

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Suicide is currently one of the most important mental health issues in South Korea. The suicide rate in South Korea is the highest among members of the Organization for Economic Cooperation and Development (OECD). Specifically, in 2011, the suicide rate was 31.7 per 100,000 people, which is 2.6 times greater than the OECD average and represents a two-fold increase over the last decade (1). According to the World Health Organization, elderly individuals are at greater risk for suicide than are any other age group. The rate of growth of the aged population in South Korea is one of the fastest in the world, and the suicide rate among elderly individuals in Korea is particularly high and rapidly increasing: again, in 2011, the suicide rate was 84.4 per 100,000 people in their 70s and 116.9 per 100,000 people in their 80s (2). With this significant increase in suicide rate in the elderly population, it is necessary to study the risk factors for suicide in the general elderly population.
Important changes in body composition with aging are an increase in fat mass and progressive loss of muscle mass (3). Abnormal or excessive fat accumulation—namely, obesity— is associated with mental health disorders (4). Recently, obesity has been considered a risk factor for suicide (567). However, previous studies on the association between obesity and suicide have yielded inconsistent results, and there is some confusion regarding which anthropometric measurement of obesity should be used (89). In addition to greater fat accumulation, aging results in a decline of skeletal muscle mass, called sarcopenia; this condition does not occur in isolation, but is strongly associated with an increase in fat mass (10).
Despite their enormous clinical importance, only a few studies have been conducted on the effects of body composition on suicidal ideation in the general population. Therefore, this study was conducted to assess the relationship between various indicators of body composition and suicidal ideation among the elderly population who participated in the Hallym Aging Study (HAS).
MATERIALS AND METHODS
Study population
This study was based on data acquired from the HAS, which is a population-based study of Koreans aged 45 years or older dwelling in Chuncheon, a small city in Republic of Korea. The city was divided into 1,408 areas based on the 2,000 census and 200 of these areas were randomly selected. The first-wave participants were selected via systematic sampling: 30% of subjects were sampled from individuals aged 45 to 64 years and 70% were sampled from individuals aged 65 years or older. The first-wave survey, conducted in 2003, included 1,520 participants. Among them, 918 subjects went on to participate in an in-depth clinical study in 2004. Two more follow-up examinations were in 2007 and 2010. Among the 918 participants of the in-depth clinical study, 547 agreed to participate in the 2007 follow-up examination, and 382 of these 547 participants agreed to participate in the 2010 examination. At each follow-up period, information on demographic factors, health behaviors, and medical history was obtained through face-to-face interviews using structured questionnaires. We used the 2010 HAS data, because information about suicidal ideation was obtained only in the 2010 examination. Of subjects aged ≥ 65 years, participants with any incomplete anthropometric measurements or laboratory test results were excluded. This resulted in a total of 302 subjects (139 men and 163 women) being included in the final statistical analysis.
Data collection and measurement
Anthropometric data were obtained using standardized guidelines. Body weight to the nearest 0.01 kg and height to the nearest 0.1 cm were measured with the subjects in an erect position after removing footwear. Waist circumference (WC) was measured at the end of each subject’s normal expiration to the nearest 0.1 cm at the midpoint between the lower end of the 12th rib and the upper end of the iliac crest using an anthropometric tape measure. Hip circumference was measured at the most protruding part of the hips.
Body composition including body fat percentage and appendicular skeletal muscle mass (ASM; kg) was quantified using dual-energy X-ray absorptiometry (DXA; Lunar, GE, Fairfield, CT, USA). ASM was defined as the sum of the muscle mass in the arms and legs, assuming that all non-fat and non-bone tissues were skeletal muscles.
To test muscle function, handgrip strength (muscle strength) and 6-meter usual gait speed (physical performance) were measured. Handgrip strength was measured for both hands, and each hand was measured twice. The main hand was first checked, after which participants were allowed to rest for 15 seconds; then, the other hand was checked. Handgrip strength measurement was performed using a digital dynamometer (TKK-5401; Takei, Tokyo, Japan) in kilograms, and the better numerical value of the main hand was used in the analysis. A 6-meter walk at the subject’s normal pace was timed twice, and the time of the faster of the two walks was used for 6-meter usual gait speed.
