

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatocellular carcinoma (HCC) is the fifth most common cancer and the third leading cause of cancer-related deaths worldwide (12). In Korea, HCC is the fourth and sixth most common cancer in men and women, respectively, and over 15,000 new cases occurred in 2009 (3). HCC accounts for 75-90% of all primary liver cancers (345). HCC was the second leading cause of cancer mortality in Korea, but the overall 5-year survival rate of HCC patients has improved from 10.7% to 28.6% in 2013, according to the national cancer center (6).
There are various treatment options for HCC. The proportion of patients undergoing curative therapies including hepatic resection, liver transplantation, and locoregional therapy has been increasing over the last decade. Several studies have demonstrated that transarterial chemoembolization (TACE) improves the survival rate (78). Radiotherapy for HCC has become more common as radiation technology has developed rapidly and high-dose radiotherapy without broad liver damage became available. The introduction of sorafenib, which lengthened survival, opened a new era of chemotherapy for HCC patients (910).
The treatment of HCC is very complicated since HCC is heterogeneous and treatable by various modalities in the same stage. The Barcelona Clinic Liver Cancer staging system, which is used commonly, is helpful for conceptualizing the different treatment options, but may not be applicable in all settings. Moreover, the Barcelona Clinic Liver Cancer staging system guideline is only for initial treatment. There are no re-treatment guidelines for HCC patients.
There is no large-scale population-based study on HCC treatment trends. We aimed to assess the trends of initial treatment and re-treatment modalities for Korean HCC patients on the basis of data taken from national data from the Health Insurance Review and Assessment Service (HIRA) between 2008 and 2012.
MATERIALS AND METHODS
Data source
We used data from the Korean HIRA, which includes adjusted medical and pharmacy claims for almost the whole Korean population. Korea has a health care system that is managed and supervised by the government; 97.0% of the population is legally obliged to register in the Korean National Health Insurance Program. All medical clinics and hospitals must submit data of inpatients’ and outpatients’ care, including diagnoses (coded according to the International Classification of Disease, Tenth Revision [ICD-10]), procedures, prescription records, demographic information, and direct medical costs, to HIRA to claim back medical costs from the government.
Patient selection
All HCC-related hospital visits or admissions were recorded in the aforementioned system using ICD-10 codes between January 2008 and December 2012. To identify newly diagnosed HCC patients, ICD-10 codes (C220) were selected and patients with previously diagnosed HCC were excluded.
Data analysis
Data regarding age, gender, etiology, and underlying liver cirrhosis were ascertained by a medical records’ review. The annual incidence was determined using the aforementioned patient selection criteria and the annual HCC prevalence was defined as the number of patients who retained the C220 code for 1 year. The following 3 institutional types were defined according to the national medical law: the clinic was defined as a facility with more than 30 beds, the general hospital was defined as a facility with more than 100 beds and a certain number of experts, and the tertiary hospital was defined as a general hospital with highly trained medical practitioners specializing in severe diseases.
Patients received 1 of the following treatments: hepatic resection, liver transplantation, radiofrequency ablation (RFA) therapy, percutaneous ethanol injection, transarterial chemoembolization (TACE) therapy, hepatic artery chemoinfusion therapy, external-beam radiation therapy, systemic cytotoxic chemotherapy, molecular-targeted therapy (sorafenib), and conservative management. All hospitals and clinics were listed in the HIRA database and used the same procedure, medicine, and surgery codes. The initial treatment modality was defined as the first treatment modality after diagnosis and was analyzed annually. Combination treatment was defined as 2 different treatment modalities administered within 30 days.
Treatment trends after initial treatment were only available from 2009 because HIRA only provided data for the most recent 5 years and analysis was performed according to the 3 most common modalities (hepatic resection, liver transplantation, and local ablation therapy). The follow-up period was 3-4 years.
Subgroup analysis of sorafenib therapy was performed in 2011 and 2012. The initial doses, 800 mg and 400 mg, were analyzed separately. The mean daily dose was calculated by dividing the total administration dose by the total number of patients and days. The median treatment duration was analyzed using each patient’s total prescription days.
RESULTS
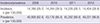
From January 2009 to December 2012, 57,690 persons were newly diagnosed with HCC, which constituted the final study population. During the study period, the annual incidence of HCC was approximately 14,000 cases per year and did not significantly change over time, while the prevalence gradually increased (Table 1).
Table 1
Incidence and prevalence rates (per 100,000 people per year) of hepatocellular carcinoma
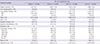
The mean age was the late fifties (57-60 years) and the majority of the patients were men. More than half of the patients were diagnosed in tertiary hospitals. The main etiology of HCC was hepatitis B virus (HBV) infection (47.9-50.2%) and this proportion did not significantly change over time. Half of the patients had accompanying liver cirrhosis. Overall, the extrahepatic metastasis rate was about 10% and the most common site was the lung, followed by the bones and the lymph nodes (Table 2).
