

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Disseminated intravascular coagulation (DIC) is characterised by thrombotic occlusion and bleeding (12). Although the diagnosis of DIC is important for patients in the medical intensive care unit (ICU), no single laboratory test with satisfactory performance for the accurate diagnosis of DIC is currently available (3). Currently, the most commonly used diagnostic criteria for DIC are the International Society on Thrombosis and Haemostasis (ISTH) criteria, the Japanese Association for Acute Medicine (JAAM) criteria and the Japanese Ministry of Health and Welfare (JMHW) (4). In 1993, the Korean Society on Thrombosis and Hemostasis (KSTH) also developed diagnostic criteria for DIC (5). However, the performance of KSTH diagnostic criteria has not yet been validated and not accepted as commonly used DIC diagnostic criteria.
Although previous studies showed that the Japanese criteria (JAAM and Revised-JAAM [R-JAAM]) possess higher sensitivity than both ISTH and JMHW criteria (67), these studies have some statistical bias such as overlap of subgroup that the DIC patients diagnosed from JAAM and R-JAAM criteria included the majority of DIC patients diagnosed from the ISTH criteria. Several studies also evaluated the prognostic impact of various DIC criteria based on the acute physiology and chronic health evaluation (APACHE) II score, the sequential organ failure assessment (SOFA) score, and mortality (78910). However, most of these studies included heterogeneous patient cohort and few studies addressed the prognostic impact of various DIC diagnostic criteria in specific patient subgroup with severe sepsis and septic shock. In the present study, we aimed to compare the performance of five DIC diagnostic criteria focused on the mortality prediction as an outcome parameter in patients with severe sepsis or septic shock, while including the KSTH criteria.
MATERIALS AND METHODS
Patient selection
Patient records and information was anonymized and de-identified prior to analysis. Among patients with severe sepsis or septic shock admitted to the medical ICU from May to August 2012, only patients in whom the routine DIC laboratory tests (platelet, D-dimer, fibrin/fibrinogen degradation product [FDP], prothrombin time [PT], activated partial thromboplastin time [aPTT], and fibrinogen) during the first consecutive 4 days after admission were performed, were enrolled in the present study. Patients with Child Pugh grade C liver cirrhosis, hematologic diseases, medication such as anticoagulant therapy or chemotherapy, and age younger than 20 years old were excluded from the present. Finally, total 100 patients with severe sepsis or septic shock were included in the present study.
Collection of clinical data and sample acquisition of patients
Electronic medical records were reviewed and basic demographic data including age, gender, use of continuous renal replacement therapy (CRRT), ventilator use, blood culture, and initial vital signs were obtained retrospectively, and both APACHE II and SOFA scores were calculated. Peripheral blood samples of enrolled patients were collected within 2 hours of admission to the ICU (Day 1) and at consecutive three days (Day 2–4), with the interval of 24 hours. Routine DIC diagnostic tests mentioned above were performed with all samples obtained. The samples for laboratory tests were blindly transferred to laboratory room without clinical information.
Definitions of criteria used in the patient classification
Systemic inflammatory response syndrome (SIRS) score was calculated according to the general SIRS guideline. Sepsis was defined as the presence (probable or documented) of infection together with systemic manifestations of infection (general variables, inflammatory variables, hemodynamic variables, organ dysfunction variables, and tissue perfusion variables). Severe sepsis was defined as sepsis plus sepsis-induced organ dysfunction or tissue hypoperfusion (sepsis-induced hypotension, lactate above upper limits laboratory normal, urine output < 0.5 mL/kg/hr for more than 2 hours despite adequate fluid resuscitation, acute lung injury with PaO2/FiO2 < 250 in the absence of pneumonia as infection source, acute lung injury with PaO2/FiO2 < 200 in the presence of pneumonia as infection source, creatinine > 2.0 mg/dL, bilirubin > 2 mg/dL, platelet count < 100,000/μL, INR > 15). Finally, septic shock was defined as sepsis-induced hypotension persisting, despite adequate fluid resuscitation. Hypotension was defined by a systolic arterial pressure below 90 mmHg, a mean arterial pressure < 70 mmHg, or a reduction in systolic blood pressure of > 40 mmHg from baseline (11). The clinical severity of each patient was evaluated according to the APACHE II and SOFA scores.