Questionnaires were administered face-to-face by trained interviewers. Socio-demographic characteristics, such as age, sex, income, and education level were obtained from the structured questionnaires. Lifestyle characteristics known to be related to suicide were also assessed, including smoking status, alcohol drinking, and regular exercise. Smoking status and alcohol drinking were classified as current or none. Regular exercise was scored as “yes” when the participant performed moderate or strenuous exercise on a regular basis. Information on medical comorbidities, which can affect sarcopenia or suicide (i.e., ischemic heart disease, stroke, or any cancer) was also obtained.
Obesity indices and sarcopenia
The obesity indices were body mass index (BMI), WC, waist-to-hip ratio (WHR), waist-to-height ratio (WHtR), and body fat percentage. BMI was calculated by dividing the body weight by the height squared (kg/m2). WHR and WHtR were calculated by dividing WC (cm) by hip circumference (cm) or height (cm), respectively. For BMI, ≥ 25.0 kg/m2 was considered obese and for WC, ≥ 90 cm in men or ≥ 85 cm in women was considered obese (11).
Sarcopenia was defined as the presence of both low muscle mass and low muscle function. Low muscle mass was defined as an ASM divided by weight (ASM/Wt) that was below the lower quintile of the study population (12). The cut-off point for low muscle mass was 25.03% in men and 20.37% in women. Low muscle function was defined by presence of low handgrip strength and/or low 6-meter usual gait speed. Low handgrip strength was defined as < 26 kg for men and < 18 kg for women, and low 6-meter usual gait speed was defined as ≤ 0.8 m/s in both sexes (12).
Determination of suicidal ideation and depressive symptoms
Suicidal ideation was assessed with the Beck Scale for Suicide Ideation (BSI). Originally, the BSI was for assessing the strength of a person’s wishes and plans to commit suicide and was completed by a clinician in a semi-structured interview (13); however, the Korean version of the BSI was modified into a self-report scale with 19 items. It shows acceptable reliability and validity (14). The items are rated on a 3-point scale from 0 to 2. The total score can range from 0 to 38, with higher scores indicating more severe suicidal ideation. A score of ≥ 9 was considered as having suicidal ideation in this study (14).
The severity of depressive symptoms was evaluated using the Korean version of the 30-item Geriatric Depression Scale (KGDS), which was standardized in 1997 after its reliability and validity were tested (15). In the standardization study, the KGDS had a correlation coefficient of 0.87 with the Geriatric Depression Scale (GDS) (16), and unlike the GDS, did not exclude an item on depressive mood related to physical aspects, because depression frequently presents as somatization symptoms in Asians, including Koreans. A score of 14 was suggested as the optimal cut-off point, with a sensitivity of 73.6% and a specificity of 72.0% (15). Subjects taking antidepressant medications or with a KGDS score of 14 or above were considered to have depressive symptoms.
Statistical analysis
Continuous data were presented as means and standard deviations (SDs), while categorical data were presented as frequencies and estimated percentages. Student’s t-test was used to compare the continuous measures, while the chi-square test was used to compare categorical measures between groups defined by sex and suicidal ideation. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated for the associations between obesity indices and suicidal ideation using logistic regression analyses. P values of less than 0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS version 21.0 software (IBM Co., Armonk, NY, USA).
RESULTS
The mean age of the study population were 75.0 years, and approximately 54.0% (n = 163) of the study population were women. Women showed a higher mean KGDS score, and more women had depressive symptoms than men (men, 46.0% [n = 64], women, 66.9% [n = 109], P value < 0.001). However, there were no significant differences in mean BSI score and presence of suicidal ideation (BSI score ≥ 9) between men and women.
The descriptive characteristics of the study population according to suicidal ideation are shown in Table 1. There were no statistically significant differences in body composition measures, including WC, BMI, WHR, WHtR, and body fat percentage between subjects with and without suicidal ideation. The prevalence of low muscle mass, low muscle function, and sarcopenia were higher in elderly subjects with suicidal ideation than in those without suicidal ideation, but these differences were not significant. Although gait speed was lower in elderly subjects with suicidal ideation than in those without it, handgrip strength did not significantly differ between the two groups. The prevalence of current alcohol drinking was higher in elderly subjects with suicidal ideation than in those without suicidal ideation, but there were no significant differences in smoking status between these groups. Subjects with suicidal ideation had a higher mean KGDS score and had a higher prevalence of depressive symptoms than subjects without suicidal ideation.
