

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bronchopulmonary dysplasia (BPD), a chronic lung disease in premature infants that requires prolonged ventilator and oxygen therapy, is a serious complication of preterm birth (12). BPD remains a major cause of mortality and lifelong morbidity in premature infants because only few therapeutic measures are available to prevent or ameliorate this common and serious disorder (34). The most severely affected infants were the most premature, particularly infants born at 23–26 weeks gestation. Recent advances in neonatal intensive care medicine have resulted in improved survival of infants born as early as 23–24 weeks gestation and therefore, the actual number of extremely premature infants at high risk for developing BPD might be increasing. Consequently, improved survival of extremely preterm infants might be closely linked to increasing rates of BPD (56). However, other researchers have reported stable, or even reduced, BPD incidences (789). Overall, the role of improved survival in the development of BPD remains largely controversial, and further studies are necessary to clarify this.
Recently, we have noted markedly improved survival rates with improvements in perinatal and neonatal intensive care in extremely preterm infants, especially those born at 23–24 weeks gestation (101112). Therefore, in the present study, we investigated whether improved survival was associated with the altered incidence of BPD, and if applicable, the clinical factors responsible for this alteration.
MATERIALS AND METHODS
The medical records of 350 preterm infants at 23–26 weeks gestation who were born and admitted to the neonatal intensive care unit (NICU) at Samsung Medical Center from January 1, 2000 to December 31, 2005 (period I, n = 137) and January 1, 2006 to December, 2010 (period II, n = 213) were retrospectively reviewed. The study periods were divided according to the survival rate, and infants were stratified into the 23–24 and 25–26 weeks gestation subgroups.
Maternal and neonatal characteristics, mortality and various major morbidity rates until discharge were assessed in the 23–24 and 25–26 weeks gestation subgroups during the study periods. The survival rate was assessed until discharge from the NICU. The traditional definition of BPD, oxygen use at postmenstrual age of 36 weeks (13), was used in this study; this was equivalent to moderate to severe BPD as determined by using the National Institutes of Health Workshop severity-based diagnostic criteria (14). In the present study, we evaluated the incidence of BPD in association with the survival rates of patients; BPD was assessed only in the survivors until NICU discharge. Subgroup analyses for infants at 23–24 and 25–26 weeks gestation were performed throughout the study periods. To identify the responsible associated factors for the changes in total mortality and BPD incidence in the survivors according to period, univariate and subsequent multivariate analyses were conducted with various clinical factors. The following variables were analyzed for the analysis of clinical factors: period, gestational age (GA), birth weight, male, appropriate for gestational age (AGA), Apgar score at 5 min, histologic chorioamnionitis, pregnancy-induced hypertension (PIH), antenatal and postnatal steroid therapy, respiratory distress syndrome (RDS), patent ductus arteriosus (PDA) at week 1, intraventricular hemorrhage (IVH) grade ≥ 3 (15), necrotizing enterocolitis (NEC) stage ≥ 2b (16), retinopathy of prematurity (ROP) stage ≥ 3 (17), neonatal sepsis, duration of total parenteral nutrition (TPN), intubation, continuous positive airway pressure (CPAP), and supplemental oxygen therapy (11). GA was determined by the last maternal menstrual period and modified Ballard test. AGA was defined as a birth weight between the 90th and 10th percentiles. RDS was defined as requiring surfactant and ventilator treatment or clinical features of RDS within the first 24 hours or birth. Neonatal sepsis was defined as a positive blood culture in symptomatic infants with antibiotic treatment.
Statistical analyses
Continuous variables were expressed as means ± standard deviations; categorical variables were expressed as numbers and percentages. Categorical variables were compared using the chi-square test or Fisher’s exact test, and continuous variables were compared using the Mann-Whitney U test or Student’s t-test. Logistic regression analysis was performed to control for all variables and estimate the independent significant risk factors associated with death or BPD. A P-value of < 0.05 was considered statistically significant. The adjusted odds ratio and 95% confidence interval for each possible risk factor were calculated. The software package SPSS version 17 (IBM Corp., Armonk, NY) was used for all statistical analyses.
RESULTS
Changes in demographic characteristics
The characteristics of the newborns according to subgroups and study periods are shown in Table 1. The GA and birth weight of infants were not significantly different in infants at 23–26 weeks between periods I and II. The Apgar score at 5 min and antenatal steroid use in all infants were significantly higher during period II compared to period I, especially in infants at 23–24 weeks gestation. Other variables, including male sex, AGA, histologic chorioamnionitis, and PIH were comparable in the subgroups between study periods.
Table 1
Comparison of demographic characteristics in enrolled infants according to period*