Comparison of baseline clinical and laboratory characteristics between survivors and non-survivors
The diagnosis of DIC based on the ISTH, JAAM, revised JAAM, JMHW and KSTH criteria which are summarized in Table 1, were done separately at each four consecutive days (day 1–4) in each patient using data obtained at that day. All patients were categorized into survivors and non-survivors according to the estimation at the final follow-up time period (overall ICU and 28-day mortality). Both clinical and laboratory characteristics obtained at Day 1 (baseline) were compared between two patient subgroups in the Table 2.
Table 1
Summary of five different DIC diagnostic criteria applied in the present study
R-JAAM criteria have same score system with JAAM except fibrinogen score.
aPTT = activated partial thromboplastin time, DIC = disseminated intravascular coagulation, FDP = fibrin/fibrinogen degradation product, ISTH = International Society on Thrombosis and Haemostasis, JAAM = Japanese Association for Acute Medicine, JMHW = Japanese Ministry of Health and Welfare, KSTH = Korean Society on Thrombosis and Hemostasis, PT = prothrombin time, R-JAAM = Revised JAAM, SIRS = systemic inflammatory response syndrome.
*D-dimer < 1.0; †D-dimer ≥ 1.0; ‡1.0 ≤ D-dimer < 5.0; §D-dimer ≥ 5.0; ‖FDP < 10; ¶10 ≤ FDP < 25; **FDP ≥ 25.
Table 2
Comparison of baseline clinical and laboratory characteristics in total 100 patients between survivors and non-survivors

P values were obtained from the Pearson’s χ2 test (for dichotomous variables) and the Mann-Whitney U test (for continuous variables) and the results were expressed as the median and interquartile range (IQR, 25th–75th percentile).
APACHE = acute physiology and chronic health evaluation, aPTT = activated partial thromboplastin time, CNS = central nervous system, CRRT = continuous renal replacement therapy, F = female, FDP = fibrin degradation product, GI = gastrointestinal, GU = genitourinary, M = male, MS = musculoskeletal, PT = prothrombin time, SOFA = sequential organ failure assessment.
Evaluation of distribution characteristics in patients diagnosed as DIC according to five different diagnostic criteria
The number of patients diagnosed with DIC according to the five DIC diagnostic criteria was evaluated separately during 4 days mentioned above. When five different DIC diagnostic criteria were applied separately, the distribution characteristics of patients diagnosed as DIC at each day and in overall period (defined as from day 1 to day 4) were analysed. These results are summarized in the Table 3.
Table 3
Distribution characteristics of patients diagnosed as DIC according to five different diagnostic criteria

The number indicates the number of patients who were newly diagnosed on each day.
DIC = disseminated intravascular coagulation, ISTH = International Society on Thrombosis and Haemostasis, JAAM = Japanese Association for Acute Medicine, R-JAAM = Revised JAAM, JMHW = Japanese Ministry of Health and Welfare, KSTH = Korean Society on Thrombosis and Hemostasis.
*P value < 0.001.
Performance of five different DIC diagnostic criteria in the prediction of overall ICU and 28-day mortality
Multivariate logistic regression analysis and receiver operating characteristics (ROC) analysis were performed to estimate prognostic impact of five different DIC diagnostic criteria diagnosed at Day 1 and overall period in the prediction of overall ICU mortality. In addition, the sensitivity, specificity, negative predictive value, positive predictive value, and accuracy of five different DIC diagnostic criteria diagnosed at Day 1 and overall period in the prediction of overall ICU mortality were analysed. Finally, the 28-day mortality of patients with DIC diagnosed by each set of five different DIC diagnostic criteria at Day 1 and overall period, were analysed and compared using a Kaplan-Meier survival analysis.
