

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The capacity for empathy is important for establishing interpersonal relationships and a healthy social life (1). This is especially crucial in the medical field where clinicians need to establish both general interpersonal relationships and doctor–patient relationships (2). Although the concept of empathy is complex, empathy is currently emphasized as a tool necessary for integrating emotional and cognitive factors (3). Research shows that empathic doctors provide sensitive care to patients, thereby increasing treatment compliance and effectiveness (2). For example, a study correlating the empathic capacity of doctors with the clinical results of their diabetes patients showed a positive correlation between doctors’ empathy scores and glycated hemoglobin control of patients (4). Based on these data, researchers are emphasizing education to improve the empathic capacity of health care providers (4).
Analyses of factors influencing empathy during medical education and training have revealed variable results. Various factors have been reviewed, including type of specialty, years of clinical experience, gender, personality, and culture; however, there were differences in evaluation results even in studies using the same criteria. In research comparing the empathic capacity (according to the Jefferson Scale of Empathy) (5) of medical students and residents according to their years of education and training, empathy decreased as years of experience increased (67). Hojat et al. (4) explained this as an “erosion of empathy.” In contrast, some research reports either an increase or no difference in empathy scores as years of training increase (8910). For empathic capacity according to specialty, people-oriented specialties (POS) such as internal medicine, obstetrics and gynecology, emergency medicine, and psychiatry showed consistently higher capacities than did technology-oriented specialties (TOS) such as anesthesiology, neurosurgery, surgery, and radiology (11121314).
Burnout is one factor that can affect personnel and the quality of medical treatment. Some research suggests that reducing burnout can enhance the quality of doctors’ lives and empathic capacities; however, sample size was small and duration of observation was insufficient (15). Importantly, one study of the relationship between burnout in health care providers and their empathic capacities showed that (a) emotional burnout can result from the health care provider attempting to empathize, and (b) the absence of reward for personal achievement results in increases in depersonalization scores (16).
Most studies of empathy in the medical context have analyzed the characteristics of personnel from a single institution or from a few specialties; results were therefore inconsistent, thus limiting the ability to draw general conclusions. To overcome these limitations, our study examined the empathic characteristics of residents with various clinical specialties working in several different institutions. We also assessed whether burnout syndrome, commonly experienced by staff on medical sites, affects empathy.
MATERIALS AND METHODS
Participants
We recruited residents (first to fourth year) from 4 university hospitals located in 4 different cities: Kyung Hee University Hospital in Seoul, Keimyung University College of Medicine in Daegu, Jeju National University College of Medicine in Jeju, and Chonbuk National University College of Medicine in Jeonju. Recruitment took place from June to August 2013, with 751 residents being sent a survey and 317 (42.2%) responding. These participants were from 27 different specialty training areas.
To examine levels of empathy and burnout according to specialty, specialties were categorized as either POS or TOS. POS consisted of primary specialty areas such as those that encounter patients early on, evaluate health and disease, or supervise prevention education. Thirteen specialties were classified as POS: family medicine, tuberculosis medicine, internal medicine, pediatrics, obstetrics and gynecology, neurology, ophthalmology, preventive medicine, emergency medicine, rehabilitation medicine, psychiatry, occupational and environmental medicine, and dermatology. One hundred ninety-three participants (60.9%) were being trained in these medical specialties. TOS consisted of medical areas that require basic or applied experimental procedures, have limited access to patients, and use technical devices (14). Another 13 specialties were considered TOS: anesthesiology, radiation oncology, pathology, urology, plastic surgery, neurosurgery, otolaryngology, surgery, radiology, orthopedics, laboratory medicine, nuclear medicine, and thoracic surgery. One hundred twenty-four participants (39.1%) had specialties in this category.
Procedure
Surveys were conducted from June to August 2013. Participants completed a survey of socio-demographic characteristics, the Jefferson Scale of Empathy (Health Professional Version, Korean edition [JSE-HP-K]), and the Maslach Burnout Inventory (MBI). Participants were not compensated.
