hospital suitable for transfer. If a secondary hospital with a counterpart coordinator was selected, the transfer coordinator of the tertiary hospital requested a transfer from the counterpart coordinator by telephone and registered the patient’s medical status before transfer on the newly developed web-based patient follow-up system.
This system is a combined information system established for follow-up monitoring of the patient’s treatment progress, separate from the medical record system of each hospital. The counterpart coordinator registers the transfer request form on the website when the attending physician of a tertiary hospital requests a transfer. The counterpart coordinator enters the progress record and the final disposition (discharge, death, or re-transfer), so that the tertiary hospital is privy to the patient’s care-progress status. Before registration at the web-based patient follow-up system, it was mandatory to obtain consent to collect and use personal information from all patients or guardians according to the Personal Information Protection Act in Korea. The transfer process through the RTNS is presented in Fig. 1.

Data collection and outcome measurements
During the study period, information on patients admitted to a single tertiary hospital ED was collected using the electronic medical record database. Patient demographics, such as age, sex, insurance type and process in ED, including mode of arrival and ED LOS were recorded. The severity of ED patients was classified as Emergency Severity Index (ESI) level used in the tertiary hospital.
The primary outcome for the effect of alleviated ED crowding was estimated using the ED LOS before and after the intervention. The service-satisfaction survey was conducted as an additional parameter for all patients or their guardians transferred to secondary hospitals participating in this study from January 2013 to October 2013 through the RTNS. Survey time was 1–3 months after transfer. All surveys were conducted by the same interviewer in the form of a telephone survey using a structured questionnaire, and each question was scored on a 5-point Likert scale. Patients who obtained ≥ 4 points (very satisfied and satisfied) were categorized as positive responders.
Statistical analysis
The resources of the tertiary emergency medical center before and after the intervention were presented as a monthly average, with the general characteristics of ED patients presented as frequency and percentage. The statistical significance of the ED patient numbers before and after the intervention was tested using a one-sample test for binomial test, and that of other characteristics was assessed using a Pearson’s χ2 test. The ED LOS before and after the intervention were presented as median and interquartile range (IQR; 25th and 75th percentiles). Significance was tested using the Mann-Whitney U-test. A multivariate analysis using the general linear model was conducted to determine the effect of RTNS after adjusting for significant variables in univariate analysis. Statistical analysis was performed using IBM SPSS statistics version 19.0 (IBM co., Armonk, NY, USA).
RESULTS
Comparison of emergency medical center resources before and after the intervention
There was no remarkable difference in the number of beds before and after the intervention. The monthly average of the number of emergency medicine staffs, residents, and emergency medical technicians on duty was the same; however, the average number of registered nurses increased from 38.3 to 41.3 after the intervention. There was no change in the amount of medical equipment or the structure of the facility.
Comparison of general characteristics of patients visiting the ED before and after the intervention
The number of ED patients before and after the intervention was 48,408 and 51,013, respectively. The final dispositions of ED patients showed that the number of transferred patients increased from 1,607 (3.3%) to 2,591 (5.1%), and the rate of patients whose LOS in the ED was < 6 hours increased from 65.1% to 68.7% (P < 0.001). The proportion of patients corresponding to ESI 1 or 2 increased from 9.4% to 11.1% (P < 0.001). The general characteristics of patients visiting the ED before and after the intervention are presented in Table 1.
Table 1
General characteristics of study patients who visited the ED

Median ED LOS before and after the intervention
The median ED LOS before and after the intervention are presented in Table 2. The median ED LOS decreased significantly from 3.68 hours (IQR, 1.85-9.73) to 3.20 hours (IQR, 1.62-8.33). The median ED LOS of patients who were hospitalized to an emergency or general ward and who were discharged from ED significantly decreased after the intervention, from 2.85 hours (IQR, 1.50-5.83) to 2.50 hours (IQR, 1.28-4.95) and from 8.12 hours (IQR, 3.28-22.66) to 6.91 hours (IQR, 2.75-31.92), respectively (P < 0.001). However, there was no significant difference in the mean ED LOS of patients who were transferred from the ED to secondary hospitals (P = 0.119). The median ED LOS of ESI 1-2 and ESI 3-5 groups decreased from 4.01 hours (IQR, 2.07-12.48) to 3.57 hours (IQR, 1.78-12.78) and from 3.63 hours (IQR, 1.82-9.47) to 3.17 hours (IQR, 1.58-7.95), respectively (P < 0.001).
