

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The term, nontuberculous mycobacteria (NTM), generally refers to mycobacteria other than Mycobacterium tuberculosis complex and M. leprae (1). NTM are ubiquitous organisms commonly isolated from environments such as drinking water, natural water, and soil (2). Host factors, such as genetic susceptibility, immune defects, and structural lung disease, as well as environmental factors, including humidity, altitude, and shower systems may also influence the development of NTM lung diseases (134).
NTM can be divided into two groups based on their rate of growth on solid culture medium. For slowly growing mycobacteria, visible colonies are produced after 7 days, compared to within 7 days for rapidly growing mycobacteria. Slowly growing mycobacteria include M. avium complex (MAC) and M. kansasii, whereas rapidly growing mycobacteria include M. abscessus complex (MABC) (1).
The incidence and prevalence of NTM lung diseases are increasing worldwide, and they can affect both immunocompetent and immunocompromised individuals (5). In Korea, NTM lung disease was first reported in 1981 (6), and the frequency of NTM isolations from clinical specimens, and the numbers of patients with NTM lung diseases, have been increasing over recent decades (7). Given these trends, clinicians should be aware of this disease. In this article, we review the epidemiology and the clinical and radiological manifestations of NTM lung disease, as well as relevant laboratory diagnosis parameters and treatment regimens.
EPIDEMIOLOGY
The incidence of NTM lung disease is increasing worldwide. Specifically, increasing incidence and prevalence of NTM lung disease has been reported in many countries, including western countries such as the United States (8), Canada (9), and the United Kingdom (10), as well as Asian countries like Japan (11) and Taiwan (12).
Although there has been no population-based epidemiologic study on NTM lung disease in Korea, the proportion of NTM among positive mycobacterial cultures is increasing in many hospitals. Before the early 1990s, 97%-98% of mycobacterial isolates from sputum specimens contained M. tuberculosis (7). However, after the early 2000s, NTM were isolated from 20%-30% of all clinical specimens submitted to mycobacterial laboratories in many referral hospitals, and this rate further increased, to approximately 50%-70%, in the early 2010s in Korea (1314151617) (Table 1).
Table 1
Increasing proportions of nontuberculous mycobacteria of all positive mycobacterial cultures from respiratory clinical specimens in Korea

| Author, year | Hospital | Study period | Proportion of NTM in clinical isolates | |
|---|---|---|---|---|
| Start of study period | End of study period | |||
| Park et al., 2010 (13) | Seoul National University Hospital | 2002-2008 | 427/1,921 (22%) | 781/1,701 (46%) |
| Lee et al., 2012 (14) | Severance Hospital | 2006-2010 | 268/1,041 (26%) | 970/2,064 (47%) |
| Yoo et al., 2012 (15) | Asan Medical Center | 2002-2010 | 403/1,921 (21%) | 1,530/2,648 (59%) |
| Koh et al., 2013 (16) | Samsung Medical Center | 2001-2011 | 548/1,283 (43%) | 3,341/4,800 (70%) |
| Kim et al., 2013 (17) | Dankook University Hospital | 2005-2011 | 26% | 44% |
The geographic diversity of NTM species in clinical specimens is well known. A recent study analyzed NTM isolates from respiratory specimens of 20,182 patients from 62 laboratories in 30 countries across six continents (18). Across all regions, the most common NTM species is MAC, followed by M. gordonae, M. xenopi, and M. kansasii. Among rapid growers, MABC and M. fortuitum are the most commonly isolated species worldwide. However, NTM species distribution varies by region and country (18). Although MAC is the most common species in Asia as a whole, the prevalence of MABC is higher in some Asian countries, including Korea (18).
As in other counties, MAC is the most common etiologic organism (about 60%-70%) in NTM lung disease in Korea (13141920) (Table 2). While M. intracellulare has been more prevalent than M. avium in MAC lung disease in the past few years (19), M. avium has been isolated more frequently in recent years (1421). Because of advances in molecular techniques, new species have been discovered in MAC. M. chimaera is one such novel species associated with MAC, and a recent study from the United States showed that about 20% of MAC lung disease is caused by M. chimaera (22). However, the proportion of M. chimaera in MAC lung disease in Korea is unknown. MABC is the second most common etiologic organism (about 20%-30%) in NTM lung disease in Korea (Table 2). Within MABC in Korea, M. abscessus (44%-53%) and M. massiliense (45%-55%) are equally distributed, while M. bolletii is a relatively rare pathogen (1%-2%) (23242526). In addition, M. kansasii is infrequently isolated, and remains a relatively uncommon cause of NTM lung disease in Korea (272829) (Table 2).