Statistical analysis
The normality of the data distribution was evaluated using the Kolmogorov-Smirnov test. All continuous variables were expressed as the median (with 25th–75th percentile) because they did not show normal distribution. Comparison of categorical and continuous variables were performed using the χ2 test (or Fisher’s exact test for small number less than 5 in each subgroup) and the Mann-Whitney U test, respectively. Prognostic impact of five different DIC diagnostic criteria for the prediction of mortality were evaluated using multivariate logistic regression analysis, ROC analysis and Kaplan-Meier curve analysis. For all comparisons, tests were two-tailed and P values < 0.05 were regarded as statistically significant. SPSS 18.0.0 software for Windows (SPSS, Inc., Chicago, IL, USA) was used for all statistical analyses.
Ethics statement
The present study was approved by the institutional review board of the Asan Medical Center for conducting a pilot study for the performance evaluation of five DIC diagnostic criteria, focusing on mortality as an outcome parameter (IRB 2012-0500). Due to the purely observational, retrospective, and non-interventional nature of this study, informed consent was deemed unnecessary and was not obtained.
RESULTS
Comparison of baseline clinical and laboratory characteristics between survivors and non-survivors
The non-survivors showed significantly higher incidence of ventilator use (P = 0.005), a higher APACHE II score (P = 0.049) and a faster heart rate (P = 0.031) than the survivors. Comparison of baseline coagulation markers between the survivors and non-survivors demonstrated that the non-survivors show lower platelet count (P < 0.001), lower fibrinogen level (P = 0.047), lower antithrombin III level (P = 0.019), more prolonged PT (P = 0.045) and aPTT (P = 0.030) than the survivors (Table 2).
Evaluation of distribution characteristics in patients diagnosed as DIC according to five different diagnostic criteria
During the overall period, the number of patients diagnosed as DIC according to the JAAM and R-JAAM criteria (69 and 74 patients, respectively) was 1.5-fold greater than the number of patients diagnosed as DIC according to the KSTH and ISTH criteria (47 and 46 patients, respectively). For the early diagnosis of DIC (on Day 1), the number of patients diagnosed as DIC according to the JAAM and R-JAAM criteria (55 and 62 patients, respectively) was 2-fold greater than the number of patients diagnosed as DIC according to the KSTH and ISTH criteria (29 and 32 patients, respectively). Satisfactory agreement (kappa = 0.76, P < 0.001) regarding the diagnosis of DIC between the ISTH and KSTH criteria was observed in 88 patients. The patients group diagnosed as DIC according to the JAAM and R-JAAM criteria on overall period included all patients diagnosed as DIC according to the KSTH, JMHW and ISTH criteria (Table 3).
Multivariate analysis of five different DIC diagnostic criteria applied at Day 1 and overall period in the prediction of overall ICU mortality
Multivariate logistic regression analysis revealed that after adjusting for the APACHE II score, SOFA score, CRRT use, ventilator use, heart rate, and antithrombin III level, only the KSTH and JMHW criteria possess independently significant prognostic value in the prediction of overall ICU mortality when applied at day 1 after admission (odds ratio [OR] 3.828 and 5.181, P = 0.018 and 0.006, 95% confidence interval [CI] 1.256–11.667 and 1.622–16.554, respectively) (Table 4). Identical analysis also showed that only the KSTH and JMHW criteria possess independently significant prognostic value in the prediction of overall ICU mortality when the results of overall periods are integrated (OR 4.588 and 4.690, P = 0.007 and 0.014, 95% CI 1.521–13.841 and 1.368–16.085, respectively).