Table 2
Comparison of median ED LOS before and after the intervention
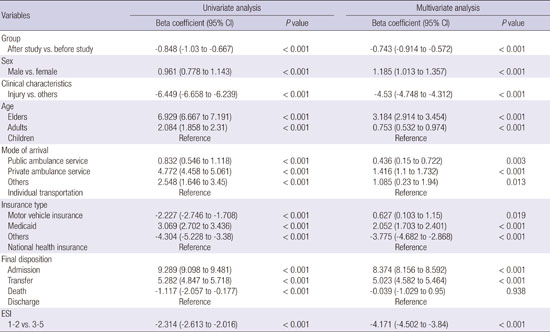
Table 3 showed that all variables used in univariate analysis were statistically significant to be associated with ED LOS. After adjusting for variables used in univariate analysis, the results of multivariate analysis showed a negative association between implementation of the RTNS and ED LOS (beta coefficient, -0.743; 95% confidence interval, -0.914 to -0.572; P < 0.001).
Table 3
The results of univariate and multivariate analysis for factors associated with ED LOS

Operation characteristics of the RTNS
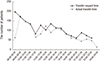
The number of transfer-request patients who used the RTNS was 1,762. Except for 287 patients whose transfer was cancelled, transfer was completed for 1,475 patients. Monthly distribution of transferred patients through the RTNS was presented in Fig. 2. The cancellation of transfer through RTNS was that hospital selection by patients without RTNS was the most common reason, with 88 patients, followed by discharge (n = 70), desire to stay in tertiary hospital (n = 66), rejection by secondary hospital (n = 28), death (n = 8), hopeless home discharge (n = 5), transferred to other tertiary hospital (n = 3) and others (n = 19). The numbers of transferred hospitals were 275. The median of transferred patients per hospital and patients transferred to secondary hospitals participating in this study were 2 (IQR 1-4) and 14 (IQR 4.75-32), respectively. The numbers of patients transferred to secondary hospitals participating in this study through RTNS were 626, and their disposition was re-transfer of 6, death of 24 and discharge of the rest. The most frequent transfer-request time was 08:00–09:00 hours (197 cases), and the most frequent actual transfer time was 09:00–10:00 hours (178 cases). Transfer request and actual transfer showed a decreasing trend after 18:00 hours (Fig. 3). The ED was the most common place of transfer request, with 1,037 patients (70.3%), followed by general ward (n = 248, 16.8%), emergency ICU (n = 120, 8.1%), and emergency ward (n = 70, 4.7%). The emergency medicine department was the most common department of transfer request, with 971 patients (55.1%), followed by neurosurgery (n = 159, 9.0%), internal medicine (n = 146, 8.3%) and orthopaedic surgery (n = 136, 7.7%).

Satisfaction of use of the RTNS
The survey was conducted on 473 patients or guardians; 355 (75.1%) of them responded. The survey questions focused on satisfaction with the information about the secondary hospital provided by the transfer coordinator and care service at the referred secondary hospitals, and reuse intention for the transfer service. The monthly average ratio of patients who responded positively was the highest for provision of information about secondary hospitals (74.4%), followed by questions on service by secondary hospitals and reuse intention (59.9% and 52.4%, respectively).
DISCUSSION
Regional emergency medical centers should be used for care of patients with very severe conditions, but they are usually used by patients with all severities of disease in Korea, including mild to serious conditions. This is a major reason for ED crowding and must be resolved to secure personnel and facilities for treating patients with urgent disease. Usually there is a lack of inpatient wards for ED patients with minor severity in the tertiary hospitals. Therefore, ED stay time is predicted to be longer and intervention for this group is necessary to relieve ED crowding.