Evaluation tools
Jefferson Scale of Empathy
The Jefferson Scale of Empathy was developed by Hojat et al. (1819) to evaluate the empathic capacity of medical students and physicians. There are 2 versions: the Jefferson Scale of Empathy-Student version (JSE-S) for medical students and the Jefferson Scale of Empathy-Health Professional version (JSE-HP) for physicians. The health professional version was a modification of the student version based on the assumption that empathic attitude and empathic behavior are 2 different aspects of empathy, wherein the JSE-HP emphasizes empathic behavior more than empathic attitude. We used the JSE-HP-K because of its confirmed reliability and validity (20). The original JSE-HP consists of 20 items, whereas the JSE-HP-K consists of 18 items; 2 of the original 20 items were removed after analysis of each item and evaluation of the internal consistency reliability. Responses to the questions are provided on a Likert-type scale (scores from 1 to 7) with the highest possible score being 126. Higher scores indicate greater empathic capacity.
Maslach Burnout Inventory
The MBI (21) is a reliable and valid tool used to evaluate burnout state related to occupational stress. We used the version translated by Kang and Kim (22). The MBI consists of 22 items with 3 subscales: emotional exhaustion (EE, 9 items), depersonalization (DP, 5 items), and personal achievement (PA, 8 items). Responses are provided on a 7-point Likert-type scale from 1 (not at all) to 7 (very much). Higher levels of burnout state are associated with higher EE and DP scores and lower PA scores (23). With reverse coding of the PA scale, higher total burnout scores would be associated with more severe burnout states. The authors used the Korean version of the MBI acquired from Mindgarden (http://www.mindgarden.com/).
Data analysis and statistics
Descriptive statistics were computed for the socio-demographic variables, JSE-HP-K scores, and MBI scores. We performed a correlation analysis to examine the relationships between the psychometric study variables. A χ2 test analyzed the difference between demographic variables in each group (POS and TOS) according to the different specialties. Independent t-tests and analyses of variance (ANOVAs) were performed to analyze the differences between demographic variables, empathy according to specialty type, and burnout. Tukey’s post-hoc tests were used to further examine group differences. All analyses were performed using SPSS® (version 12.0) with the significance criterion set at P < 0.05.
Ethics statement
This study was approved by the institutional review boards of Kyung Hee University Hospital (KMC IRB 1317-01), Keimyung University College of Medicine (2013-07-013-007), Jeju National University College of Medicine (2013-07-012-002), and Chonbuk National University College of Medicine (2013-05-018-001). All participants gave written informed consent before participation.
RESULTS
Overall analysis of socio-demographic characteristics, JSE-HP-K scores, and MBI scores
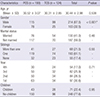
JSE-HP-K scores were significantly higher when participants were female, married, or had children (female versus male, t = -2.129, P = 0.034; married versus unmarried, t = -2.078, P = 0.038; children versus no children, t = 2.860, P = 0.005) (Table 1). JSE-HP-K scores also showed a significant difference depending on the number of siblings (P = 0.007). Post-hoc test results revealed that participants with 2 or more siblings had higher empathy scores than did those who had 1 sibling or were only children (F = 5.042, P = 0.007). For the MBI, overall, there were no significant statistical differences according to the socio-demographic characteristics of the residents.
Table 1
The comparison of JSE-HP-K and MBI scores according to socio-demographic data for all participants (mean ± SD)

Socio-demographic characteristics according to specialty
There was no significant age difference between POS and TOS groups. There were significantly more females in the POS than in the TOS group (χ2 = 14.118, P < 0.001). No significant differences were observed between groups in terms of marital status, number of siblings, and children (Table 2).
Table 2
The comparison of socio-demographic characteristics according to medical specialty type
Empathic capacity and burnout according to specialty
Covariance analysis on the effect of gender on differences in JSE-HP-K scores according to specialty showed that JSE-HP-K scores did not differ by sex in either group (F = 2.88, P = 0.091). The POS group had higher JSE-HP-K scores than did the TOS group (t = 2.259, P = 0.025); however, no differences were observed on the 3 subscales of the MBI between groups (EE, t = 0.152, P = 0.879; DP, t = 0.861, P = 0.390; PA, t = -0.750, P = 0.454) (Table 3).
