

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Human papillomavirus (HPV) is the most common sexually transmitted pathogen and is the cause of various urogenital cancers (12). Approximately 60 HPV genotypes are known to infect the genital tract and at least 13 of these are considered ‘‘high-risk’’ or oncogenic (13). Although infection is mostly transient and asymptomatic, oncogenic genotypes of HPV are related with cervical cancer development and other urogenital cancers in both men and women (4). Meanwhile, low-risk HPV types cause genital warts and other benign lesions (5). HPV co-infection or sequential infections with multiple HPV types reportedly synergistically increase the risk of cervical cancer (6). Patients infected with multiple HPV types require intensive care to prevent cancer progression and death, which indicates that monitoring the genotype and quantity of HPV may provide critical information in the diagnosis of infections for future patient management and prognosis (7).
The advance of helpful prophylactic vaccines against HPV types 16 and 18 has significantly foremost the prevention of cervical cancer, the second most common cancer in women worldwide (89). Moreover, there has been increasing interest in expansion HPV vaccination to men, in whom genital warts and oropharyngeal, penile, and anal cancers are also symptoms of HPV infection (1011). Therefore, full HPV genotyping is not only useful clinically to identify patients with type-specific high-risk HPV infections that confer a higher risk of cancer progression, but also to identify patients in whom vaccination is an effective prevention. The Anyplex II HPV28 Detection kit is designed for HPV genotyping and quantitation to meet the current demands for HPV detection. It simultaneously detects 19 high-risk HPV types (types 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 69, 73, and 82) and 9 low-risk HPV types (types 6, 11, 40, 42, 43, 44, 54, 61, and 70) from a single specimen using Tagging Oligonucleotide Cleavage and Extension (TOCE) technology.
Moreover, although genital HPV infections have been extensively studied in different groups of women, HPV infection in men is still not fully understood (1213). Further understanding of male HPV infection is necessary to prevent infection in men, as well as transmission to women. In our current study, we investigated the patterns of HPV infection and genotype distributions in male genital warts using Anyplex II HPV28 Detection.
MATERIALS AND METHODS
Study participants
The medical records of 80 male patients who presented to the 5 neighborhood clinics of Ulsan, Korea, between April 2014 and January 2015 for the treatment of genital warts were reviewed. All patients underwent HPV genotyping using Anyplex II HPV28 Detection. The following information on patterns of HPV infection was retrieved from the medical records of all patients: age, lesion location, methods of sample acquisition, types of HPV, and history of HPV. Multiple HPV infection was defined as co-infection with 2 or more types of HPV. Based on the type of HPV, patients were divided into 3 groups: no HPV infection, low-risk HPV infection, and high-risk HPV infection.
Collection of biologic samples
The collection of exfoliated genital cells from patients was performed by surgical excision of tissue or by cytobrush scratching. The cytobrush was moistened with phosphate-buffered saline and used to brush the penis, in a continuously rotational movement, from bottom to top, starting at the middle third of the scrotum. After retraction of the prepuce (in uncircumcised males), the coronal sulcus, the glans, and the tip of the penis also were brushed. The brush was cut and placed in a tube containing 5 mL of phosphate-buffered saline. Finally, a premoistened Dacron swab was gently rotated into the urethral opening and was placed in the same tube.
DNA extraction, HPV detection and genotyping
Nucleic acids were extracted from a 400 µL sample using the MICROLAB STARlet automated purification system (Hamilton, Reno, NV, USA). HPV detection and genotyping were performed according to the manufacturer’s instructions using the Anyplex II HPV28 kit and a CFX96 real-time thermocycler (Bio-Rad, Hercules, CA, USA). TOCE technology (Seegene, Seoul, Korea) is a novel approach that enables the detection of multiple targets in the same fluorescence channel of real-time PCR instruments using 2 components, “Pitcher” and “Catcher”. Taq polymerase extends from a target specific primer and encounters the target-bound Pitcher, which is cleaved by 5’ nuclease activity, releasing the Tagging portion. The sequence of the released Tagging portion is complementary to the capturing portion of the Catcher. TOCE assay uses a predetermined target sequence specific to the Catcher, enabling predictable analysis of the melting temperature of the Catcher duplex and providing multiplex real-time PCR capability to HPV28. In addition to amplification of the L1 gene of HPV DNA, the human housekeeping gene (human beta-globin) was simultaneously co-amplified as an internal control to monitor DNA purification efficiency, PCR inhibition, and cell adequacy. The thermal cycler conditions consisted of an initial incubation at 50℃ for 4 minutes to activate the uracil DNA glycosylase system in order to prevent contamination and denaturation at 95℃ for 15 minutes, followed by 50 cycles of denaturation at 95℃ for 30 seconds, annealing at 60℃ for 1 minute, and elongation at 72℃ for 30 seconds. The fluorescence was measured continuously as the temperature increased.