The full capacity protocol (FCP) has been proposed as a solution for insufficient inpatient wards, which is the main reason for ED crowding (11). This protocol involved making patients wait in the inpatient ward hallway instead of the ED hallway; the satisfaction level was high, and it was successfully applied to safely resolve ED crowding (1214). However, according to one review article, because only 1.7% of all research articles that used FCP applied it as a single intervention, additional studies are needed to resolve such crowding situations (15). In addition, this method is a mere redistribution of patients within a hospital. To more effectively resolve ED crowding, it is necessary to approach the situation as a local community problem and redistribute the strain of ED crowding to the entire local community.
Inter-regional inter-hospital transfer was proposed as a part of the strategy (161718). This measure allows patients with a relatively mild disease or stable condition to transfer from a tertiary hospital with a long, predicted ED stay and be hospitalized in a local secondary hospital with available beds. Freedman and Thakkar (19) reported that by transferring clinically stable pediatric patients in a tertiary hospital ED to a regional or community hospital, the issue of lack of inpatient beds in a tertiary hospital could be resolved and the burden of ED could be simultaneously reduced. Furthermore, the safety of this type of redistribution system has been verified. The independent capacity protocol, in which the inter-hospital transfer strategy was used, was predicted to be another valuable option for resolving ED crowding and boarding of inpatients (20).
Providing the best result by optimizing supply and demand of patients to community resources is called a regionalization strategy (21). Regionalization has commonly been used in association with establishment of a regional network for specialized care of high-acuity urgent diseases such as ST-elevation myocardial infarction, post-arrest care, and acute ischemic stroke (222324). By establishing a regional network for diseases required hospitalization in this study, we induced inpatient treatment at an optimal facility while considering medical and geographical conditions.
To our knowledge, this is the first study to construct local governance using RTNS to relieve ED crowding of one tertiary hospital. The purpose of RTNS was to reduce ED LOS of tertiary hospital by transferring patients in need of a hospital admission, who was expected for a longer stay of ED to secondary hospitals. One of the notable results of our study was that the median ED LOS significantly improved despite the increasing severity of patients during study period. The median ED LOS of patients admitted and discharged from the ED significantly improved. Despite a significant increase in the proportion of transferred patients, there was no statistically significant difference in the ED LOS of patients transferred from the ED before and after the intervention. However, RTNS was not intended to expedite the transfer for patients who already met the former transfer criteria. The difference compared with the before study period was that some of the patients who stayed in the ED until admitted to the ward or discharged were aggressively transferred to secondary hospitals during the study period. Therefore, it is considered that RTNS influenced ED LOS reduction of patients admitted or discharged rather than transferred from the ED, and there is no relationship between difference of transferred patients' ED LOS and effect of RTNS. This study showed that the percentage of ESI 1 or 2 patients at tertiary hospital increased 1.7% during study period. Improving capacity of tertiary hospital for high acuity patients by reducing ED crowding is important. Although the percentage of high acuity patients at the tertiary hospital was higher than before the study period, this study did not demonstrate direct association between this result and implementation of RTNS.
It is necessary to establish a network system through which a community can share medical information for regionalization. Because the existing medical data-recording methods and systems differ among hospitals, we constructed a new web-based network service in which the local government, tertiary hospital, and secondary hospitals could participate. Through this system, a patient’s treatment progress and outcome can be shared between the referral and referred hospitals. Although the local government was not directly involved in the transfer process, it provided administrative and financial support needed to establish and maintain the system. Moreover, access to the network service was granted to only a limited number of people to prevent leakage of information.