Table 2
Common etiologic organism in patients with nontuberculous mycobacterial lung disease in Korea
| Author, year | Koh et al., 2006 (19) | Park et al., 2010 (13) | Lee et al., 2012 (14) | Jang et al., 2014 (20) |
|---|---|---|---|---|
| Study period | 2002-2003 | 2002-2008 | 2006-2010 | 2012 |
| No. of patients | 195 | 651 | 345 | 111 |
| M. avium complex | 94 (48%) | 63% | 263 (76%) | 73 (66%) |
| M. avium | 38 | NA | 141 | 32 |
| M. intracellulare | 56 | NA | 122 | 41 |
| M. abscessus complex | 64 (33%) | 27% | 63 (18%) | 32 (29%) |
| M. abscessus | NA | NA | NA | 21 |
| M. massiliense | NA | NA | NA | 11 |
| M. kansasii | 7 (4%) | NA | 7 (2%) | 1 (1%) |
| Others | 30 (15%) | 10% | 12 (3%) | 5 (5%) |
Geographic differences in the prevalence and distribution of bacterial species in NTM lung disease might be due to a combination of environmental and host immune and behavioral factors. However, environmental risk factors remain poorly understood. For example, one study reported the predominance of NTM in showerheads and the presence of MAC in nearly one-third of shower biofilm samples collected around the United States (30). Another study suggested that specific environmental factors, such as high mean daily potential evapotranspiration levels and percentage of surface water, are associated with increased incidence of NTM lung disease (4). A study of a registry of cystic fibrosis patients reported that high saturated vapor pressure is related to increased prevalence of NTM lung disease (31). The results of this study suggest that high-moisture environments might lead to large numbers of circulating aerosolized mycobacteria and an increased risk of NTM infection in patients with cystic fibrosis (31). Thus, regions with higher vapor pressure and temperatures may have an increased prevalence of NTM lung disease.
NTM disease is also an important cause of disease in immunocompromised hosts (3233), which includes patients with human immunodeficiency virus infection, malignancy, and autoimmune disease, particularly those receiving tumor necrosis factor (TNF)-α blockers. Interestingly, studies from the United States and Canada revealed that the use of TNF-α blockers is associated with an increased risk of both tuberculosis (TB) and NTM disease (3435). Similar findings have also been reported in Korea (3637).
CLINICAL AND RADIOLOGICAL MANIFESTATIONS
Pulmonary TB remains a major health concern, and the number of reported TB cases in Korea has not significantly decreased over the last decade (383940). Therefore, differentiating between pulmonary TB and NTM lung disease is important for controlling TB transmission and preventing unnecessary TB treatment in patients with NTM lung disease (41). The symptoms of NTM lung disease – cough, sputum, hemoptysis, fatigue, malaise, and weight loss – are nonspecific and similar to symptoms of pulmonary TB, and thus may also reflect underlying lung disease such as bronchiectasis and chronic obstructive lung disease. Patients with NTM lung disease are more likely to be older, female, non-smoking, and to have fewer constitutional symptoms, a history of previous TB treatment, absence of pleural effusion, involvement of the middle and lower lung zone, and bilateral disease than do patients with pulmonary TB. However, there is considerable overlap in the clinical and radiographic findings between the two conditions (4243). Therefore, additional microbiologic diagnostics are essential.