The Anyplex II HPV28 consists of 2 sets: the A set has 14 high-risk types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) and the B set covers 5 high-risk and 9 low-risk types (26, 53, 69, 73, 82, 6, 11, 40, 42, 43, 44, 54, 61, and 70). In addition, knowledge of the step at which the melting curve becomes positive allowed us to semiquantify the viral load, from low (+; positive after 40 PCR cycles), to intermediate (++; positive within 31 to 39 cycles), to high (+++; positive before 31 cycles). HPV28 thus semiquantitatively distinguishes 28 HPV genotypes. Data recording and interpretation were automated with the Seegene viewer software according to the manufacturer’s instructions.
Statistical analysis
The 3 study patient groups were compared using the χ2 test or the Fisher-Freeman-Halton test for categorical variables and the Kruskal-Wallis test for continuous variables. Quantitative data were expressed as mean ± standard deviation. The patterns of HPV infection according to age were also assessed. All statistical tests were 2-sided, with P < 0.05 considered significant. Data were analyzed using IBM SPSS Statistics Version 21 (IBM Corporation, Somers, NY, USA).
RESULTS
The descriptive characteristics of the 80 study patients are shown in Table 1. Of these patients, there were 13 (16.3%) whose specimens were negative for HPV infection, while 46 (57.3%) were infected with low-risk HPV, and 21 (26.3%) were infected with high-risk HPV. The mean age of all patients was 35.4 years and there were few differences among the groups. Although most of the samples were obtained from the penile shaft (75.0%), samples obtained at the urethra were more likely to have high-risk HPV infection (P = 0.017). Patients with multiple HPV infection were also more likely to have high-risk HPV infection (P = 0.001). The prevalence of HPV infection was much higher in samples obtained by tissue excision due to a definite lesion (P = 0.001). Infection recurrence was found in 34 patients (42.5%) at diagnosis, mostly of high-risk HPV infection.
Table 1
Characteristics of study cohorts according to oncogenic risk

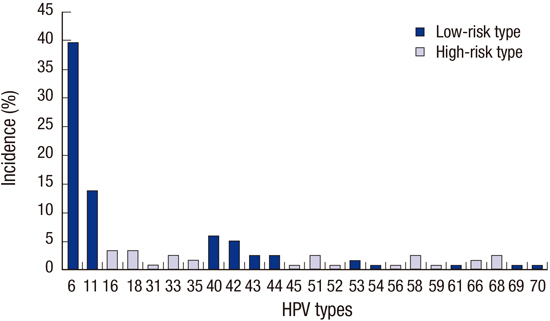
The patterns of HPV infection according to age are shown in Table 2. There were no differences in high-risk HPV infection (P = 0.459), multiple HPV infection (P = 0.185), and recurrence at diagnosis (P = 0.178) according to age. Type-specific infections by genotyping are shown in Fig. 1. HPV-6 and HPV-11 were the most common type detected overall (39.7% and 13.8%, respectively). HPV-16 and HPV-18 were the most common high-risk HPV infections (both 3.4%).
Table 2
Patterns of HPV infection according to age

DISCUSSION
Several research have reported estimates of HPV prevalence among men; however, these estimates range widely from 10% to 70% (14). Significant differences to the synthesis and interpretation of these studies are the discordance of sampling techniques used, the diversity and combinations of sites and specimens sampled, and the different HPV types tested. Moreover, few studies have assessed HPV prevalence in men with genital warts. In our present study, 67 (83.7%) of the 80 men with genital warts were infected with HPV. This rate is much greater than that observed previously in asymptomatic men recruited from the general population (15). Our current findings suggest that patients with genital warts should undergo HPV testing. Also, the relatively high rate of HPV prevalence in men with genital warts might be attributable to several features of HPV. Low-risk HPV types were the main causes of genital warts and patients with genital warts have been shown to also have a HPV co-infection or sequential infections of multiple HPV types.