Table 1
General characteristics of study population according to suicidal ideation (n = 302)

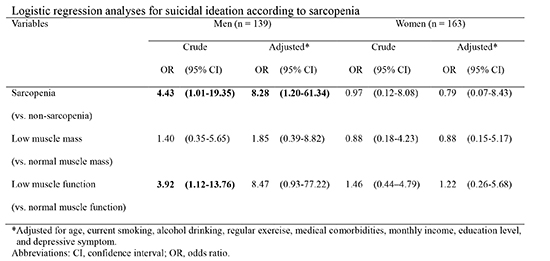
The logistic regression analyses for suicidal ideation according to obesity indices and sarcopenia are shown in Table 2. In the univariate analysis, there were no significant relationships for suicidal ideation according to obesity (defined by WC and BMI) and other body composition measures (1-unit increment for body fat percentage and 0.1-unit increment for WHR and WHtR) in both men and women. The multiple logistic regression analyses were used to determine whether the association between suicidal ideation and body composition remained significant after adjusting for other potentially confounding variables. In model 1, where age, smoking status, alcohol drinking, regular exercise, medical comorbidities, monthly income, and education level were adjusted for, the OR was significantly higher in elderly men with sarcopenia as compared with those without sarcopenia (OR, 9.00; 95% CI, 1.24–65.37). In model 2, where in the presence of depressive symptoms was also adjusted for, the OR was significantly higher in elderly men with sarcopenia as compared with those without sarcopenia (OR, 8.28; 95% CI, 1.20–61.34). However, there were no significant relationships for suicidal ideation with low muscle mass and low muscle function in the same models. In women, there were no significant relationships for suicidal ideation with sarcopenia (OR, 0.79; 95% CI, 0.07–8.43) and components of sarcopenia definition (low muscle mass and low muscle function) in the same models.
Table 2
Logistic regression analyses for suicidal ideation according to obesity indices and sarcopenia
Sarcopenia was defined as the presence of both low muscle mass and low muscle function. Model 1, adjusted for age, current smoking, alcohol drinking, regular exercise, medical comorbidities, monthly income, and education level. Model 2, adjusted for all variables in model 1 plus depressive symptom. CI, confidence interval; OR, odds ratio.
DISCUSSION
The purpose of this study was to evaluate the relationship between body composition and suicidal ideation in elderly Koreans. We found that elderly men with sarcopenia had a higher risk of suicidal ideation compared with those without sarcopenia. Only a few studies have been conducted on the association between sarcopenia and suicide, although there are several studies reporting the association between obesity and suicide. In a study where in the relationships between obesity (according to BMI), suicidal ideation, and suicide attempts were examined, obesity in men was associated with decreased suicidal ideation and attempts (5). Furthermore, a stepwise linear decrease in attempted suicides with increasing BMI was reported in a large prospective cohort study of Swedish men (9). More than 90% of all suicides are attributable to an emotional or psychiatric condition, including depression (1). In a study where in the relationships between depression and body composition were examined in elderly Koreans, depression was associated with low body mass and sarcopenia, especially in men (17). In our analysis, obesity was not associated with suicidal ideation, but elderly men with sarcopenia showed an increased risk of suicidal ideation compared with those without sarcopenia.
In contrast to the studies described above, which found a negative relationship between suicide and obesity in men, several studies showed inverse relationships in both sexes or positive relationships between BMI and suicide (6718). These discrepancies in the findings may be due to the different approaches used for assessing obesity or suicide and population characteristics, such as ethnic differences. In most studies conducted in other countries, depression was positively correlated with obesity (19), whereas an inverse relationship was reported in Korea (20). Lifestyle characteristics that can increase suicide risk, such as alcohol intake, and presence of depression, which can affect psychopathology, are also considered confounding factors. In the present study, this bias was reduced by adjusting for such variables (i.e., smoking status, alcohol drinking, and presence of depressive symptoms).
In the current study, elderly men with sarcopenia were associated with a risk of suicidal ideation, whereas no significant relationships were observed in elderly women. It means that the pathophysiology of sarcopenia or suicide would be different between the sexes. Men lose a greater skeletal muscle mass with aging, which is highly associated with other health problems relating to sarcopenia (i.e., functional decline, decreased muscle strength, and osteoporosis) than women (2122). Furthermore, there were no significant differences in presence of suicidal ideation between men and women (7.0% in men vs. 7.1% in women; P = 0.982), while women had more depressive symptoms than men (41.3% in men vs. 67.1% in women; P < 0.001). It means that contribution of depression on suicide is higher in women than men, and then the impact of sarcopenia on suicide is decreased in women. In this aspect, it is expected that women are less affected by sarcopenia relating to suicide than men.