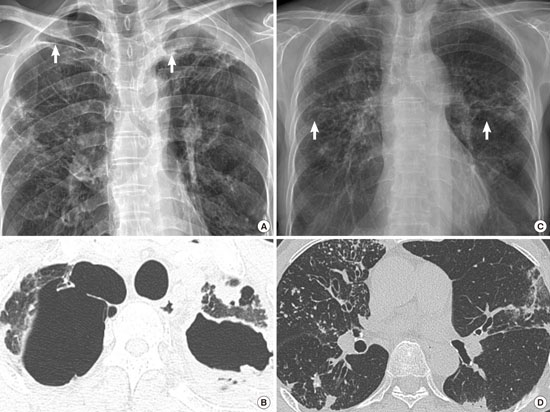
NTM lung disease has two different radiographic manifestations: fibrocavitary and nodular bronchiectatic forms (4445). Fibrocavitary forms of NTM lung disease have cavitary lesions predominantly in the upper lobes, with radiographic findings are similar to those of pulmonary TB (1) (Fig. 1A and 1B). This manifestation shows relatively rapid disease progression and frequently develops in older men with a history of smoking and underlying lung disease such as previous TB (1). The other form of NTM lung disease is nodular bronchiectatic disease. This manifestation can present as multifocal bronchiectasis, clusters of small nodules, and branching linear structures that frequently involve the right middle lobe and the lingular segment of the left upper lobe (4647) (Fig. 1C and 1D). Although these findings are quite specific for NTM lung disease, particularly MAC and MABC infections, other diseases such as diffuse panbronchiolitis may present with similar findings (4849). In the nodular bronchiectatic form of NTM lung disease, patients have unique body morphotypes, including a lower body mass index and body fat, taller stature, and increased instances of scoliosis and pectus excavatum, compared to control subjects (505152).
Fig. 1
Two distinct manifestations of nontuberculous mycobacterial lung disease: fibrocavitary and nodular bronchiectatic forms. (A, B) A 56-year-old male with Mycobacterium avium lung disease. The chest radiograph shows cavities in both upper lung fields. The chest CT shows two thin walled cavities in bilateral upper lobes. (C, D) An 83-year-old female with Mycobacterium avium lung disease. The chest radiograph shows multiple nodules in both mid-lung fields. The chest CT shows multiple centrilobular nodules with bronchiectasis in the right middle lobe and the lingular segment of the left upper lobe.

Uncommon presentations of NTM lung disease include hypersensitivity-like disease and solitary pulmonary nodules. Hypersensitivity-like disease, also known as “hot tub lung,” has been reported in relation to aerosols of infected water, including household water, medicinal baths, pools, hot tubs, and occupational exposure such as from metal-working fluids and fisheries (5354). Hypersensitivity-like disease is similar to hypersensitivity pneumonitis with respect to its clinical and radiologic presentation. Another uncommon presentation is solitary pulmonary nodules. In TB-prevalent areas, solitary pulmonary nodules with granulomatous inflammation in histological examinations are generally considered to indicate tuberculoma, and TB drugs are administered for treatment. However, solitary pulmonary nodules caused by NTM cannot be differentiated from tuberculoma by clinical, radiographic, or even pathologic examination (5556). Therefore, physicians should consider the possibility of solitary pulmonary nodules caused by NTM to prevent unnecessary treatment with long-duration TB drugs.
Clinical and microbiological criteria from the American Thoracic Society (ATS) and Infectious Disease Society of America (IDSA) are widely used to diagnose NTM lung disease (1). Clinical findings should include pulmonary symptoms and compatible radiographic evidence (nodular or cavitary opacities) and high-resolution computed tomography findings (multifocal bronchiectasis with multiple small nodules). Microbiological criteria include two positive sputum cultures, one positive bronchial wash or lavage, or compatible mycobacterial histological features such as granulomatous inflammation, positive acid-fast bacilli (AFB) lung biopsy, positive lung biopsy culture, or more than one positive sputum culture or bronchial wash (1) (Table 3). These criteria fit best with MAC, MABC, and M. kansasii; however, there is insufficient information regarding other forms of NTM to be certain that these diagnostic criteria are universally applicable for all types of NTM respiratory pathogens (1).
Table 3
Diagnostic criteria for nontuberculous mycobacterial lung disease*

AFB, acid-fast bacilli; NTM, nontuberculous mycobacteria.
*Reproduced with permission of the American Thoracic Society. Copyright © 2015 American Thoracic Society (1).
