

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Panic disorder (PD) is a common chronic condition associated with significant social morbidity and increased health care utilization (12). There is growing evidence that poor health-related quality of life (HRQOL) is noted in patients with PD (345) even in remission state (6). However, little is known about the factors that affect HRQOL of panic patients. Although several demographic, illness-specific symptom severity, psychiatric morbidity, and social support factors were reported to predict HRQOL in panic patients (34789), the variance of the explanation is quite small to modest. Thus, it raises the question regarding other factors that affect the HRQOL. Conceptually, QOL is defined as the subjective as well as objective evaluation of physical and mental status, well-being, and environmental factors (10). A recent twin study showed that genetic factors accounted for 17% to 33% of the variance of the HRQOL by the 36-item Short-Form Health Survey (SF-36) (11), a reliable and widely used QOL-related research tool (1213). However, it is unknown which specific genes affect HRQOL in patients with PD.
Serotonin transporter gene linked polymorphism (5-HTTLPR) and Catechol-O-methyltransferase (COMT) Val158Met polymorphism have been extensively studied in psychiatric research field and known to be closely related to anxiety disorders including PD (14151617). Lesch et al. (17) first reported that individuals with one or two copies of short (S) alleles of the 5-HTTLPR have less efficient transcription of the 5-HTT gene compared to those with homozygous long (L) alleles (L/L) and show higher levels of anxiety-related trait. However, studies on the role of 5-HTTLPR have been inconsistent (181920). Recently, several researcher groups revealed that there exists a single nucleotide polymorphism within the L allele that can be further divided into LA (A variant) or LG (G variant) (212223). The former is known to yield high 5-HTT mRNA levels and LG is functionally equivalent to the low-mRNA-expressing S allele. This tri-allelic (S or LG vs. LA) approach has opened new opportunities for exploring the role of 5-HTTLPR in psychiatric researches (212425). In the present study, S or LG allele was designated as S’ whereas LA allele as L’.
COMT is a major enzyme that metabolizes catecholamines including dopamine and norepinephrine and the enzymatic activity exhibits allelic variation according to the genetic locus COMT Val158Met (2627). COMT Val allele encodes for valine, associated with high activity whereas the Met allele encodes for methionine at position 108/158. Research has shown that COMT Val158Met is associated with panic disorder (15).
Thus, the present study was to examine whether 5-HTTLPR and COMT Val158Met could be independent predictors of HRQOL in patients with PD controlling for sociodemographic data and illness-related symptomatology.
MATERIALS AND METHODS
Participants
The sample consisted of 179 panic patients with or without agoraphobia who met the diagnostic criteria in the Structured Clinical Interview for DSM-IV (SCID-IV) (28) by experienced psychiatrists. They were recruited consecutively at the Department of Psychiatry of CHA Bundang Medical Center. Age- and gender ratio-matched 110 healthy controls were recruited by local advertisement and referrals. All subjects were 18 to 70 years old, unrelated, and of Korean ancestry. Exclusion criteria included any history of schizophrenia, bipolar disorder, alcohol and substance abuse or dependence, mental retardation, and current or past serious medical or neurological disorders.
Measures
The SF-36 (1229) was used to determine HRQOL in patients with PD. It consists of eight subscales: physical functioning (the ability to perform a range of physical activities), role physical (the impact of physical health on usual role activities), bodily pain, general health (overall perception of personal health), vitality (energy and fatigue), social functioning (interference of physical and emotional problems in social activities), role emotional (impact of emotional problems on usual role activities), and mental health (psychological distress and well-being). The raw scores of SF-36 were transformed to a 0 to 100 range with higher scores indicating better HRQOL. The Panic Disorder Severity Scale (PDSS) (30) was used to assess the overall panic-related symptoms. Depressive symptoms were determined by the Beck Depression Inventory (BDI) (31).
Genotyping
Genomic DNA was extracted from blood (stored frozen) using a G-DEXTM II Genomic DNA Extraction Kit (Intron Biotechnology, Seongnam, Korea). The genotyping was based upon analysis of primer extension products generated from previously amplified genomic DNA using a chip-based matrix assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry platform (Sequenom, San Diego, CA, USA). Genotyping for the triallelic 5-HTTLPR was performed as previously described method (32) with slight modification. Traditional biallelic polymerase chain reaction (PCR) analysis yields an "S" 486 bp and an "L" 529 bp fragment. MSPI restriction enzyme digestion analysis were also performed and resulted in the following fragments: 340, 127, and 62 bp for the LA allele, 297, 127, and 62 bp for the SA allele, 174, 166, 127, and 62 bp for the LG allele and 166, 131, 127, and 62 bp for the SG allele. The COMT Val158Met was analyzed as previously described method (16).