Several different definitions of sarcopenia have been proposed in previous studies, but most studies defined sarcopenia solely on the basis of decreased skeletal muscle mass. In recent studies, a decline in muscle mass without simultaneously considering muscle function was found to be not associated with health outcomes related to sarcopenia (2324). Consequently, the Asian Working Group for Sarcopenia (AWGS) proposed an operational definition and diagnostic strategy for sarcopenia requiring measurements of both muscle mass and function (12). In this study, low muscle mass without considering muscle function was not associated with suicidal ideation, but sarcopenia as defined by the presence of both low muscle mass and low muscle function was significantly associated with suicidal ideation. Low muscle mass can be described using either the height-adjusted or the weight-adjusted definition (25). The AWGS recommends using height-adjusted skeletal muscle mass instead of weight-adjusted skeletal muscle mass (12). However, in previous studies conducted in South Korea, the height-adjusted definition showed a weak correlation with age-related muscle mass loss than the weight-adjusted definition, and the weight-adjusted definition was more closely correlated with health problems related to sarcopenia as compared with the height-adjusted definition (252627). Therefore, we selected the weight-adjusted definition for evaluating sarcopenia status in this study.
Several mechanisms could explain the relationships between sarcopenia and suicidal ideation. For instance, the high prevalence of physical illness in elderly individuals could contribute to the high suicide rate in this population (28). Sarcopenia is not a focal functional impairment but a systemic health problem that can result in poorer quality of life, unfavorable metabolic effects, and impaired cardiopulmonary performance (12). Consequently, the general physical illness resulting from sarcopenia may lead to an increased risk of suicide. In addition, central serotonergic activity influences many behaviors (e.g., eating, locomotion, reproduction, sleep, pain, aggression, and stress responses) (29). Serotonergic dysfunction, such as low levels of the serotonin metabolite in cerebrospinal fluid or altered serotonin receptor and transporter binding, has been extensively studied in adults as a possible biological marker of suicide (30). In a study in which central nervous system (CNS) serotonergic function was examined, low CNS serotonergic responsivity was associated with physical inactivity (31). Therefore, it is possible that the physical inactivity resulting from sarcopenia may induce serotonergic dysfunction, which in turn leads to an increased suicide risk.
In this study, obesity indices, which reflects fat accumulation were not associated with an increased risk of suicidal ideation. However, sarcopenia, which reflects muscle mass and muscle function was associated with an increased risk of suicidal ideation. In the aspect of prevention of suicide, rather than reduce the fat mass for obesity management, it is vitally important to sustain or improve muscle mass and function through physical activities and balanced nutrition in elderly population. Physical activities, including aerobics, endurance exercise, and resistance exercise training have been demonstrated to significantly increase muscle mass and strength in elderly with sarcopenia (32). Protein intake may also be a significant factor for preventing the development of sarcopenia. It was reported that nutritional supplements of oral amino acid mixtures increased the whole-body lean mass in elderly with sarcopenia (33). Therefore, protein supplementation in combination with adequate physical activities enhances muscle protein synthesis and improves body composition by increasing lean mass.
The present study has several limitations. First, the cross-sectional design limited us from identifying any causal relationships between variables. Therefore, a causal relationship between body composition and suicidal ideation cannot be inferred. Second, our study population may not represent the population of Korea because subjects resided in Chuncheon, a small city in Korea, and the sample size was relatively small. To minimize the effects of this limitation, participants were selected using systematic sampling from a random selection of 200 areas. Despite these limitations, our study has several advantages. On the survey of suicidal ideation, we used a validated questionnaire, the BSI, instead of a single-item question (e.g., thoughts of suicide over the previous year), and the questionnaires were administered face-to-face by trained interviewers. Furthermore, although the BMI is easy to compute and is a more economic parameter, medical examination measurements such as WC, WHR, and WHtR may be more accurate reflections of health status. As such, we included these various body composition indices in our assessment of obesity. Finally, the definition of sarcopenia was based on both muscle mass and muscle function.
In conclusion, sarcopenia was closely associated with an increased risk of suicidal ideation in elderly men. Given the prevalence of suicide in the Korean elderly population, further studies are required to examine the causal relationships between suicide and sarcopenia. Furthermore, public health interventions are needed for developing effective methods of promoting prevention and treatment of suicide in general practice.
 XML Download
XML Download