The presence of multiple HPV types was found previously to be the most important risk factor for subsequent acquisition of a new HPV type, recurrence, and cancer progression (612). Although it has been hypothesized that the acquisition of one HPV type facilitates the acquisition of another type by some yet unknown biological mechanism, it is important that these HPV-positive men who acquired a new type were more likely to acquire multiple HPV types than HPV-negative men who acquired HPV during follow-up. This was especially evident for the high-risk HPV infection in our current study. Among all of our present patients, 32 cases (40%) had multiple HPV infection and all of the 21 patients with high-risk HPV infection had multiple HPV infection. In addition, the incidence of multiple HPV infection varies and is related to the method of HPV detection. In previous reports, the rate of multiple HPV infection in men ranged from 10% to 20% (1516). These differences may be due to the type of sample and the molecular techniques used for HPV detection. In our current analyses, most of the samples were obtained via tissue excision due to a definite lesion and HPV infection was assessed by multiplex real-time PCR. Given the dangers of multiple HPV infection and co-infection or sequential infections of HPV, genotyping is necessary to determine the appropriate treatment.
HPVs are subdivided into low-risk and high-risk variants based on the potential for oncogenesis. Genital warts are caused by the low-risk types of HPV (6, 11, 42, 43, and 44) with 90% of these cases caused by 2 genotypes, HPV-6 and HPV-11 (17). In contrast, high-risk HPVs cause cervical carcinomas and urogenital cancers. One study has shown that 31% of adults suffering from carcinoma are co-infected with a high-risk HPV (18). In our present study, HPV-16 and HPV-18 were the most common causes of high-risk HPV infections. Few data on HPV-16/-18 prevalence are available among men for whom current HPV prophylactic vaccines are approved (101116). These data would be useful to estimate the proportion of men positive for both HPV-16/-18 and who thus may obtain optimal benefits from HPV vaccination. This also supports efforts to extend HPV vaccination to men.
HPV prevalence might be high among sexually active young men and women because it is one of the most common sexually transmitted infections worldwide (2). However, global data on the age-specific prevalence of HPV infection in males show a more stable HPV prevalence by age in men than in women (19). These data also show similar age-related trends across major regions. Similarly, there were no differences in the patterns of HPV infection such as high-risk HPV infection and multiple HPV infection according to age in our current study series. Therefore, HPV testing is necessary for genital wart treatment, regardless of age.
The anatomical sites and genotyping methods used for HPV detection have varied across different studies and may have contributed to the observed differences among men in these reports (2021). In our current study, most of the samples were obtained at the penile shaft (75.0%). These findings emphasized the importance of the penile shaft as a site of HPV infection in men, as well as being a site with the most potential for HPV transmission during sexual intercourse. In addition, our finding that samples obtained at the urethra were more likely to have high-risk infection suggests that men with genital warts should undergo urethral examination. Comparisons of HPV prevalence among studies are also hampered by differences among the study populations surveyed, laboratory methods used, and HPV types analyzed. To reduce possible underestimation of overall or type-specific prevalence, we used the Anyplex II HPV28 Detection multiplex real-time PCR assay. Although this assay has a relatively higher sensitivity for HPV detection than earlier detection assays, the sensitivity of HPV detection presented by our present data might have been optimal if the chosen type-specific PCR primers included typing for only a relatively small number of HPV types (2223).
Our present study findings were limited by the retrospective nature of our analyses, our relatively small study cohort, and the significant differences among the patients in terms of several clinical variables. Second, our data were limited to cross-sectional prevalence, rather than the identification of persistent HPV infection, which has been shown to be highly predictive of the future risk of cancer (24). Moreover, we did not evaluate the treatment outcomes or the prognosis. Finally, the current study represents patients from six institutions in Ulsan, Korea; therefore, differences in technique and decision-making are possible. Furthermore, our findings may have resulted from limitations in the regional case study. Lager studies including a broader region, applying HPV detection at several time points, are needed to confirm our study. Nonetheless, our report is the meaningful study to analyze the patterns of HPV infection and genotype distributions in male genital warts using the Anyplex II HPV28 Detection kit. Above all, a wide range of ages was enrolled in our current study. Also, we found that multiple HPV infection is associated with high-risk infection which is most important risk factor for subsequent acquisition of a new HPV type, recurrence, and cancer progression.
In conclusions, HPV infection is not only commonly encountered in male genital warts, but is also accompanied by high-risk HPV and multiple infections. There are no differences in patterns of HPV infection according to age. Although HPV-16/-18 infections, which can cause urogenital cancer, are the most common high-risk HPV infections and no current antiviral therapy exists, prophylactic vaccines for HPV-16/-18 have been approved. HPV genotyping, regardless of age, is therefore a logical first step in the clinical strategy to avoid or minimize potential HPV-related carcinogenesis and harm from male genital warts. However, our present study cohort was relatively small and further studies are needed to fully determine the prognosis of HPV infection.
 XML Download
XML Download