Statistical analysis
Pearson correlation coefficients measured the linear relationship between the SF-36 subscales and age, education level, duration of illness, and clinical data. For binary measures, Student’s t-test was used to compare mean scores of the SF-36. For categorical variables with more than 2 levels, one-way analysis of variance (ANOVA) was used to compare the SF-36 scores. Hardy-Weinberg equilibrium was tested using χ2 test. The Bonferroni correction was applied for the multiple tests according to the two genetic polymorphisms. Hierarchical multiple regression analysis was performed to examine whether 5-HTTLPR or COMT Val158Met could independently predict the subscales of SF-36 controlling for age, gender, and other variables that were statistically significant in bivariate analysis. Tests were two-tailed and alpha was set at 0.05. Data analysis was conducted by using SPSS version 20 software (SPSS, Inc., Chicago, IL, USA).
RESULTS
Table 1 displays sociodemographic and clinical features of the sample. Of the 179 patients with PD, 96 (53.6%) were female, with a mean age of 39.1 years (SD = 10.6), a mean education of 12.9 years (SD = 2.9). One-hundred seven patients (65.4%) were diagnosed as PD with agoraphobia. Patients with PD showed lowered HRQOL in all sub-domains of the SF-36 compared to healthy controls. Panic patients were less educated and had less amount of monthly income. More divorced/separated/widowed subjects were in patient group. Subjects in unemployed states were more in patient group than in normal control group.
Table 1
Demographic and clinical characteristics of study subjects

In patients with PD, male gender was related with better function in terms of physical functioning, bodily pain, and vitality. Age was positively correlated with the vitality, role-emotional, and mental health. Education was associated with better QOL of physical functioning, role-physical, and bodily pain. Employment status was associated with better QOL in all subscales of the SF-36 except for role-physical and role-emotional. Patients with higher monthly income reported better QOL except for mental health. Married patients reported better role-physical, vitality, social functioning, role-emotional, and mental health compared to those who had never married. Both the PDSS and BDI were negatively correlated with all domains of the SF-36 (Table 2).
Table 2-1
Factors associated with health-related quality of life in patients with panic disorder
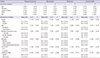
Table 2-2
Factors associated with health-related quality of life in patients with panic disorder
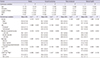
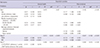
The genotype frequencies in the 5-HTTLPR and COMT Val158Met in patient group were in Hardy-Weinberg equilibrium (S’S’ = 129 [72.1%]; S’L’ = 46 [25.7%]; L’L’ = 4 [2.2%], P = 1.0 and Val/Val = 94 [52.5%]; Met/Val = 73[40.8%]; Met/Met = 12 [6.7%], P = 0.91). Panic patients with 5-HTTLPR S’S’ showed a trend to be associated with poorer general health (corrected P = 0.076) compared to L’ carriers. Patients with COMT Val/Val were significantly associated with poor role-emotional (corrected P = 0.032) (Table 2). In hierarchical multiple regression analysis, 5-HTTLPR S’S’ predicted poor general health (ΔR2 = 0.022, P = 0.018). COMT Val/Val also predicted poor role-emotional (ΔR2 = 0.015, P = 0.048) controlling for sociodemographic factors and disorder-related symptom levels (Table 3).
Table 3
Hierarchical multiple regression analysis of factors associated with quality of life in panic disorder patients
DISCUSSION
Patients with PD showed lowered HRQOL in all sub-domains of the SF-36 compared to healthy controls which is largely consistent with previous reports (345). In patient group, the tri-allelic approach of 5-HTTLPR independently and additively accounts for 2.2% of variation (6.7% of inherited variance) of general health (i.e. S’S’ with poor HRQOL). The COMT Val158Met independently and additively accounts for 1.5% of variation (5.0% of inherited variance) of role-emotional (i.e. COMT Val/Val with poor HRQOL). To our knowledge, this is the first study to examine the independent effect of specific genetic polymorphisms on the HRQOL in patients with PD. In our data, socioeconomic variables accounted for 7%-20% of each domains of the SF-36. Disorder-related symptom levels in terms of PDSS and BDI scores explained 10%-25% additionally which is largely consistent with previous results (37).
