

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Intussusception is a common cause of acute intestinal obstruction in young children, and it is rarely associated with pathological lesions. However, chronic intussusception is a rare childhood disease that is more commonly accompanied by leading points, such as polyps or neoplasms, and should be treated surgically (12). The clinical triad of colicky intermittent abdominal pain, vomiting, and bloody stool in acute intussusceptions is observed only in a few patients with chronic intussusceptions (1). Chronic intussusception is associated with increased mortality (1234). Here, we report a case of chronic intussusception with intestinal lymphoma that presented as abdominal pain and constipation for 2 months. Based on our experience, a high index of suspicion is vital for diagnosing chronic intussusception.
CASE DESCRIPTION
On May 23, 2014, a 6-year-old female visited our outpatient clinic complaining of recurrent abdominal pain and constipation for 2 months. The pain occasionally interrupted her sleep and had reduced her appetite. Several primary physicians had examined her, and the symptoms were relieved with the use of antispasmodic and probiotics. Three days before visiting our clinic, she had been admitted to the emergency room for non-bilious vomiting and worsening abdominal pain. After simple abdominal radiographs showed mild ileus in the lower abdomen (Fig. 1), an evacuation enema relieved her symptoms, with the expulsion of feces and gas. She was discharged from the emergency room, and given an outpatient appointment.
Fig. 1
Plain abdominal radiographs taken in the emergency room 3 days before visiting the outpatient clinic showed mild to moderate ileus without definite mechanical obstruction. (A) Erect view. (B) Supine view.

On physical examination, she looked fatigued, but showed no sign of significant weight loss. She was 116 cm tall (50th percentile) and weighed 20 kg (25th percentile). On palpation, her abdomen was distended mildly, with tenderness in the right upper quadrant. There was no hepatosplenomegaly or peripheral lymph node enlargement. Laboratory tests included the following: white blood cells 14,000/µL (segmented neutrophils 94%, lymphocytes 4.0%, monocytes 2.0%, eosinophils 0%, basophils 0%), hemoglobin 12.2 g/dL, and platelets 423,000/µL. The serum chemistry was within normal limits, except a C-reactive protein of 0.87 mg/mL (normal < 0.5 mg/mL).
Ultrasonography (Fig. 2) revealed an ileocolic-type intussusception that contained crescent-shaped hypoechoic spots, suspected to be the leading cause, and enlarged mesenteric lymph nodes. Abdominal computed tomography revealed an ileocolic-type intussusception with 3-cm, crescent-shaped, low-density lesions at the top of the intussusceptum and small lymph nodes along the intussusception (Fig. 3).
Fig. 2
Abdominal ultrasonography of the right upper abdomen. (A) An ileocolic-type intussusception was found with a crescent-shaped hypoechoic portion (arrows). (B) Enlarged lymph nodes (*) along the intussusceptions.

Fig. 3
Abdominal computed tomography. (A) A 3-cm, crescent-shaped (arrow), low-density lesion at the top of the intussusception. (B) Ileocolic-type intussusception (arrow).

After the failure of air reduction, laparoscopic exploration of the abdomen and reduction of the intussuscepted bowel were attempted. At laparoscopic exploration of the abdomen, the intussuscepted bowel was seen in the right upper quadrant of the abdomen, immediately proximal to the hepatic flexure of the large bowel. Grossly, no ischemic change of the intussuscepted bowel was observed and the appendix appeared normal (Fig. 4). Laparoscopic instruments were used to drain the intussuscepted bowel several times, in an attempt to reduce it. However, laparoscopic reduction was unsuccessful because a tight, fibrous adhesion was present around the ileocecal valve and proximal cecum, where the main part of the bowel intussusception was located.
Fig. 4
Laparoscopy view showing the intussusception. Distal ileum (a) is pulled into ascending colon (b), forming ileocolic type intussuception (arrow).

The procedure was converted to open manual reduction. Through a transverse incision of the right side of the abdomen, the intussusceptum was extracted from the abdomen. The inside of the normal large bowel should normally slide easily over the intussusceptum. In this case, however, the intussuscepted bowel had formed a hard mass, and the serosa was thickened at the severely folded ileocecal junction. Manual reduction was impossible because a hard, fibrous adhesion had formed between the strongly impacted ileum and cecum. The affected bowel was resected and an ileocolic anastomosis was performed. The resected bowel specimen showed a 5 × 4-cm lesion in the terminal ileum. Histopathologically, it showed features of diffuse large B-cell lymphoma (Fig. 5). The isolated mesenteric lymph nodes were reactive, without lymphoma-like findings. The serosa and submucosa showed chronic fibrosis. The postoperative recovery was uneventful. She was discharged on the seventh postoperative day, with good bowel movements and was referred to the cancer center for further management.
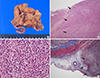
Fig. 5
Gross and microscopic findings of the resected tissue. (A) Gross view of the formalin-fixed hemicolectomy specimen including ileum, cecum and appendix showing an ill-defined ulcerative lesion (arrow), measuring 5.5 × 4.0 cm. (B) The terminal ileum shows ulceration with diffuse tumor cell infiltration (arrow) in the mucosa and proper muscle layer in a low-magnification view (H&E stained, × 20). (C) The tumor cells have large vesicular nuclei with prominent nucleolus and thick nuclear membrane (H&E stained, × 400). (D) The subserosa and serosa of the terminal ileum show fibrosis and chronic inflammatory cell infiltration (arrow) admixed with tumor cell infiltration (Masson trichrome stained, × 20).
DISCUSSION
In recent literature reviews, cases reported between 1972 and 2007 indicate that chronic intussusceptions more frequently involve leading points, especially in children older than 2 years, and the classical triad of colicky abdominal pain, vomiting, and passage of blood through the rectum was absent at the time of diagnosis. Furthermore, 80% of the patients had abdominal pain or vomiting (1). Our patient had only a 2-month history of abdominal pain and constipation with transient vomiting; therefore, we could not determine when the intussusception occurred. The finding of a tight, fibrous adhesion around the intussusception, and microscopic submucosal and serosal fibrosis suggest that her condition was not the result of recent events.
Chronic intussusception is a rare disease that can follow repeated episodes of subacute intestinal obstruction without strangulation. A partially maintained blood supply through another mesenteric artery may allow the intussusception to remain viable in a chronic state in older children. We believe that our patient underwent repeated subacute intussusceptions with collateral circulation via other mesenteric arteries (2). Lymphoma as a leading point is often reported in childhood, causing acute intussusception with abdominal pain and passage of blood through the rectum (567). Few cases of chronic intussusception with lymphoma accompanied by a palpable mass and abnormal blood findings have been reported.
Diffuse large B-cell lymphoma is the most common non-Hodgkin’s lymphoma in adolescents, and manifests as either abdominal or primary mediastinal lymphoma (34). In children, recurrent abdominal pain is occasionally considered a functional disorder in the absence of alarming symptoms such as significant vomiting, fever, diarrhea, and weight loss or delayed growth, without an imaging or laboratory work-up. The intussusception in this patient progressed slowly, with no definite signs or symptoms of intestinal obstruction. Therefore, a careful examination and a high index of suspicion when chronic abdominal pain is present could decrease the mortality due to this disease.
 XML Download
XML Download