Changes in management factors during NICU care
The management factors during periods I and II are shown in Table 2. The duration of CPAP, TPN, hospital days, and antibiotics days in all infants was significantly higher during period II compared to period I. Moreover, the duration of CPAP, supplemental oxygen, antibiotics days, postnatal steroid use, and hospital days in infants at 23–24 weeks gestation was significantly higher during period II compared to period I. By contrast, a lower duration of intubation and supplemental oxygen were observed in infants at 25–26 weeks gestation in period II compared to period I.
Table 2
Comparison of neonatal intensive care management factors in enrolled infants according to period*

Changes in survival rate, BPD incidence, and other morbidity rates
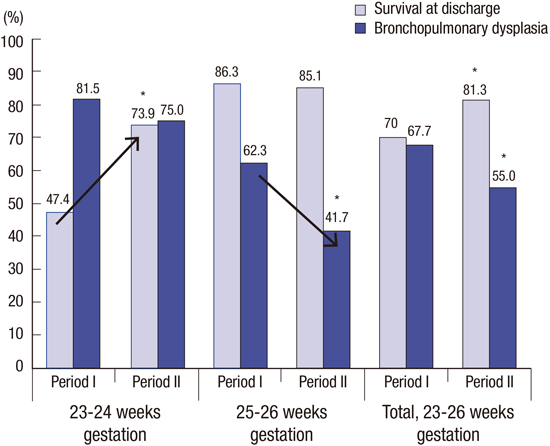
The mortality, BPD incidence, and other morbidity rates among infants during period I and II are shown in Table 3. The survival rate at discharge in infants at 23–26 weeks gestation was significantly improved during period II (80.3%, 171/213) compared to that during period I (70.0%, 96/137). In subgroup analyses, a significantly increased survival rate was observed during period II (73.9%, 68/92) compared to that in period I (47.4%, 27/57) in the 23–24 weeks gestation subgroup. However, there was no significant difference in the survival rate of infants in the 25–26 weeks gestation subgroup between periods I (86.3%, 69/80) and II (85.1%, 103/121).
Table 3
Comparison of mortality and incidence of bronchopulmonary dysplasia and other morbidities in enrolled infants according to period

In contrast, the incidence of BPD in survivors was improved during period II (55.0%, 94/171) compared to that in period I (67.7%, 65/96). The 25–26 weeks gestation subgroup had a significantly reduced incidence of BPD in period II (41.7%, 43/103) compared to period I (62.3%, 43/69). However, there were no significant differences in the incidence of BPD in infants in the 23–24 weeks gestation subgroup. Increased survival at discharge in premature infants at 23–24 weeks gestation was not associated with increased incidence of BPD in infants at 23–24 weeks gestation (Fig. 1).
Fig. 1
Survival rate and incidence of bronchopulmonary dysplasia in extremely preterm infant survivors according to time period. The overall survival rate was improved in period II compared to that in period I, especially in infants at 23–24 weeks gestation. The BPD incidence in survivors was decreased during period II compared to that in period I, especially in infants at 25–26 weeks gestation. Improved perinatal and neonatal care can simultaneously lead to improved survival and decreased incidence of bronchopulmonary dysplasia. *P < 0.05.

The incidence of neonatal sepsis in infants at 25–26 weeks gestation was significantly lower during period II (15.7%) compared to period I (32.9%; P = 0.004). The incidences of RDS, PDA, IVH grade ≥ 3, NEC stage ≥ 2b, and ROP stage ≥ 3 were not significantly different in the subgroups between study periods.
Associated factors for mortality and BPD
The univariate analysis of possible associated factors for mortality and BPD in survivors is shown in Table 4. For adjustment of confounding factors, multivariate analysis was conducted for mortality and BPD with factors that were confirmed significant in the univariate analysis.
Table 4
Univariate analysis of associated factors for mortality and bronchopulmonary dysplasia in survivors
OR, odds ratio; CI, confidence interval; BPD, bronchopulmonary dysplasia; y/n, yes/no; AGA, appropriate for gestational age; RDS, respiratory distress syndrome; PDA, patent ductus arteriosus; CPAP, continuous positive airway pressure; TPN, total parenteral nutrition; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis.
The adjusted odds ratio and 95% confidence intervals for these factors analyzed by multivariate linear regression are shown in Table 5. A larger birth weight (per 100-g increment), higher Apgar score at 5 min, and maternal use of antenatal steroid before delivery were negatively associated with mortality in infants at 23–26 weeks gestation. A longer duration (per week) of intubation and supplemental oxygen were significantly associated with the development of BPD in survivors. In contrast, prolonged use of less invasive CPAP (per week) was protective against the development of BPD in survivors.
Table 5
Multivariate analysis of associated factors for mortality and bronchopulmonary dysplasia in survivors