Table 3
The comparison of JSE-HP-K and MBI according to medical specialty group (mean ± SD)
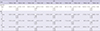
When the JSE-HP-K and MBI were analyzed according to specialty and years of training, the POS group showed higher JSE-HP-K scores in the fourth year (t = 3.349, P = 0.002); no differences were observed in MBI scores in the fourth year (EE, t = -1.194, P = 0.238; DP, t = -1.620, P = 0.111; PA, t = 1.097, P = 0.278). However, in the first year, the POS group had significantly higher scores than did the TOS group on the DP subscale of the MBI (EE, t = 1.366, P = 0.175; DP, t = 2.183, P = 0.031; PA, t = -0.486, P = 0.628).
Empathic capacity and burnout according to years of training
Overall, there was no significant difference in JSE-HP-K scores (F = 0.583, P = 0.626) or MBI scores (EE, F = 1.270, P = 0.285; DP, F = 0.646, P = 0.586; PA, F = 0.330, P = 0.804) according to years of training (Table 4). A sub-analysis assessed differences according to years of training in the POS and TOS groups and showed a significant difference in JSE-HP-K scores according to years of training in the POS group (F = 3.166, P = 0.026). Post-hoc analysis (using Tukey’s test) showed that fourth year JSE-HP-K scores were significantly higher than were first year scores (F = 3.166, P = 0.026). No significant differences were found according to years of training in the TOS group for either JSE-HP-K scores or MBI scores.
Table 4
The comparison of JSE-HP-K and MBI according to grade (year of training) in each specialty (mean ± SD)
*P < 0.05. JSE-HP-K, Jefferson Scale of Empathy, Health Professional version, Korean edition; MBI, Maslach Burnout Inventory; SD, standard deviation; POS, patient-oriented specialties; TOS, technology-oriented specialties; n.s., statistically nonsignificant; EE, emotional exhaustion; DP, depersonalization; PA, personal achievement.
Correlation between empathic capacity and burnout
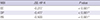
Overall, the JSE-HP-K showed a negative correlation with the EE and DP subscales of the MBI (EE, r = -0.277; DP, r = -0.447) and a positive correlation with the PA subscale (r = 0.500) (Table 5). A similar pattern was observed for separate analyses of the POS (EE, r = -0.313; DP, r = -0.518; PA, r = 0.475) and TOS (EE, r = -0.228; DP, r = -0.364; PA, r = 0.567) groups.
DISCUSSION
A main result of our study was that female medical residents had significantly higher empathy scores than did male residents. This is consistent with early reports that females have better empathic capacity because they perceive emotional signals better than males and have a better understanding of others (24). This might be explained by the “nurturing investment” theory, which proposes that females develop greater empathic capacity because they nurture offspring (24). However, in our previous studies, we found no gender-based differences in empathy scores (91725) and the same trend was reported in studies of physicians in Italy (26) and medical students in Iran (27). Therefore, the concept of gender differences in empathic capacity remains controversial.
In the present study, married residents had significantly higher empathy scores than did single residents. This is consistent with our own research showing that, for residents specializing in psychiatry, empathy scores were higher for married than for single residents (9). Indeed, Crowell et al. (28) claimed that marriage has a positive effect on emotional development.
A further key finding was that empathy scores were higher for residents with their own children. To our knowledge, our study is the first to assess the relation of empathic capacity with whether or not residents have children. We also found that residents who had 2 or more siblings showed higher empathy scores than did those who had one or no siblings. Lam et al. (29) have reported that siblings influence each other’s socio-emotional development and may act as a factor contributing to the socialization process. It is not known whether the relationship between siblings promotes development of empathy or whether the empathic capacities of siblings promote positive interactions. However, having many siblings does appear to increase the odds of promoting socio-emotional development. Conversely, Lam et al. (29) proposed that sibling conflict may act as a negative factor in the development of empathy development and Kitamura et al. (5) reported that nurturing by parents declines as the number of siblings increases. Thus, both the number of siblings and the qualitative aspect of sibling relationships can act as critical factors for empathy development.