Previous studies have reported some disadvantages of inter-hospital transfer strategy, such as unfamiliarity with the transferred hospital, transfer rejection by the community hospital, hospital income reduction, and the potential for discrimination according to the patient’s insurance coverage status (1720). However, we experienced different problems while operating this new transfer system. First, patients who wanted to be referred to secondary hospitals were focused on specific clinical departments. Most of the patients should have been referred to a secondary hospital equipped with inpatient wards available for the department of internal medicine, but the number of hospitals was relatively insufficient compared to the number of requests from the tertiary referral hospital in our region. The disparity between the demand and supply was a main problem in the transfer process. Second, at the beginning of the study, the attending physicians, except the emergency physician, lacked an understanding of inter-hospital transfer to resolve ED crowding. To overcome this issue, the “ED crowding solution committee” that included several physicians associated with ED crowding held several meetings. This helped in not only introducing the RTNS to other department physicians, but also improving the interest and understanding of ED crowding.
We tried to ensure safety of transfer and continuity of care. For this, we applied transfer indication strictly and shared medical information by developing a new web-based patient follow-up system. Thus, there were only 6 patients re-transferred in the study period and no case of unexpected death.
The hourly use of the transfer system shows that transfer requests were made most frequently at 08:00–09:00 hours, and overall, there were more transfer requests in the morning hours. This is likely because numerous transfer requests are made by patients waiting in the ED, whose transfer decisions were already made and transfer through a transfer coordinator starts at 08:00 hours. In addition, this is the time when the disposition decision of clinical patients is usually made. On the other hand, transfer request and actual transfer numbers decreased after 18:00 hours. The number of transfer cases is low at this hour because it is after the standard work hours, and fewer medical staff may be available at secondary hospitals as compared to that during the day. Based on these results, it is necessary to flexibly improve the working hours of transfer coordinators for effective operation.
In the satisfaction survey result of the network service users, satisfaction for information provision was the highest, and this is important in relieving unfamiliarity towards the referred hospital; moreover, there is room for improvement as coordinators’ skills improve. However, the reuse intent of the transfer system was relatively low, indicating that good medical service by secondary hospitals and detailed explanation for the transfer do not necessarily lead to reuse intent for the service. This finding is similar to that of the study by Freedman and Thakkar (19), in which the redistribution system did not change the trend of tertiary care center use. This might be related to the trend of favoring tertiary hospitals in Korea, and inconvenience of the transfer process might have contributed to this result. It is difficult to resolve this trend within a short period, but it can be resolved gradually through promotional activities for the public or through an improvement in medical service of secondary hospitals.
Despite our important findings, our study had several limitations. First, pediatric patients were excluded from the transfer target patients. Although hospitals where pediatric care was possible were located in the community, there was a lack of pediatric hospitals equipped with an inpatient ward that was available for project participation. Second, the inter-hospital transfer target patients included inpatient ward patients in addition to patients waiting in the ED, in order to secure empty beds to send patients waiting in the ED preferentially to the inpatient ward. Although we did not check how many ED patients could actually use empty beds secured through RTNS, it is assumed that some ED patients used those beds, considering the result of ED LOS reduction of patients admitted from the ED. However, we could not assure its effect on resolving ED crowding. Third, although results of our study showed decrease of ED LOS and increase of proportion of critically ill patients, we could not verify whether these were unique results influenced by implementation of the new transfer system intervention or other tertiary hospitals in Daegu also showed similar results at that time, because we did not establish control groups in this study. Finally, when the patient was not a resident of Daegu or wanted a specific hospital, the patient was transferred without counterpart coordinators. In such cases, the final outcome for the patient could not be determined because they were not registered in the web-based patient follow-up system. To construct a comprehensive coordinated system, more hospitals in the region must participate, and we should consider including hospitals in other regions as well.
In conclusion, ED LOS in the tertiary referral hospital decreased after implementation of the RTNS. Organic cooperation between tertiary referral hospitals, local secondary hospitals, and the local government is important for continuous maintenance of the system. To determine the effectiveness of this system, further studies should be conducted in other regions or involve more tertiary and secondary hospitals in Daegu.
 XML Download
XML Download