DISCUSSION
In the present study, the survival rate in extremely preterm infants at 23–26 weeks gestation was significantly improved during period II compared to that in period I, which was mostly attributable to improved survival in infants born at 23–24 weeks gestation. This improved survival of extremely preterm infants was not associated with increased incidence of BPD at 23–24 weeks gestation. Furthermore, the incidence of BPD in survivor infants at 25–26 weeks gestation was significantly decreased during period II compared to period I. Possible factors responsible for these changes include higher antenatal steroid use and improved 5-min Apgar scores, which were associated with improved survival in infants at 23–24 weeks gestation. In addition, earlier extubation, less oxygen supplementation, and increased less invasive nasal CPAP use were associated with reduced BPD incidence, especially in infants at 25–26 gestation.
The association between the increased survival of preterm infants and BPD remains a controversy. A lower GA at delivery, especially ≤ 26 weeks gestation, which results in extreme structural and biochemical lung immaturity, is the most powerful risk factor for the development of BPD (181920). Increased survival of extremely premature infants might increase the actual number of premature infants at risk for BPD (5212223). However, increased survival of extremely preterm infants at 23–24 weeks gestation was associated with reduced incidence of BPD in infants at 25–26 weeks gestation at our NICU setting. Botet et al. (1) reported that there was no increase in the survival of extremely low birth weight infants; however, the survival of infants without BPD increased from 58.5% in 1997–2000 to 75% in 2006–2009. According to these findings, better perinatal and neonatal intensive care for improving survival of extremely preterm infants also simultaneously reduces the incidence of BPD in these infants (2425). Currently, few effective treatments are available for treating BPD. However, marked variation in the BPD incidence rates among medical centers and some reported success in reducing the BPD incidence rate within individual hospitals through quality improvement efforts suggest that identification and implementation of specific neonatal intensive care practices could modify the incidence of BPD (26272829). In the present study, early CPAP after having early extubation and reducing supplemental oxygen use were independent effective strategies identified for reducing the incidence of BPD. Intubation and ventilation could induce volutrauma and barotrauma, and the use of less invasive CPAP could allow continuous alveolar growth, which might consequently reduce lung damage (30). Other possible risk or preventive factors for BPD, including birth weight, nosocomial sepsis, PDA, postnatal steroid use, and nutrition (3132) were not significantly associated with the development of BPD in the present study. Collectively, these findings suggest that although the ‘magic bullet’ for preventing and/or treating BPD might not exist, the implementation of combined clinical practices, including reduced oxygen exposure, early extubation and less invasive CPAP, might be an effective strategy for reducing BPD among extremely preterm infants (33).
This study had several limitations, including its retrospective nature and the relatively small sample size of infants born at 23–24 weeks gestation during period I. In addition, although “period” was included as an independent factor for multivariate analysis for the effect, unknown confounders might not be controlled in this retrospective study. Another limitation was that the results were obtained from a single institution and therefore, our findings might not be generalizable to another NICU. However, a strength of this study was the relatively large sample size of infants at 23–26 weeks gestation (n = 350) with similar baseline characteristics who were born at a single institution. Furthermore, possible factors responsible for these outcome changes were confirmed using both period comparison and risk factor analysis in the present study. In period II, increased antenatal steroid use and higher 5-min Apgar scores, which were confirmed as associated factors for improved survival were demonstrated in infants at 23–24 weeks gestation; these infants had significantly improved survival rates compared to those in period I. Earlier extubation and less oxygen supplement with increased nasal CPAP use, which were associated factors confirmed to be responsible for protecting against BPD, were also demonstrated in period II in the 25–26 weeks gestation subgroup; the BPD incidence was significantly lower compared to period I in these infants.
In conclusion, infants born at 23–26 weeks gestation had improved survival rates, which was mostly attributable to improved survival of infants born at 23–24 weeks gestation. Simultaneously, the incidence of BPD in survivors was reduced in infants born at 23–26 weeks gestation, which was mostly attributable to decreased BPD incidence in infants born at 25–26 weeks gestation. In this study, improved survival of extremely preterm infants born at 23–24 weeks gestation may be associated with reduced incidence of significant BPD in survivor infants born at 25–26 weeks gestation. These findings are in agreement with those of other studies in which the quality of life was improved in extremely preterm infants. The development of perinatal and neonatal care improved the survival of immature preterm infants and simultaneously decreased morbidities in mature preterm infants (3435). Collectively, aggressive perinatal and improved neonatal care can simultaneously lead to improved survival and decreased BPD incidence in extremely premature infants.
 XML Download
XML Download