With regard to type of specialty, our study showed differences in empathy scores between POS and TOS groups even when the difference in gender ratio was taken into account. One explanation for the higher empathy scores in POS physicians is that the POS group has more opportunity for direct contact and conversation with patients, thus emphasizing interpersonal relationships (30). However, it has also been reported that the interpersonal skills of physicians in the POS group may be different from those of the TOS group even before choosing a specialty; that is, their choice of a suitable specialty may be reflected in later empathy scores (31). Our finding that, in the TOS group, there was no difference in empathy scores according to years of training indirectly supports the view that TOS physicians choose specialties suitable for themselves according to their interpersonal skills.
We also found that longer duration of training significantly increased empathy score in the POS group. This finding is consistent with a study of the empathic capacity of psychiatry residents (9) but contradicts the findings of Bellini and Shea (32) concerning surgery residents. In the latter study, as duration of training increased, “personal distress” decreased. However, “acceptance of view” and “empathic interest” (variables related to empathic capacity) were maintained at a continuously low level. We propose that to understand changes in empathy score according to years of training, it is necessary to verify occupational characteristics and socio-cultural differences during each year of training. We also recommend that further studies (based on such characteristics and differences) should be carried out to determine the factors influencing empathic capacity.
Changes in patterns of empathy according to years of residency are diverse and are similar to the changes in patterns of empathy according to year of medical school. Studies by Chen et al. (6) at Boston University School and Hojat et al. (7) at Jefferson Medical College both reported a decrease in empathy scores as time in medical school increases. Contrary to these findings from the United States, a study of empathic capacity of medical students in Korea (25) and a follow-up study on the same group after a year (17) found positive correlations between empathy and number of years in medical school. Other studies from the United States (33) and Japan (34) also revealed that clinical experience does not have negative effects on level of empathy and that there is a positive correlation between empathy and years of education. Feighny et al. (35) and Wilkes et al. (36) have also demonstrated positive effects of clinical experience and educational training on empathy. At least one study using a control group of non-medical personnel has shown that, for medical students and physicians, clinical experience (rather than medical education) has an impact on empathy development and seems instrumental in maintaining empathetic skills (37). Although it is difficult to show a causal relationship, the observed increases in empathy scores in the present study might be related with education course “Physicians in Society”, which has been included in the Korean standard medical education curriculum for 3 years (17).
Even considering that the JSE-HP-K was composed of 18 items (2 fewer than the usual 20), the mean score for Korean physicians (POS, M = 94.95, SD = 13.10; TOS, M = 91.48, SD = 13.76) was lower than those in previous studies of young physicians in the United States (M = 120, SD = 12) (19), Italy (M = 115, SD = 15.55) (26), and Romania (M = 113.4, SD = 14.4) (15). The reason for this discrepancy may be the hierarchical nature of the Korean physician–patient relationship (influenced by Confucian philosophy), which makes expression of empathy less important (38). Future studies should take this difference into account.
Our analysis (including all participants) of the JSE-HP-K and MBI subscales revealed that JSE-HP-K scores were negatively correlated with the EE and DP subscales of the MBI and positively correlated with the PA subscale. This is consistent with the findings of Walocha et al. (39), who showed that, for people with burnout syndrome, there were negative effects of EE and DP on empathic capacity. Collectively, these results are also similar to those of a study with medical students showing that high burnout scores were associated with lower empathy scores (23). The burnout rate among students graduating from medical school is close to that of private practice physicians (about 20%), in line with results of a German study showing that burnout leads to a decrease in self-reported empathy scores (40).
Although the present study was designed to address the weaknesses of previous studies, some limitations should be reported. First, due to cross-sectional data collection, the present study was limited to analyzing empathy by group rather than measuring change in individual medical residents. Second, because resident training programs vary depending on country, hospital, and clinical specialty, it is possible that workload or psychological burden also varies. For an accurate assessment of changes in empathic capacity, it is necessary to modify variables such as a resident’s “occupational analysis.” Third, the present study used the JSE-HP-K, which was modified from the original JSE-HP to contain 18 items instead of 20; this should be taken into account when interpreting comparisons with other studies. Fourth, some residents did not participate in the study and although the exact reason is unknown, we may assume that there was a selection bias of residents who are more interested in the subject 'empathy', are more likely to participate in the study.
Despite the aforementioned limitations, our study is important because it is the first to examine the correlation between empathic capacity and burnout characteristics in medical residents from multiple institutions and with 27 different clinical specialties.
 XML Download
XML Download