Table 4
Multivariate analysis of five different DIC diagnostic criteria applied at Day 1 in the prediction of overall ICU mortality
Performance of five different DIC diagnostic criteria in the prediction of overall ICU and 28-day mortality
ROC analysis showed higher AUC value of both KSTH and JMHW criteria in the prediction of overall ICU mortality when applied at Day 1 (area under the curve [AUC] 0.687 and 0.699, P = 0.003 and 0.002, 95% CI 0.568–0.806 and 0.589–0.808, respectively) and overall periods (AUC 0.744 and 0.711, P < 0.001 and 0.001, 95% CI 0.640–0.848 and 0.606–0.815, respectively) than ISTH (AUC 0.619 and 0.681, P = 0.058 and 0.004, 95% CI 0.496–0.741 and 0.567–0.795, respectively), JAAM (AUC 0.616 and 0.678, P = 0.065 and 0.005, 95% CI 0.498–0.733 and 0.572–0.783, respectively), and R-JAAM criteria (AUC 0.612 and 0.642, P = 0.075 and 0.024, 95% CI 0.495–0.728 and 0.532–0.751, respectively). In addition, both KSTH and JMHW criteria showed comparable or higher accuracy in the prediction of overall ICU mortality when applied at Day 1 as well as when applied at overall periods compared to other three criteria (Table 5).
Table 5
Performance of five different DIC diagnostic criteria in the prediction of overall ICU mortality when applied at Day 1 and overall period

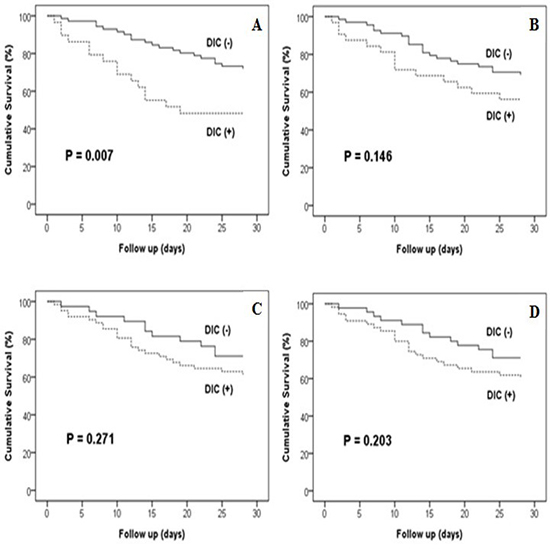
Subsequently performed Kaplan-Meier survival curve analysis showed that both KSTH and JMHW criteria are statistically significant in terms of predicting 28-day mortality when applied at Day 1 and overall period (P = 0.007 and P = 0.012, respectively vs. P = 0.049 and P = 0.014, respectively) (Fig. 1). The JAAM criteria were statistically significant for the prediction of 28-day mortality only when applied at overall period (P = 0.010).
Fig. 1
Comparison of five different DIC diagnostic criteria in terms of predicting 28-day mortality when applied at Day 1. Kaplan-Meier survival curve analysis shows that the KSTH (A) and JMHW (E) criteria could significantly predict 28-day mortality when applied at Day 1. However, ISTH (B), JAAM (C) and R-JAAM (D) criteria could not significantly predict 28-day mortality when applied at Day 1.
ISTH = International Society on Thrombosis and Haemostasis, JAAM = Japanese Association for Acute Medicine, JMHW = Japanese Ministry of Health and Welfare, KSTH = Korean Society on Thrombosis and Hemostasis, R-JAAM = revised JAAM.
DISCUSSION
We compared the ability of five sets of DIC diagnostic criteria, including the non-validated KSTH criteria, to predict overall ICU and 28-day mortality in patients with severe sepsis or septic shock. Our present study showed that both KSTH and JMHW criteria possess superior performance than the ISTH, JAAM and R-JAAM criteria in the prediction of overall ICU and 28-day mortality.