Table 2
Demographic features of newly diagnosed hepatocellular carcinoma patients

The initial treatment was usually performed in tertiary hospitals (approximately 70%) and there was no significant change during the study period. However, more patients visited tertiary hospitals after the diagnosis. The median period from diagnosis to initial treatment was 22 days (range 14-36 days). TACE was the most common initial treatment modality (29.3-33.0%). The use of curative treatment modalities (hepatic resection, liver transplantation, and local ablation therapy) gradually increased from 17.7% to 22.1% during the study period. Sorafenib therapy has been used in about 3.5% of HCC patients since 2011. Combination treatment accounted for about 4% of patients every year, and TACE plus radiotherapy and TACE plus RFA were performed commonly. The patients who did not receive treatment decreased over time, after the diagnosis (Table 3).
Table 3
Initial treatment modalities
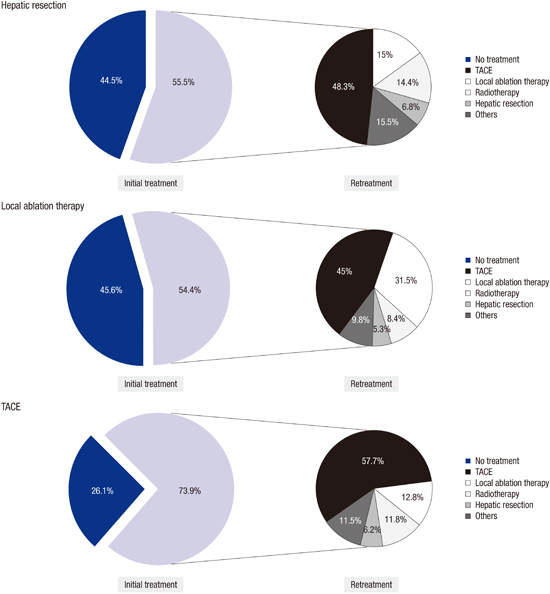
Re-treatment trends were evaluated in HCC patients who first received treatment in 2009 (Fig. 1). In patients who underwent hepatic resection initially, 44.5% of patients received the same or other treatments over the study period. The most common treatment modality was TACE (48.3%), followed by local ablation therapy (15.0%) and radiotherapy (14.4%). Hepatic resection was repeated in 6.8% of patients. In patients initially treated with local ablation therapy, 54.4% of patients received re-treatments during the study period. The most common modality was TACE (45.0%), followed by local ablation therapy (31.5%) and radiotherapy (8.4%). Hepatic resection was performed in 5.3% of patients. In patients initially treated with TACE, 73.9% of patients were re-treated and the most common modality was TACE (57.7%), followed by local ablation therapy (12.8%) and radiotherapy (11.8%). TACE was performed 0.8 times/year. Hepatic resection was performed in 6.2% of patients who initially underwent TACE.
Fig. 1
Treatment trends after initial treatment in 2009. Treatment trends after initial treatment were analyzed for 3 of the most common initial treatment modalities (hepatic resection, local ablation therapy, and transarterial chemoembolization [TACE]).

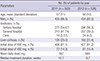
Sorafenib has been used widely since 2011, when the reimbursement policy was applied. In 2011 and 2012, the majority of HCC patients received sorafenib in the general or tertiary hospitals. About 25% of patients had extrahepatic metastases. The majority of patients received the standard dose of 800 mg (81%). The mean daily doses were 667 mg and 680 mg in 2011 and 2012, respectively. The median treatment durations were 10.7 weeks and 8.7 weeks, respectively (Table 4).
Table 4
Subgroup analysis of sorafenib administration in 2011 and 2012
DISCUSSION
This study is a nationwide cross-sectional study undertaken to evaluate the trends and patterns of HCC treatment in Korean patients. The prevalence of HCC has gradually increased from 40,908 in 2009 to 49,221 in 2012. The increasing prevalence of HCC seems to be caused by the increased survival time of Korean HCC patients according to the national cancer registry’s report (6).
The etiology of HCC was mostly HBV infection. HBV infection caused 50%, while hepatitis C virus infection and alcohol caused 11% and 10-11% of HCCs, respectively. The proportion of cases accounted for by HBV infection was lower than that reported by other studies (1112). However, considering that the etiology for about 30% of cases was not known and that HBV infection accounted for about 50% of the cases reported in this study, this study is not different from other reports. Extrahepatic metastases of HCC occurred in 9-10% of the patients and HCC frequently spread to the lungs, bones, lymph nodes, adrenal glands, and brain. The rate of metastasis was lower than that in other reports; about 30–50% of patients presented with metastases (13). The lower rate might be due to lower recording as a result of physicians’ unawareness of clinically insignificant metastatic lesions.
Initial treatment seems to start early in Korea. The period from diagnosis to initial treatment was 14-36 days. The majority of patients received initial treatment within 30 days of diagnosis. The proportion of patients who received curative treatments (hepatic resection, liver transplantation, local ablation therapy) increased slightly from 17.7% in 2009 to 22.1% in 2012. At the same time, the proportion of patients who received supportive care decreased during the study period, from 41.6% to 36.6%. The increase in curative treatment is probably caused by earlier HCC detection due to physicians’ awareness of HCC surveillance in high-risk patients and the nationwide check-up program.