LABORATORY DIAGNOSIS
Smear microscopy is an inexpensive method for rapid detection of mycobacteria; however, it cannot differentiate NTM from M. tuberculosis (57). Therefore, detection of mycobacterial growth in culture media is necessary for definite diagnosis of NTM lung disease, although this method requires several weeks before results can be obtained. Nucleic acid amplification (NAA) assays are an excellent tool for rapid detection of M. tuberculosis directly from clinical specimens, offering higher sensitivity than smear microscopy (5859). The test can also rapidly discriminate between M. tuberculosis and NTM in smear-positive specimens (60). If the AFB smear result is positive and the NAA result is negative, the patient can be presumed to have NTM lung disease (41). Thus, NAA tests can be used as an additional test for patients with AFB smear-positive sputum for the rapid detection of M. tuberculosis and differentiation from NTM. In addition, some commercial tests are currently available that amplify different target genes to detect M. tuberculosis and several NTM species (6162).
Both liquid and solid media are recommended for mycobacterial culture to enhance the ability to detect growth of M. tuberculosis and NTM (63). Increased growth in both liquid and solid culture media is more prominent for NTM than for M. tuberculosis, especially in smear-negative respiratory specimens (64). In addition, culturing allows for the identification of NTM species, drug susceptibility tests, and genotyping of particular NTM species, and helps to assess treatment response using semi-quantitative results in solid media (65).
Identification of NTM species is very important, due to differences in clinical relevance of NTM isolates and drug susceptibilities that require different antibiotic treatment regimens. For this reason, species-level identification of NTM is recommended (64). The methods for identifying mycobacteria in clinical laboratories have changed dramatically over the past two decades. Specifically, molecular methods have now surpassed biochemical tests and high-performance liquid chromatography (HPLC) as the methods of choice for NTM identification (64). Among molecular methods, polymerase chain reaction (PCR) and restriction fragment length polymorphism analysis or PCR-reverse blot hybridization assay of the rpoB gene have been developed for use in clinical practice in Korea (41). For precise subspecies-level identification of MABC and uncommon species, sequencing of the hsp65 and rpoB genes and the 16S-23S rRNA internal transcribed spacer (ITS) region is necessary (64).
The utility of in vitro susceptibility tests for managing patients with NTM remains controversial (1). Macrolides play a key role in MAC treatment, and in vitro clarithromycin susceptibility testing is recommended for both new and previously untreated patients as well as those who fail to respond to macrolide treatment for MAC lung disease (1). Clarithromycin is recommended as the class agent for testing macrolides because clarithromycin and azithromycin share cross-resistance and similar patterns of organism susceptibility. Previously untreated M. kansasii strains should be tested in vitro only with rifampin. M. kansasii isolates resistant to rifampin should be tested against a panel of secondary agents, including rifabutin, ethambutol, isoniazid, clarithromycin, fluoroquinolones, amikacin, and sulfonamides (1). For MABC, drug susceptibility testing is difficult and of controversial merit (66). Current guidelines recommend susceptibility testing against a panel of drugs, including amikacin, cefoxitin, clarithromycin, ciprofloxacin, doxycycline, imipenem, linezolid, moxifloxacin, trimethoprim-sulfamethoxazole and tobramycin, although there is limited evidence on the applicability of the results of in vitro tests of susceptibility to the clinical response to treatment regimens based on those tests (1). With respect to in vitro susceptibility testing, MABC is typically susceptible to amikacin, cefoxitin, and clarithromycin. Macrolides are frequently the only oral agents active against MABC, and there is correlation between in vitro susceptibility and treatment response (67). However, inducible macrolide resistance was recently discovered in M. abscessus, with altered resistance to clarithromycin observed during in vitro susceptibility testing after prolonged incubation (susceptible at day 3 but resistant at day 14) or pre-incubation in macrolide-containing media (68). This inducible resistance to clarithromycin is due to a functioning erythromycin ribosomal methylase gene, erm (41), which is present in most strains of M. abscessus, but not in M. massiliense (697071).