Several guidelines for the diagnosis of DIC were published. Di Nisio et al. (4) recommended the use of the ISTH, JMHW or JAAM criteria. Levi et al. (3) used ISTH criteria and evaluated mortality to judge the efficacy of the DIC criteria. On the other hand, Wada et al. (1213) recommended the JAAM criteria while emphasizing the importance of early diagnosis and treatment. Although the KSTH DIC scoring system has the advantage of being concise and relatively easy to use for calculations without a weighted score, the KSTH criteria are currently not accepted as an international diagnostic method due to a lack of clinical application data. However, a previous study compared the KSTH criteria and ISTH criteria, and reported a K-coefficient of 0.78 (6). Moreover, a study by Lee et al. (5) reported a concordance rate of 84.7% and K-coefficient of 0.6 between the ISTH criteria and KSTH criteria, and concluded that the KSTH criteria is more sensitive predictor of mortality than the ISTH criteria. In the present study, we found a similar concordance rate (88.0%) and K-coefficient (0.76) which is higher than the earlier reported concordance rate for the ISTH/JMHW criteria (67.4%) (14) and the ISTH/JAAM criteria (86.5%) (15).
The patient cohort in the present study who were diagnosed as DIC according to the ISTH, JMHW and JAAM criteria on day 1–4 showed a similar distributions to that reported previously. Gando et al. (67) and Hayakawa et al. (15) reported that the JAAM criteria is the most sensitive diagnostic criteria for the diagnosis of septic DIC, whereas the ISTH criteria are the most specific. Similarly, our present results showed that DIC cases diagnosed according to the JAAM criteria included all patients diagnosed as DIC according the KSTH, JMHW and ISTH criteria. However, our study showed higher incidence of DIC than result of Gando et al. (16) for patients with severe sepsis or septic shock (JAAM DIC 69% vs. 46.8%). We hypothesize that enrollment of patients having more severe severity in our present study may be attributable to this result (septic shock 70% vs. 45%, APACHE II score 24.7 vs. 23.2, SOFA score 10.5 vs. 8.5, respectively).
Many studies showed that these characteristics above mentioned of each DIC criteria are reflected by the extent of mortality. Gando et al. (6) reported that the prediction rates of mortality using the ISTH criteria (51.9%) and JMHW (50.0%) are higher than those predicted by the JAAM criteria (43.8%). Takemitsu et al. (17) reported a similar performance between these two sets of criteria in terms of predicting mortality. The mortality rates predicted by the ISTH, JMHW and JAAM criteria in that study were 40.6%, 35.5% and 31.7%, respectively. The sensitivity/specificity of the ISTH, JMHW and JAAM criteria for the prediction of mortality were 50.4%/71.4%, 51.3%/64.9%, and 80.0%/33.2%, respectively. Our present study showed similar results that both ISTH and JMHW criteria are more specific than the JAAM criteria in the prediction of overall ICU mortality. Our present study found the sensitivity/specificity of the ISTH, JMHW and JAAM criteria for predicting mortality as 48.4%/75.4%, 77.4%/62.3% and 71.0%/52.2%, respectively, when applied at Day 1.
Few studies have used logistic regression and ROC analysis to evaluate the DIC diagnostic criteria and mortality outcomes. Angstwurm et al. (10) analysed ISTH criteria for the prediction of mortality using the ROC analysis, and reported AUC of 0.735. Gando et al. (8) applied logistic regression analysis in the evaluation of the JAAM criteria on the prediction of mortality and reported OR of 1.223. Iwai et al. (9) reported that only the APACHE II score is independently associated with mortality (P < 0.001, OR 1.21); however, the JAAM criteria also showed a low, non-significant OR for the prediction of mortality after the removal of confounding factors (P = 0.066, OR 0.29). Recently, Gando et al. (16) reported that the JAAM criteria applied at day 1 (OR 1.282, P < 0.001) and the Delta JAAM DIC score applied at day 1 (OR 0.770, P < 0.001) are independent predictors of 28-day mortality in DIC patients with severe sepsis. In the present study, the delta DIC score did not predict ICU mortality significantly, but tended to reduce mortality when the delta score increases. However, our present study demonstrated that both KSTH and JMHW criteria applied on Day 1 and overall period significantly predicted the overall ICU mortality. Kaplan-Meier curve analysis also showed that the ability of the KSTH and JMHW criteria on Day 1 and overall period to predict 28-day mortality was significantly high.