The implications of the 5-HTTLPR in panic disorder have been inconsistent. Kim et al. (33) reported no association between the 5-HTTLPR and PD in a Korean sample. Recent data of ours also suggest that even tri-allelic approach shows no direct association between the 5-HTTLPR and PD in a Korean sample (34). Taken together, the present study suggests that the 5-HTTLPR is related with specific domains (i.e., perception of general health) of HRQOL rather than with psychopathology or symptoms in patients with PD. The COMT Val158Met was not associated with the symptomatology in terms of PDSS and BDI. Thus, the COMT Val158Met is also related with specific domain of HRQOL in terms of the SF-36 (i.e. role-emotional) rather than with symptoms in patients with PD. This is consistent with previous studies showing that the HRQOL is another different domain compared to symptoms in panic disorder (4).
Interestingly, our finding suggests that different domains of HRQOL in terms of the SF-36 have a different genetic basis. It is well known that the 5-HTTLPR is closely related with 5-HT neurotransmitter system and the COMT Val158Met with dopamine and norepinephrine system (172627). Specifically, our finding means that increased serotonergic neurotransmission is associated with poor HRQOL in terms of general health while decreased catecholaminergic neurotransmission is associated with more role limitation due to emotional problems. Given that the magnitude of variance of the two genetic polymorphisms in our study was much smaller than proposed total variation of inheritance of the SF-36 (11), it is also plausible that there should be other genes that explain the rest of the variance in general health and role-emotional in patients with PD. On the other hand, it is also possible that there exist other genetic polymorphisms rather than 5-HTTLPR and COMT Val158Met that explain other domains of the SF-36.
Ethnicity and culture are important factors that should be considered. Although little is known about the ethnic or cultural effects on the profile of SF-36 in patients with PD, studies of other conditions suggest the possibility of different profile of the domains of SF-36 by different ethnicity or cultures (3536). The previous studies (3337) showed that the distribution as well as the roles of both 5-HTTLPR and COMT Val158Met in Korean panic patients are different from those in Westerners. However, in terms of the COMT Val158Met, we recently found that the frequency of COMT Val/Val is higher in the panic patient group than in normal controls (unpublished data, available at request), consistent with the results in Caucasians and contrary to the report by Woo et al. (37). Thus, further studies in other ethnic groups or cultures are warranted.
The present study has several limitations. First, our investigation about the relationship between the genetic factors and HRQOL was performed only in panic patients, not in healthy controls or other psychiatric illnesses. Thus, it is unclear whether the relationship between the 5-HTTLPR and COMT Val158Met and HRQOL in terms of the SF-36 is specific to PD. Second, our sample size was too small to examine the effect of the 5-HTTLPR L’ or COMT Met homozygotes on HRQOL. It is known that the frequencies of L or L’ allele as well as COMT Met allele in Asians (especially, in Korean and Japanese populations) are much less compared to those in Westerners (152233). Third, we used the data reported by Romeis et al. (11) in which the subjects were middle-age, middle-class Caucasians, to calculate the portion of the genetic effect in terms of inheritance of the SF-36. Finally, the significant differences in education level and job status might have played as confounding factors for explaining the between group difference in HRQOL. Further studies on the heritability of SF-36 in patients with PD as well as in Asians are needed for more accurate calculation of the proportion of variance in terms of inheritance by certain genetic polymorphisms.
In conclusion, the present study suggests that the 5-HTTLPR S’S’ independently predicts poor perceived general health (2.2% of total variation and 6.7% of variance in terms of inheritance) and COMT Val/Val are related with poor functioning in role-emotional (1.5% of total variation and 5.0% of variance in terms of inheritance) in terms of the SF-36 controlling for sociodemographic factors and disorder-related symptom levels in patients with PD. Our finding also shows that specific domains of the SF-36 are associated with the specific genetic polymorphisms that are closely related with specific neurotransmitter systems. In addition, the finding that the magnitude of explanation for HRQOL by symptom levels is not so large is consistent with the previous reports and suggests the need to include HRQOL in assessment of the patients. Finally, the total variance of prediction by sociodemographic factors, disorder-related symptoms, and the two genetic polymorphisms were all less than 40%, which warrants exploration of other factors that explain the HRQOL in patients with PD.
 XML Download
XML Download