TREATMENT
Treatment of NTM lung disease is difficult due to the uncertainty surrounding the timing of when treatment should be started and which regimen is most likely to achieve a successful treatment (1). Initiation of NTM treatment should be individualized considering disease types, comorbid conditions, and age. Patients with fibrocavitary disease usually require immediate treatment, because the presence of cavitary disease is associated with higher mortality (7273). On the other hand, nodular bronchiectatic disease tends to occur in the absence of significant comorbidity and progresses very slowly (46). Therefore, early treatment of mild and indolent nodular bronchiectatic disease may not be advisable, due to adverse drug effects from the long-term use of many drugs (1). These decisions may also be aided by molecular analyses, as specific mycobacterial genotypes within the same species have been shown to predict disease progression or treatment response in patients with NTM lung disease (7475).
Mycobacterium avium complex lung disease
Newer macrolide drugs such as azithromycin and clarithromycin are the cornerstone of MAC treatment. Specifically, current guidelines for the treatment of MAC lung disease recommend a three-drug macrolide-based therapy including macrolides, rifampin, and ethambutol (Table 4) (1). In addition, streptomycin is recommended for patients with severe and advanced disease, especially if of fibrocavitary form (1). Antibiotic therapy should be continued for at least 12 months after the conversion of sputum cultures from positive to negative. In non-cavitary nodular bronchiectatic MAC lung disease, intermittent, three-times-weekly therapy is recommended over daily therapy to improve drug tolerability (Table 4) (1). Importantly, intermittent therapy has potential benefits in decreasing adverse drug effects and medication costs, as well as in increasing treatment compliance (7677).
Table 4
Treatment regimen for nontuberculous mycobacterial lung disease

Despite advances in understanding treatment regimens and therapeutics, overall, treatment outcomes remain unsatisfactory. Specifically, patient dropout rates are 10%-30% due to adverse drug effects, and treatment success rates are only 40%-60% (7879). Furthermore, even after successful completion of antibiotic therapy, microbiologic recurrence is relatively common, mainly due to MAC reinfection (768081). Indeed, prolonged duration of treatment, drug side effects, and reinfection rather than relapse are responsible for the suboptimal treatment success rates of MAC lung disease.
Drug-drug interactions, especially those between rifampin and macrolides, can cause reduced plasma concentrations of macrolides, resulting in suboptimal responses to antibiotic treatment for MAC lung disease. Specifically, low serum concentrations of macrolides caused by drug-drug interactions are very common in patients treated for MAC lung disease with regimens consisting of both clarithromycin and rifampin (8283). However, it remains unclear whether low serum concentrations of macrolides are the reason for suboptimal treatment outcomes, and whether increasing the dose of macrolide or substituting rifampin for another drug can improve treatment outcomes for MAC lung disease.
Although there have been many studies aimed at improving treatment outcomes for MAC lung disease, and current guidelines recommend evidence-based standard treatments for this disease, current treatment outcomes remain unsatisfactory. Furthermore, the recommended regimens are associated with numerous side effects due to the use of multiple drugs and the long duration of treatment. As a result, clinician adherence to guidelines may not be very high, further contributing to poor treatment outcomes (84). Indeed, in a survey of United States physicians treating patients with MAC lung disease regarding adherence to guidelines, only 13% of the antibiotic regimens prescribed to patients with MAC met current guidelines, while 30% of the prescribed regimens were associated with an increased risk of developing macrolide resistance (84). In treating MAC lung disease, preventing the emergence of macrolide resistance is very important. Specifically, development of macrolide resistance is strongly associated with treatment failure and increased mortality (85). The most important risk factors for developing macrolide-resistant MAC are macrolide monotherapy and the combination of macrolides and fluoroquinolone without a third companion drug (85).
The value of adding additional drugs to standard antibiotic treatment of refractory MAC lung disease is unclear (86). A study suggested that clofazimine with clarithromycin and ethambutol is as effective as currently-recommended macrolide-rifampin-ethambutol therapy (87). Moxifloxacin may improve treatment outcomes in about one-third of patients with persistently culture-positive MAC lung disease who fail to respond to standardized antibiotic treatment (88). However, the role of these agents in treating refractory MAC lung disease remains unclear (86).