The possible explanations for these results are as follows: first, fibrinogen is an acute phase protein increased during inflammatory responses. Therefore, in certain situation that DIC is accompanied by inflammation, we would expect that a decrease in fibrinogen levels in DIC can be masked by the increase of fibrinogen level due to inflammatory process. Bakhtiari et al. (18) reported that exclusion of fibrinogen level from the ISTH DIC score would not affect the accuracy of scoring system in the detection of DIC in critically ill patients. Gando et al. (7) made the R-JAAM criteria based on the little effect of fibrinogen level on the prediction of outcome in the DIC patients. However, Kim et al. (19) showed that the OR of the low fibrinogen level (< 1.0 g/L) is 2.13 (P = 0.024) and Gando et al. (16) reported that the fibrinogen is an independent predictor for 28-day mortality (OR 0.998, P = 0.033). The present study showed that fibrinogen on Day 1 transformed to nominal variable is an independent predictor for ICU mortality in univariable analysis. Especially, the KSTH criteria showed the best statistical significance (P = 0.007, OR 9.479, 95% CI 1.839–48.853).
Second, only the KSTH criteria included the aPTT as a variable. Our present study showed that the aPTT (P = 0.042, OR 1.024, 95% CI 1.001–1.048), D-dimer (P = 0.042, OR 1.037, 95% CI 1.001–1.075), and platelet (P = 0.002, OR 0.988, 95% CI 0.981–0.996) except PT (P = 0.083, OR 1.061, 95% CI 0.992–1.134) were risk factors for ICU mortality. In additional analysis using nominal variable of marker transformed by the KSTH criteria, aPTT was a more useful marker for ICU mortality than PT (P = 0.027, OR 2.705, 95% CI 1.121–6.527 vs. P = 0.286, OR 1.629, 95% CI 0.665–3.990, respectively) (data not shown). We assumed the reason for these results. First, a prolonged PT, which reflects the inhibition of hemostasis cascade from the release of tissue factor (extrinsic pathway), happens faster than a prolonged aPTT which is related to the inhibition of intrinsic pathway. Second, at the early stage of sepsis, factor VIII levels are likely to be increased because factor VIII is an acute phase reactant. As a result, the prolongation of aPTT may be masked by an increase in factor VIII levels in early sepsis patients with DIC. Kinasewitz et al. (20) and Kim et al. (19) reported that the abnormality rate in PT is hihger than that in aPTT (93.4% vs. 63.1% and 68.4% vs. 47.3%, respectively) for patients with sepsis. In conclusion, we suggest that PT is an early marker for the detection of DIC, and aPTT is a marker for the reflection of severity in DIC.
Our present study had certain limitations. First, our small sample size would be main limitation. We could not calculate appropriate sample size due to lack of previous study comparing DIC diagnostic criteria in the prediction of mortality in patients with severe sepsis or septic shock. Unavoidably, our present pilot study included small number of patients compared with other studies. Second, single center design for clarification and generalization of analysis results would be another limitations. More comprehensive and well-designed multicenter prospective study focused on this issue should be performed. Third, our present study limited study population as patients with severe sepsis or septic shock and possible selection bias may affect the study results. Especially, as previously discussed, it is needed to consider that our present study enrolled more severe septic patients. More comprehensive study in the DIC patients caused from other diseases should be required for the generalization of our present study results. In addition, although our present study showed higher AUC values of KSTH and JMHW criteria than other three criteria, AUC values of all five criteria were below 0.7, which may remain a concern that these level can be regarded as an adequate evidence of diagnostic value. Therefore, we suggest that clinicians should be warned not to predict prognosis entirely based on the DIC criteria.
In conclusion, our present study showed that both KSTH and JMHW criteria would be more useful than other three criteria in predicting prognosis in DIC patients with severe sepsis or septic shock, and more comprehensive study would be required for the confirmation of our present study results.
 XML Download
XML Download