TACE was the most common modality for initial treatment in Korea and is used more frequently than in other countries (14). Generally, single drug chemotherapy was used with TACE. Doxorubicin accounted for 80% and cisplatin for 15% of cases. TACE with 3 chemotherapeutic agents is routinely administered in other countries and a recent large randomized controlled trial showed that TACE with 3 chemotherapeutic agents increased the overall survival (15). The reimbursement policy permits the use of only 1 chemotherapeutic agent in Korea, which possibly led to a different practice environment.
Combination treatments accounted for about 4% of cases every year. TACE plus radiotherapy and TACE plus RFA were performed commonly. Combination therapies are expected to increase based on several recent studies, which report that combination therapies including TACE plus radiotherapy, showed better results for advanced HCC patients compared to monotherapy and combination of TACE with RFA could improve the survival rate (16).
A small proportion of HCC patients received systemic cytotoxic chemotherapy. The most frequently used monotherapeutic agent was 5-fluorouracil. Combination therapy with 5-fluorouracil and cisplatin, or cisplatin and gemcitabine was used most frequently. These chemotherapeutic agents have not demonstrated efficacy in HCC, although they reportedly increased survival time in several solid gastrointestinal tumors. Physicians still seemed to prefer systemic chemotherapy for treatment-refractory advanced HCC patients. This practice lasted until 2012, even after sorafenib, an effective molecular-target agent, was introduced in Korea. This study did not show whether systemic chemotherapies were administered in patients who were sorafenib-naïve or sorafenib-refractory.
Sorafenib, a molecular target therapy, was introduced in 2007 in Korea, while the reimbursement policy has been implemented since 2011. According to the reimbursement policy data, sorafenib accounted for about 3.5% of all treated patients in 2011 and 2012. Subsequently, sorafenib use has presumably become more common due to the expanded reimbursement policy in force since 2013.
In HCC patients, there are several treatment modalities that are curative or palliative. The curative treatment modalities are hepatic resection, liver transplantation and locoregional ablation therapy. Unlike other solid gastrointestinal tumors, multiple treatments are administered to HCC patients, and treatment modalities are not hierarchical. They can be used interchangeably in the same patients. Although there are several guidelines for the treatment of HCC patients, they are limited to initial treatment. There is no study about how often and which treatment modalities are selected after initial therapy. Ignoring treatment modalities following initial treatment in HCC patients may lead to confusing results, as many studies that compared curative treatment modalities have demonstrated (1718). The re-treatment rate was much lower in patients who initially underwent curative treatments such as hepatic resection and local ablation therapy than in patients who received TACE, a palliative treatment. TACE was the most common re-treatment modality regardless of the initial treatment modality. In a significant proportion of HCC patients, re-treatment modalities were selected interchangeably with the first treatment modalities, regardless of whether they were curative or palliative treatments. This study demonstrated the overall pattern of re-treatments 3-4 years after initial treatment.
On analysis of sorafenib administration, we found that the majority of patients had received sorafenib in general or tertiary hospitals consistent with the institutional pattern of initial treatment; however, long-term follow-up was not possible. Most (70-90%) HCC cases are known to involve underlying liver cirrhosis (19), but in the present report, only 25% and 31% of HCC cases were accompanied by liver cirrhosis in 2011 and 2012, respectively. The lower rate is believed to be because of the enrolled patients’ criteria, as unlike other studies, only Child Pugh-A patients were enrolled in this study. The majority of patients received the recommended initial dose (800 mg) and mean daily dose (about 680 mg) of sorafenib. Thus, the majority of Korean physicians have tried to administer the recommended dose during HCC treatment. The median treatment duration in our study was relatively shorter than that in Child-Pugh A patients, as reported in the final analysis of the global investigation of therapeutic decisions in HCC and of its treatment with sorafenib (20). This can be explained by a limited follow-up period in our study.
There are some limitations to this population-based study. First, the HIRA database provided limited information about the patients. Because the available data are age, gender, year, diagnostic code, procedure code, and medication code, we could not identify associated diseases and treatment methods, such as combination treatment, accurately by reviewing medical records. It is possible that clinicians had missed final diagnosis records such as underlying disease or extrahepatic metastasis sites. Second, the incidence of HCC may have been overestimated. Cases for 5 years (January 2008-December 2012) were obtained from the HIRA database. Although we excluded the same patient prior to the patient`s registration during the study period, we could not isolate the first diagnosed patients accurately, because the 5-year overall survival rate of HCC is greater than 20%.
Even though we could not identify the patterns of re-treatment accurately and sequentially due to these limitations, our study may highlight the current situation of HCC treatment. There are no data on re-treatment trends after initial treatment or for the entire population. Therefore, our study may provide new insights regarding the patterns and trends of HCC treatment.
 XML Download
XML Download