Although species differentiation between M. intracellulare and M. avium in terms of clinical features and prognosis were not clearly defined therein, a recent large retrospective cohort study showed that patients with M. intracllulare lung disease present more severe manifestations: lower body mass index, more frequent presence of respiratory symptoms and fibrocavitary disease, higher rate of smear-positive sputum, and worse prognosis, including more frequent initiation of antibiotic treatment during follow-up period and higher unfavorable treatment response than those in patients with M. avium lung disease (21). The same group also reported that patients with M. intracellulare lung disease showed evidence of more extensive disease in chest CT scan than did patients with M. avium lung disease (47).
Mycobacterium abscessus complex lung disease
The treatment of MABC lung disease is more difficult than that of MAC lung disease due to a lack of effective antibiotics. MABC is resistant to many antibiotics and is only susceptible in vitro to the parenteral agents, amikacin, cefoxitin, and imipenem, and to the oral macrolides, clarithromycin and azithromycin (1). Therefore, current guidelines recommend a regimen consisting of two parenteral agents and a macrolide for 2 to 4 months (Table 2) (1). However, there is little data on the efficacy and safety of this regimen, and its high cost and numerous side effects may limit its use. Several studies regarding treatment outcome in MABC lung disease have recently been reported, with positive results ranging from 25% to 88% (2467899091). However, these were retrospective studies utilizing various regimens with different treatment durations, and many patients included in these studies received treatment in combination with surgery. Therefore, the results of these studies may not be generalizable to all patients, and should be interpreted cautiously with respect to treating individuals with MABC lung disease.
A recent study differentiated MABC lung disease according to causative organism, including M. abscessus, M. massiliense, and M. bolletii (92), although the taxonomic status of MABC is still a matter of debate (93). The precise differentiation of the etiologic organisms is very important due to the high treatment success rate in M. massiliense lung disease compared to that in M. abscessus lung disease. In a recent study on this issue, negative culture conversion was achieved and maintained in 88% of patients with M. massiliense lung disease, which was significantly higher than that with M. abscessus lung disease (25%) (24). Similar results have been reported in other studies (919495).
There are currently no standard antibiotic strategies for MABC lung disease, nor are there any highly effective and safe antibiotics. For these reasons, experts believe that curative therapy for MABC lung disease may only be feasible in patients with limited disease and in combination with surgical resection and chemotherapy (9096). On the other hand, suppressive therapy using periodic parenteral antibiotics or oral antibiotics to control symptoms and progression of disease may be appropriate for the majority of patients. Recently, new treatment options for MABC lung disease have been investigated, including amikacin inhalation treatment and the novel drug bedaquiline (979899). In a preliminary study on refractory MABC lung disease, both amikacin inhalation and bedaquiline therapy, in addition to other drugs, showed encouraging results (9799). A liposomal form of amikacin inhalation therapy is currently under study for treatment of this disease (www.clinicaltrials.gov, identifier NCT01315236).
Mycobacterium kansasii lung disease
Rifampin is the most important drug in the treatment of M. kansasii lung disease due to the high culture conversion rate and low long-term relapse rate that follow drug introduction (1). Current guidelines recommend a rifampin-containing regimen in combination with isoniazid and ethambutol (Table 2) (1). This regimen is associated with a high sputum culture conversion rate and low long-term recurrence rate. In a study in Korea, the sputum culture conversion rate with rifampin-based regimens was very high, reaching 95% in patients who received antibiotic therapy for more than 12 months (28), the recommended duration of treatment after negative sputum conversion. In these cases, because antibiotic therapy produces an excellent treatment outcome, surgical resection is not recommended to treat the disease. In addition, due to the high efficacy of new macrolides against M. kansasii and the questionable role of isoniazid in the current recommended regimen, some experts are now recommending substituting macrolides for isoniazid (100).
CONCLUSIONS
The incidence of NTM lung disease is increasing worldwide. In addition, NTM species exhibit significant geographic diversity. MAC and MABC are the most commonly encountered etiologic organisms in NTM lung disease. There are two distinctive types of NTM lung disease, namely nodular bronchiectatic and fibrocavitary forms. Precise species-level identification of NTM is very important due to species-based differences in treatment regimen and prognosis. Treatment of NTM lung disease requires multiple drugs over a long course of therapy. However, treatment outcomes are routinely unsatisfactory. Thus, additional efforts to improve treatment outcome and develop new agents for NTM lung disease treatment are needed.
 XML Download
XML Download